0601
Convolutional neural network classification of axillary lymph node metastasis on MRI of breast cancer patients1Stony Brook University, Stony Brook, NY, United States, 2Columbia University, New York City, NY, United States
Synopsis
The majority of breast cancer metastasis spreads through the axillary lymph nodes. It is challenging to classify whether there is disease or no-disease axillary lymph nodes because they are small and cluster together. We implemented a convolutional-neural network for automatic classification of diseased versus non-diseased axillary lymph nodes by analyzing data from standard clinical breast MRI. Data were assigned randomly to 70/30 as training/validation set. The results showed the remarkable agreement with ground truths, with 86.7% accuracy. This approach may prove useful for automatically detecting lymph nodes metastasis on MRI in clinical settings in breast cancer patients.
Introduction
Axillary lymph node (aLN) staging is critically important in the prognosis and treatment planning of breast cancer. Current methods for aLN staging include sentinel biopsy, ultrasound, and FDG-PET. Sentinel biopsy is the standard of care but it is invasive, has comorbidity, and >70% of biopsied nodes are negative [2]. Ultrasound is cost-effective but has moderate accuracy and sensitivity in detecting node metastasis [3]. FDG-PET is an excellent marker for cancer but it is not routine for cancer imaging and has moderate accuracy and sensitivity. MRI staging of aLNs is challenging and generally unreliable because of small node size, and poor contrast with neighboring tissue.
Artificial intelligence has gained popularity for extracting radiomic features from diagnostic images. One common machine-learning algorithm is the convolutional neural network (CNN) [6]. CNN uses artificial neural network to automatically construct predictive statistical models by self-optimization through complex layers. To our knowledge there is only one report using CNN to evaluate aLNs in breast cancer patients [1].
We implemented a CNN algorithm for automatic classification of whether the aLNs had disease or not by using standard clinical breast MRI images. The ground truths were based on FDG-PET with confirmation of radiology reports and pathology reports.
Methods
This study included 150 aLNs from 42 neoadjuvant-chemotherapy breast cancer patients, with FDG-PET/CT and breast MRI (1.5T) data. The aLN were segmented on contrast-enhanced MRI (1x1x2mm). The aLNs were determined to have disease or no-disease from FDG-PET, with confirmation by pathology reports. Hyperintense aLN on FDG-PET were considered abnormal. Contralateral unaffected nodes and ipsilateral nodes with no FDG-PET hyperintensity were normal [5].
In this cohort, 46 nodes had diseases, and 104 nodes were normal. Data was separated randomly into 70/30 as training/validation set. Lymph nodes on MRI were manually segmented. To improve computational efficiency, we manually cropped the images to size 32x32x10 which were large enough to contain all aLNs. Using the machine learning frameworks Keras and TensorFlow, we built a biomedical image classification architecture consisting of a path that enabled precise classification. CNN consisted of four layers of complex convolutions as well as layers of max pooling and dropout. We trained this model using multi-slice images. This program was run on an NVIDIA Tesla K80 GPU.
Hyperparameters such as epochs, batch size, and optimizer were tuned to improve training. Batch size was reduced from 32 images to 10 so the program could run without crashing. The number of epochs was increased from 20 to 100 and the learning rate was increased from 0.0001 to 0.001 so the program could give more accurate predictions.
Area under the curve (AUC) of the receiver-operating curve was obtained as a measure of classification accuracy on the validation dataset.
Results
The speed metrics in our architecture were optimized with a high-learning rate to create an efficient system. The average learning rate per epoch was 9.88s. The final CNN parameters are shown in Table 1.
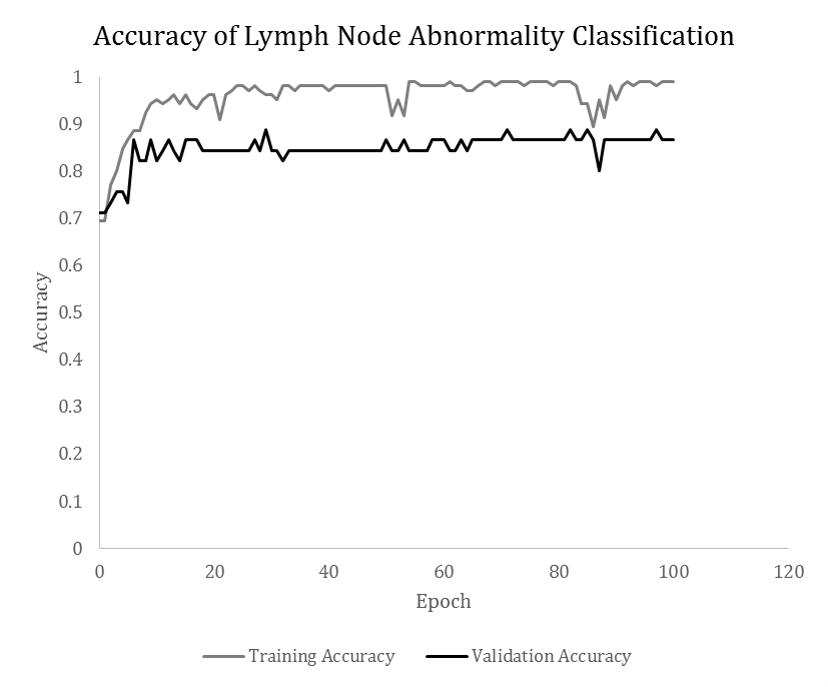
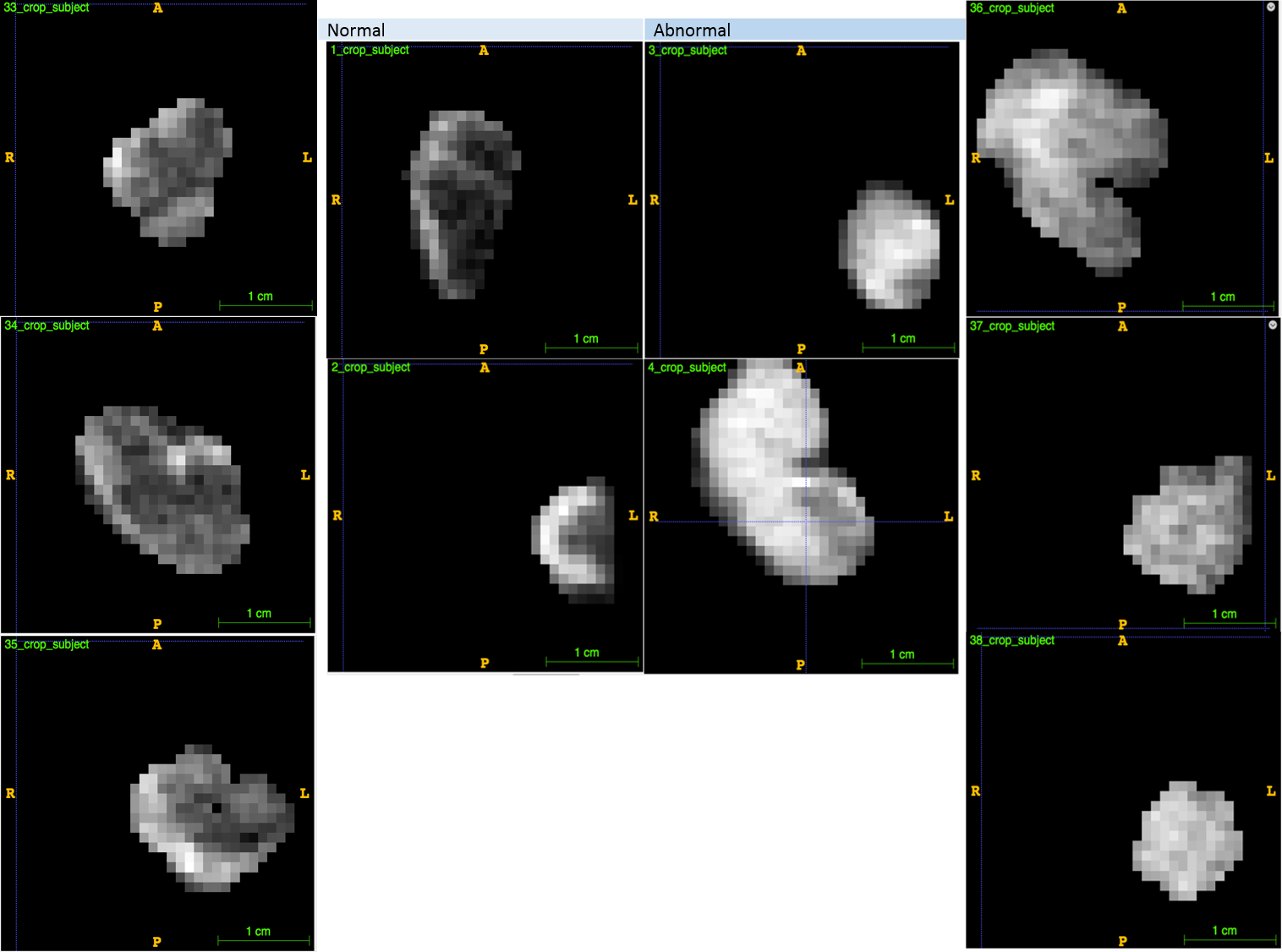
Figure 1 shows a typical run of 100 epochs for the training and validation dataset, showing algorithm convergence. Classification model improves consistently and then plateaus around the 25th epoch. Examples of some of the classification of normal and abnormal nodes are shown in Figure 2. When applied to the validation data, the accuracy (AUC) of classification was 86.7%.
Discussion
CNN can be efficiently used for aLN disease classification with a validation accuracy of 86.7%. Our accuracy compared favorably to previous reports using different imaging and analysis methods. With ultrasound, accuracy was 67-77% and sensitivity 43.5-72.3% in detecting node metastasis [3]. With FDG-PET accuracy was 81.1% and sensitivity 56-63% in detecting node metastasis [4]. MRI and ultrasound staging yielded accuracy of 72.6% and 73.3% for MRI and ultrasound respectively [7]. Most direct comparison is a previous CNN study of MRI images of axillary lymph which reported an accuracy of 84% [1].
One limitation of this study is a small sample size. Further validation also needs to be performed on a larger and independent dataset. Another limitation is this algorithm is not fully automated. With image quality and contrast, the results will likely improve. CNN model can also be trained with multiple MRI data (i.e., T2).
Conclusion
It is possible to automatically classify diseased versus non-diseased aLNs using convolutional neural networks in breast cancer. The results showed the remarkable agreement with ground truths. With improvement in automation and accuracy, this approach may prove useful for automatic detecting aLNs metastasis on MRI in clinical settings.Acknowledgements
No acknowledgement found.References
- Ha R. et al. Axillary Lymph Node Evaluation Utilizing Convolutional Neural Networks Using MRI Dataset. J Digit Imaging. 2018 Apr 25. doi: 10.1007/s10278-018-0086-7.
- M. Ahmed & S. I. Usiskin & M. A. Hall-Craggs & Michael Douek. Is imaging the future of axillary staging in breast cancer? Eur Radiol (2014) 24:288–293
- An YS, Lee DH, Yoon JK, Lee SJ, Kim TH, Kang DK, Kim KS, Jung YS, Yim H: Diagnostic performance of 18F-FDG PET/CT, ultrasonography and MRI. Detection of axillary lymph node metastasis in breast cancer patients. Nuklearmedizin 53(3)
- Cooper KL, Meng Y, Harnan S, Ward SE, Fitzgerald P, Papaioannou D, Wyld L, Ingram C, Wilkinson ID, Lorenz E: Positron emission tomography (PET) and magnetic resonance imaging (MRI) for the assessment of axillary lymph node metastases in early breast cancer: systematic review and economic evaluation. Health Technol Assess 15(4):iii–iiv, 1–134, 2011. https://doi.org/ 10.3310/hta15040
- Huang P. et al. Correlation of PET, MRI, and Pathology of Axillary Nodes in Breast Cancer, ISMRM 2019 submitted.
- Finzel, Mitchell "Convolutional Neural Networks in Medical Imaging," Scholarly Horizons: University of Minnesota, Morris Undergraduate Journal. 2017: Vol. 4 : Iss. 2 , Article 3.
- Hiroyuki A. et al. Accuracy of Axillary Lymph Node Staging in Breast Cancer Patients: An Observer-Performance Study Comparison of MRI and Ultrasound. Acad Radiol. 2013 Nov;20(11):1399-404. doi: 10.1016/j.acra.2013.08.003.
Figures