0600
Deep learning-based whole breast segmentation to support automated breast density measurements from fat-water decomposition MRI1Biomedical Engineering, Stony Brook University, Stony Brook, NY, United States, 2Biomedical Engingeering, Stony Brook University, Stony Brook, NY, United States, 3Medical Imaging, University of Arizona College of Medicine, Tucson, AZ, United States, 4Pathology, Stony Brook Medicine, Stony Brook, NY, United States, 5Hematology & Oncology, Stony Brook Medicine, Stony Brook, NY, United States, 6Radiology, Stony Brook Medicine, Stony Brook, NY, United States, 7Psychiatry, Stony Brook Medicine, Stony Brook, NY, United States
Synopsis
Breast density monitoring has become a clinically interesting topic in the past several years. MRI-based methods are attractive because they allow for frequent monitoring without ionizing radiation. Here, we present evidence that a convolutional neural network can replace manual or algorithmic breast segmentation in such pipelines.
Introduction
Breast cancer, the most commonly diagnosed cancer in women in developed countries, is a pressing public health concern. Elevated breast density (BD) is a widely reported risk factor for developing breast cancer. It has been suggested this risk is modifiable and that a sizeable portion of breast cancer diagnoses could be prevented by decreasing BD.
Because of this, accurate and clinically feasible pipelines for determining BD are an important research topic. The current clinical gold standard is mammographic BD (MBD), however this is not optimal as it exposes the subject to ionizing radiation and requires compression of the breast. Recent publications have demonstrated the suitability of MRI for determining BD (MR-derived breast density; MRD)(1,2). Whole breast segmentation is a requirement for such pipelines, and there is a need to improve upon traditional cumbersome segmentation methods with quicker and more accurate techniques than manual or semi-automated segmentations. In order to promote the clinical viability of MRD analysis, we sought to determine whether a deep learning (DL)-based segmentation method could achieve similar results to a previous automatic segmentation method developed by our group. Whereas the previous segmentation algorithm performed well, it required parameter tuning in order to be used between different scanners and sequences. Demonstrating equivalent or superior performance will allow for more rapid segmentations which are independent of user parameter selection, allowing for the advancement of such techniques toward clinical adoption.
Methods
A total of 234 breast MRI datasets were available. Manual breast segmentations were drawn according to an established protocol(3) prior to our previous study. MRI acquisition consisted of either radial IDEAL-GRASE (n=203) on a 1.5T GE Signa scanner or a 6-echo GRE acquisition on a 3T Siemens Skyra (n=31). Fat-water separation was performed as previously described(1). These datasets were partitioned into two subsets in the former study: 182 scans were used to test accuracy in relation to MBD while 52 paired studies were used to assess test-retest reliability.
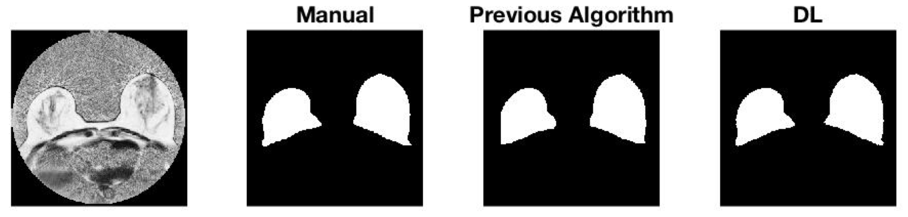
In the previous study, a multi-step segmentation algorithm was employed. It consisted of determining upper and lower boundaries for the breast using the fat and water images respectively, and then creating the breast segmentation using a 3D region growing algorithm followed by automated removal of the nipple. Figure 1 in Results shows a side-by-side comparison of manual and algorithmic segmentations, as well as the DL result, for a randomly selected subject.
In this work, we segment the breast using a u-Net(4). The former data partitioning was employed, with the network trained on the 182 scan dataset and evaluated in the 52 scan test-retest dataset. The network was provided a fat-water ratio image for each scan and trained to maximize the Dice coefficient between the network output and the manual segmentation.
Following network optimization, MRD for each scan in the test-retest dataset was determined using the previous automatic segmentation as well as the DL-based segmentations. Reliability was determined by the mean difference between MRD for paired scans as well as the intraclass correlation coefficient.
Result
The DL method achieved comparable segmentation accuracy to the previous algorithmic method in the testing set (DiceDL: 0.914± 0.03 ; DiceAlgorithm: 0.911±0.03). Figure 1 shows a side-by-side comparison of manual, algorithmic and CNN segmentations.
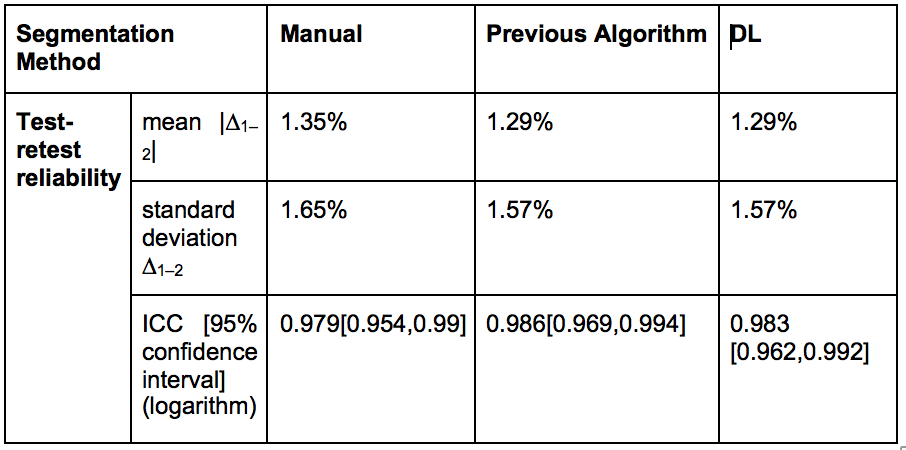
In terms of task-based comparison, the DL-based method exhibited nearly identical performance to the previous algorithmic method; both methods improve upon manual segmentation slightly in terms of reliability. Table 1 shows the precision measures for all three segmentation methods.
Discussion
Whereas our previously published technique(1) was validated for both manual and automated segmentations, the manual segmentation algorithm was cumbersome, requiring multiple processing steps and user supervision. Whereas breast segmentation was fully automated, the algorithm required parameter tuning for the different scan sites and sequences utilized, and relied on assumption of FOV placement. Parameter tuning was seen to control a bias for over or under estimation of breast volume, particularly in the areas close to the medial in deep areas of the breast. In contrast, u-Net performed well for both scanners, independent of user-specified parameters, and spatially invariant. Moreover, the u-Net approach reduced processing time from several minutes with the previous automated technique to less than 10 seconds per subject once the network was trained.
In totality, we observe that DL provides sufficiently accurate and precise segmentations to replace an automated pipeline previously used. It is not only entirely hands off and independent of parameters the user must provide, but it also provides segmentations for a whole breast in several seconds, even without GPU acceleration, as opposed to several minutes for the previous pipeline. These aspects make it more suitable for clinical adoption.
Conclusion
Deep learning-based segmentations are sufficient for use in our automated MR-based breast density pipeline.Acknowledgements
This work was supported by National Institutes of Health (R03CA223052), Carol M. Baldwin Foundation for Breast Cancer Research (2017-Huang), Walk-for-Beauty FoundationReferences
1. Ding J, Stopeck AT, Gao Y, Marron MT, Wertheim BC, Altbach MI, Galons JP, Roe DJ, Wang F, Maskarinec G. Reproducible automated breast density measure with no ionizing radiation using fat‐water decomposition MRI. Journal of Magnetic Resonance Imaging 2018.
2. Wengert GJ, Pinker K, Helbich TH, Vogl WD, Spijker SM, Bickel H, Polanec SH, Baltzer PA. Accuracy of fully automated, quantitative, volumetric measurement of the amount of fibroglandular breast tissue using MRI: correlation with anthropomorphic breast phantoms. NMR in Biomedicine 2017;30(6):e3705.
3. Rosado-Toro JA, Barr T, Galons J-P, Marron MT, Stopeck A, Thomson C, Thompson P, Carroll D, Wolf E, Altbach MI. Automated breast segmentation of fat and water MR images using dynamic programming. Academic radiology 2015;22(2):139-148.
4. Ronneberger O, Fischer P, Brox T. U-net: Convolutional networks for biomedical image segmentation. 2015. Springer. p 234-241.
Figures