0580
Prediction of breast lesion malignancy in high-risk oncogenetic patients with MRI BI-RADS 4 lesion using multiparametric MRI-based radiomicBenjamin Leporq1, Camille Schreiner2, Agnes Coulon2, Olivier Beuf1, and Frank Pilleul2
1CREATIS CNRS UMR 5220; Inserm U1206; INSA-Lyon; UCBL Lyon 1, Université de Lyon, Villeurbanne, France, 2Department of Radiology, Centre de lutte contre le cancer Léon Berard, Lyon, France
Synopsis
In this study a multiparametric MRI-based radiomic method to predict cancer in MRI BI-RADS 4 breast lesions, in high-risk oncogenetic patients is proposed. The results demonstrated that mpMRI-based radiomic can predict all malignant lesions among MRI BI-RADS 4 lesion and reduced the number of unnecessary biopsy by 86% in our population.
Introduction
Breast cancer is one of the major health concerns, and the most common malignancy worldwide for women with an incidence estimated around 2.1 million in 2018(1) and the second leading cause of cancer death, for women (2). Up to 20% of breast cancer occurs in women with a genetic predisposition linked to BRCA1-2 gene mutations (3,4). In this high-risk oncogenetic population, a screening program has been developed, recommending MRI as a supplemental diagnostic tool in many countries (5-7). While MRI have a good sensitivity for breast cancer detection in screening context (estimated at 90%) (4,8-11) it suffer from a lack of specificity with a positive predictive values for MRI BI-RADS 4 lesions reported around 20% (12), many biopsies done for benign lesions could be avoided. Therefore, more specific and objective methods to guide the decision for biopsy in this population are needed. The purpose of this study is to develop and assess a multiparametric MRI (mpMRI)-based radiomic method to predict cancer in MRI BI-RADS 4 breast lesions, in high-risk oncogenetic patients.Methods
49 MRI BI-RADS 4 lesions from 44 high-risk oncogenetic patients with histology and 1.5T multiparametric MRI data available were retrospectively enrolled. Fat-suppressed perfusion-weighted images at 3 min and subtraction; diffusion-weighted images (b = 0 and b = 700 s.mm-2) and ADC maps were used as radiomic fingerprints. The lesions were manually segmented by two independent radiologists to extract the radiome and to study the inter-observer reproducibility. The radiome included 87 features describing shape, size, distribution and texture in for each radiomic fingerprint in images and frequency domain (Fig.1). Overall, 435 features were integrated. The learning base dimension was reduced to decrease the risk of overfitting and create another set of relevant features in term of relevancy and inter-observer reproducibility criterion. This procedure was achieved using a backward selection by a double thresholding on t-test p-value (t < 0.2) and Pearson’s correlation coefficient (t > 0.8), computed from the reproducibility study. The implementation of classification model was performed with a support vector machine as a classifier with a linear kernel. Before training, data were centered at their mean and scales to have unit standard deviation. Support vector computation and hyperplane separation was done using a sequential minimal optimization. Internal validation was performed with a holdout cross-validation method (75 % of data were used for training and 25 % for test).Results
Among the 435 radiomic features, Pearson’s correlation coefficient ranged between 0.18 and 0.99; mean: 0.80 ± 0.14. Determination and Spearman rho coefficients ranged between 0.03 and 0.99; mean: 0.66 ± 0.21 and between 0.39 and 0.99; mean: 0.22 ± 0.12 respectively. The parts of reproducible features stratified by feature family and radiomic fingerprint were summarized in Fig.2 and Fig.3. Based on t-test p-value, the radiome extracted from the DWI images at b = 700 s.mm-2 was the most relevant with 36.8% (32/87) of features considered relevant. The radiome extracted from the subtracted dynamic images was the less relevant with only 5.8% (5/87) features considered relevant. The parts of relevant features stratified by feature family and radiomic fingerprint were summarized in Fig.2 and Fig.3. After combination with reproducibility criterion, 8.3% of features (36/435) were integrated in the learning step. The diagnosis performances to predict malignant lesions were: AUROC 0.94; sensitivity, 100% (95% CI: 100 – 100%); specificity, 85.6% (95% CI: 59.8 – 111%); PPV, 87.5% (95% CI: 64.6 – 110%); NPV, 100% (95% CI: 100 – 100%) and accuracy 92.9% (95% CI: 79.4 – 106%).Discussion
In this study, all cancers have been detected and 18 (85.6%) biopsies could be avoided. This is a central issue in these young, anxious and asymptomatic women to improve adhesion to the screening program reduce morbidity, psychologic impact and healthcare cost. To conclude, mpMRI-based radiomic could be helpful to non-invasively predict cancer among MRI BI-RADS 4 lesion in high-risk patients. These results need to be confirmed in a validation cohort from multicentric data.Acknowledgements
This work was performed within the framework of the SIRIC LyriCAN grant INCa_INSERM_DGOS_12563 and LABEX PRIMES (ANR-11-LABX-0063), program "Investissements d'Avenir" (ANR-11-IDEX-0007).References
(1) Ferlay J et al. Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.fr/today, accessed [20 Sept 2018] (2) Siegel RL et al. CA Cancer J Clin 2017; 67(1):7-30. (3) Collaborative Group on Hormonal Factors in Breast Cancer. The Lancet 2001; 358(9291):1389-1399. (4) Riedl CC et al. J Clin Oncol 2015; 33(10):1128-1135. (5) Mann RM et al. Eur Radiol 2015; 25(12):3669-3678. (6) Sardanelli et al. Eur J Cancer 2010; 46(8):1296-1316. (7) Kuhl et al. Radiology 2017; 283(2):361-370. (8) Warner E et al, JAMA 2004; 292(11):1317-1325. (9) Sardanelli et al. Invest Radiol 2011; 46(2):94-05. (10) Kuhl et al. J Clin Oncol 2010; 28(9):1450-1457. (11) Bluemke DA et al. JAMA 2004; 292(22):2735-2742 (12) Mahoney MC et al. Radiology 2012; 264(1):51-58.Figures
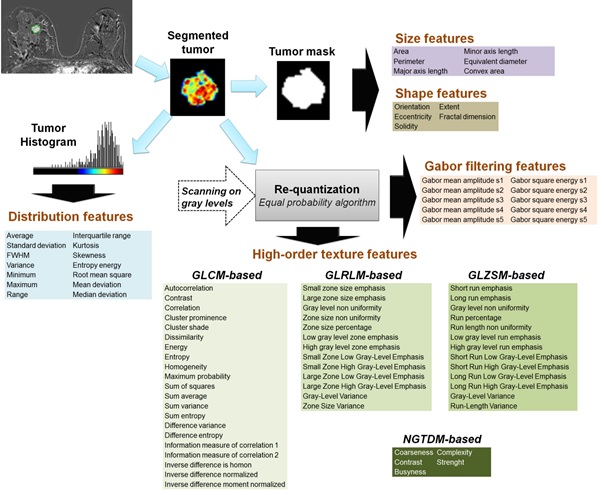
Fig.1: Radiome extraction pipeline. Size and shape features were extracted from the binary
mask. Intensity distribution features were extracted from the histogram built
with 256 bins. Images gray levels were discretized in a smaller number of gray
levels with an equal probability algorithm. Images were discretized in 8, 16,
24, 32, 40, 48 and 64 grey levels. For each discretization level, four matrixes
were built: GLCM (Gray-level co-occurrence), GLRLM (Gray-level run length),
GLSZM (Gray-level size zone) and NGTDM (Neighborhood gray tone difference) from
which characteristics were extracted, then averaged. Frequency domain-based
texture features were extracted using a Gabor filtering.
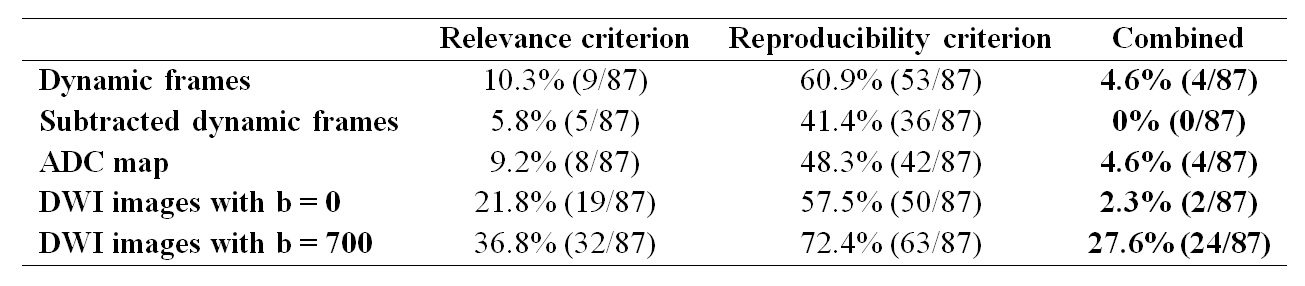
Fig.2: Part of features integrated in the learning step for the prediction of
malignant lesion for each radiomic fingerprint stratified by filter criterion.
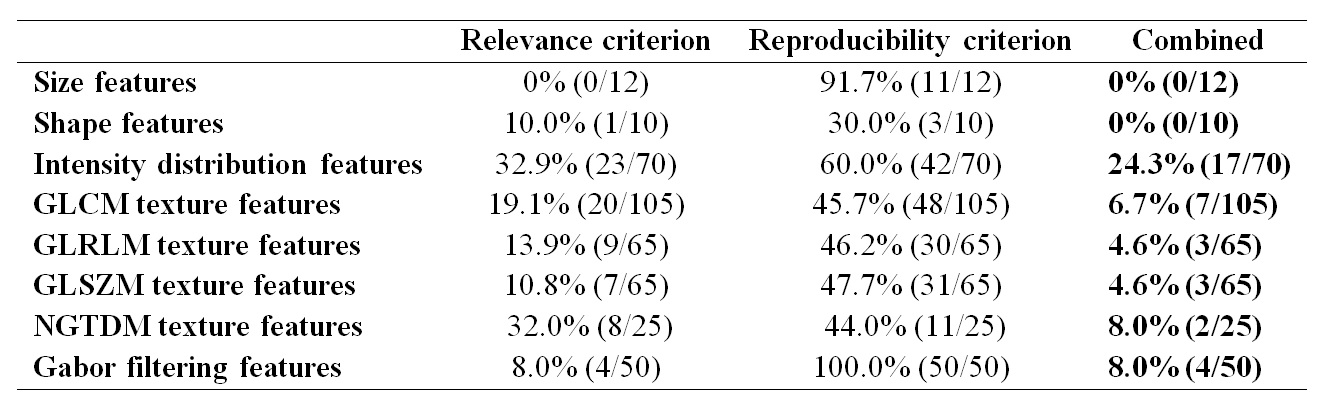
Fig.3: Part of features integrated in the learning step for the prediction of
malignant lesion for each feature family stratified by filter criterion.