0575
Respiratory Motion Management in MR-guided Radiotherapy treatment and assessment with IVIM.1Radiation Oncology, Virginia Commonwealth University, Richmond, VA, United States, 2C. Kenneth and Dianne Wright Center for Clinical and Translational Research, Virginia Commonwealth University, Richmond, VA, United States, 3Radiation Oncology, Washington University in St. Louis, St. Louis, MO, United States
Synopsis
In
radiotherapy (RT), respiratory motion induced target displacement can cause the
treatment beam to miss the target, irradiating normal tissue instead. This
study introduces a novel pressure based motion management system with
biofeedback, compatible with MRI, CT, and megavoltage RT. A belt, wrapped around
the abdomen, with a pressure sensor provided respiratory traces and guidance to
subjects during MR acquisition. Superior-inferior liver dome motion could be
reduced from 30.6mm under free breathing to 5.6mm with a small guiding window. This
device provides significant motion reduction and a surrogate to internal organ
motion for use across the RT treatment process.
Introduction
This pilot study introduces a pressure belt design for respiratory motion management (RMM) and biofeedback. Respiratory motion in the thoracoabdominal cavity is a major cause of positional uncertainty in radiotherapy (RT), increasing the probability of increased dose to normal tissue, and geometric miss of target volumes.1,2 Currently, compression and motion monitoring belt systems in RT do not provide biofeedback to the patients and contain metal, further, compression plate systems cannot be placed in MR bores due to size restrictions, and the plate prevents RF coil placement. Various other motion management methods have been introduced in RT, including breath-hold techniques, respiratory gating, target tracking, surface monitoring, and image reconstruction methods.3-6 These methods reduce target motion or positional uncertainty, but are not useable in all stages of RT treatment, or do not provide real-time feedback to the patient. To the authors’ knowledge this is the first pressure based RMM system which can be used throughout the radiotherapy treatment process, including MR and CT acquisition, and treatment delivery, while also providing quantitative biofeedback to the patient. The device can be used for breath hold monitoring as well, displaying the breath hold window and trace.Methods
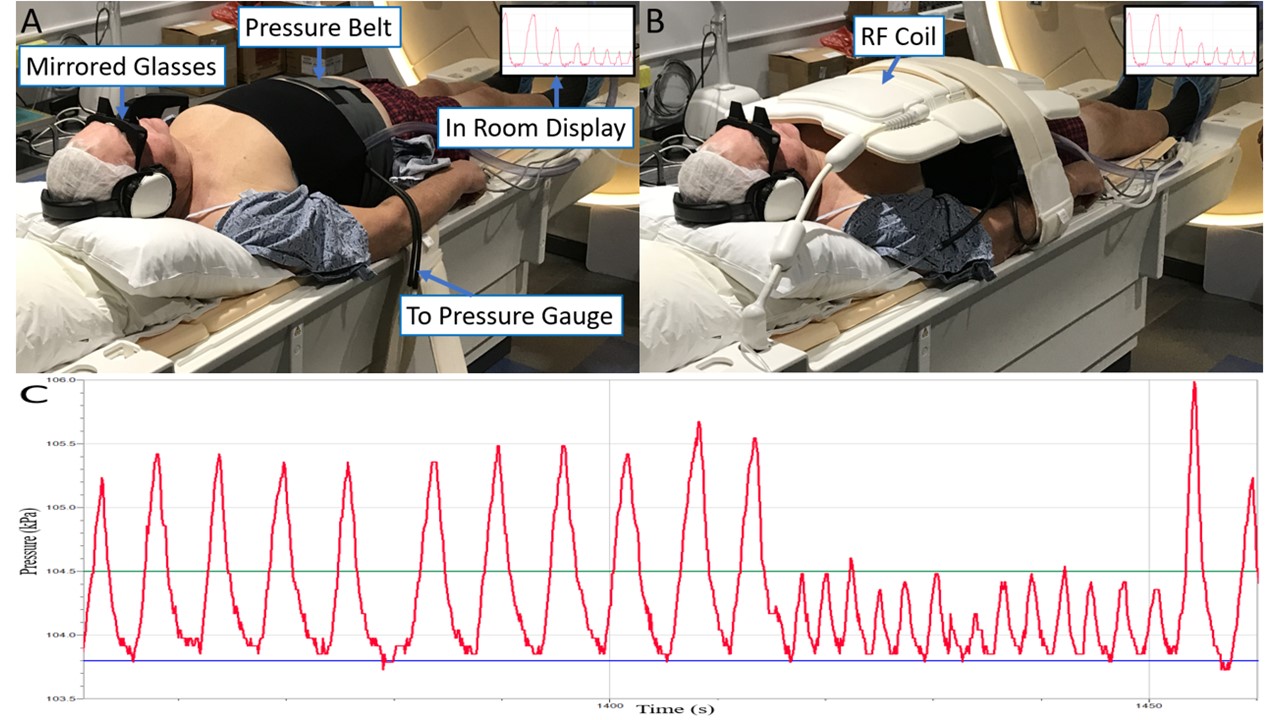
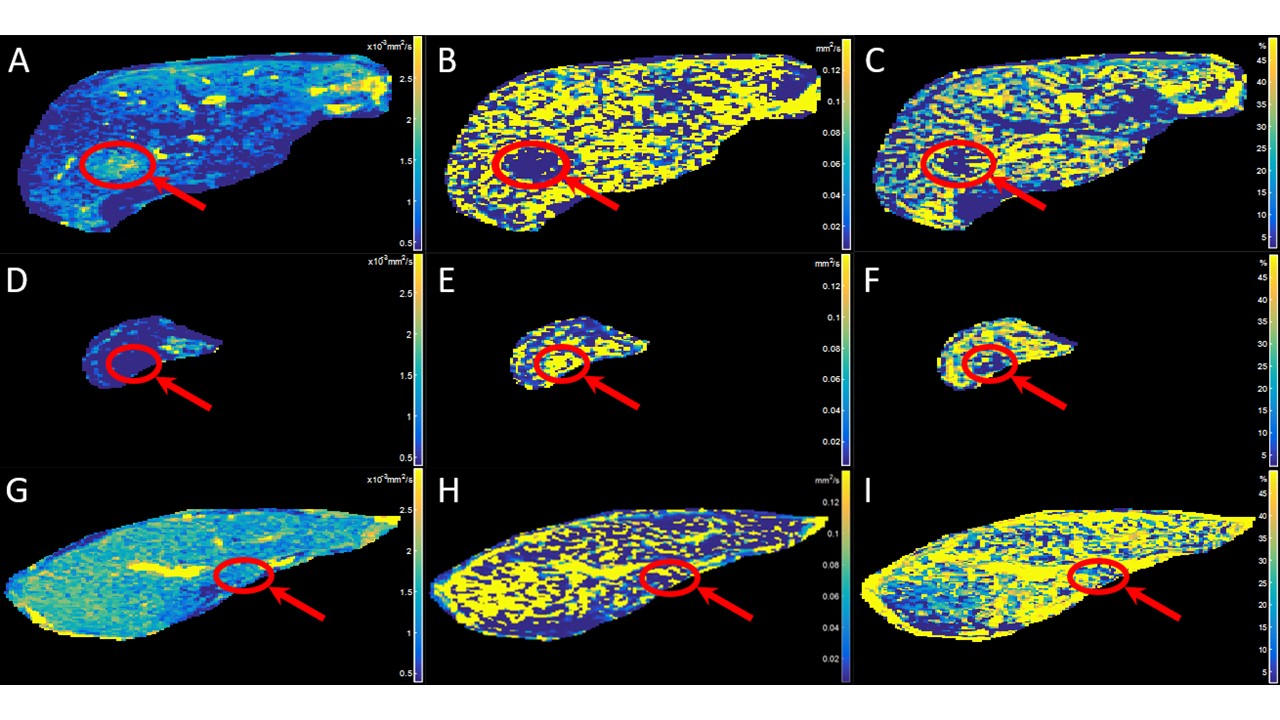
The real-time RMM with biofeedback system was implemented by modifying a commercially available pressure sensor belt system. The belt system was modified by removal of the metal-rubber air pump, metallic pressure gauge, and metal facets, creating a sealed system with minimal air loss. The belt was connected to an electronic pressure sensor which sent real-time pressure signals to the subject using an in-room screen, and mirrored glasses, through a commercial software (LoggerPro). Figure 1A-C show an example setup using the pressure belt system, as well as a respiratory trace under normal breathing and guided shallow breathing. Three separate imaging groups participated to test this system, including two healthy investigators (group 1), five healthy volunteers (group 2), and three liver cancer patients prior to treatment (group 3). Investigators underwent two MR imaging sessions separated by one week. Investigators were imaged under three scenarios: free breathing (FB), maintaining their respiratory signal within a large guiding window (GW), and within a small GW on the visual guidance screen. A CINE MR acquisition over 30s and a diffusion weighted imaging (DWI) volume with two b-values were acquired for each scenario. Group 2 and 3 were imaged with the proposed monitoring system undergoing CINE and DWI acquisitions with eight b-values of 0, 20, 40, 80, 100, 300, 600, and 1000s/mm2 (IVIM). Intra-voxel incoherent motion (IVIM) values, including Dslow, Dfast, and perfusion fraction (PF) were calculated using a biexponential fit of equation 1 to all b-values, using the Levenberg-Marquardt fitting algorithm.7
$$ Sb/S0 = (1-PF)*exp(-b*Dslow)+PF*exp[-b*(Dslow+Dfast)] (1)
Results
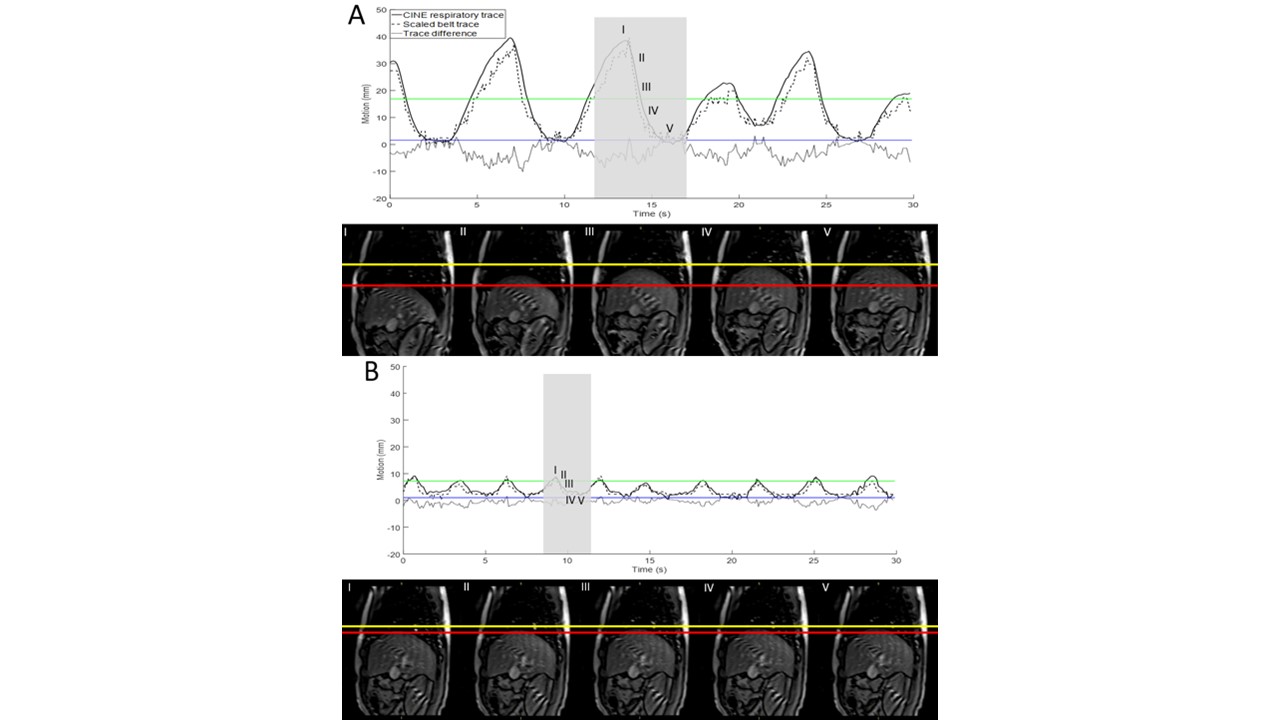
In the investigator study, peak-to-peak motion of the liver dome was reduced from a mean of 30.55±7.83mm for FB to 11.5±3.67mm and 5.58±0.85mm for large and small GW respectively. Figure 2A-B show the respiratory traces for one investigator under FB, and small GW. During the volunteer study, the MR technologist’s instructions for BH and guided breathing were understood and achieved by the volunteers. The difference between CINE motion amplitude and belt amplitude was less than 3.5mm for all volunteer CINE acquisitions. Healthy volunteers and patients were able to comply with instructions. Figure 3 displays the Dslow, Dfast, and PF value maps of IVIM calculated for group 3, using the motion management system. Patients 1 and 3 had masses near the liver center of mass, while patient 2 had a mass near the inferior tail.Discussion
This study found that this device could significantly reduce the SI respiratory motion from FB, provide biofeedback to the subject, and be used in the MR, CT, optical surface tracking, and RT treatment environments. The study subjects were able to successfully maintain their respiratory traces within the GW, with simple instructions from the operator for MR acquisitions. The belt was also able to track liver dome position with an average error of 2.3mm when compared to CINE images.Conclusion
The RMM and biofeedback system can greatly reduce peak-to-peak motion of the liver and reduce motion error during MR acquisition including CINE and IVIM. The system can be utilized in the entire radiotherapy procedure for image-guided RT and assessment.Acknowledgements
This research has been supported by Institutional Research Grant IRG-14-192-40 from the American Cancer Society.References
- Keall, P, Magera, G, Balter, J, et al. The management of respiratory motion in radiation oncology report of AAPM Task Group 76. Medical Physics. 2006;33(10):3874-3900.
- Pollock S, Keall, R, Keall, P. Breathing guidance in radiation oncology and radiology: A systematic review of patient and healthy volunteer studies. Medical Physics. 2015;42(9):5490-5509.
- Kim, S, Pollock, S, Lee, D, O’Brian, R, and Keall, P. Audiovisual biofeedback improves diaphragm motion reproducibility in MRI. Medical Physics. 2012;39(11):6921-6928.
- Park, Y., Kim, S, Kim, H, et al. Quasi-breath-hold technique using personalized audio-visual feedback for respiratory motion management in radiotherapy. Medical Physics. 2011;38(6.1):3114-3124.
- Kim, T, Kim, S, Park, Y, et al. Motion management within two respiratory-gating windows: feasibility study of dual quasi-breath-hold technique in gated medical procedures. Physics in Medicine and Biology. 2014;59:6583-6594.
- Kim, T, Kim, S, Kim, D, et al. Development of real time abdominal compression force monitoring and visual biofeedback system. Physics in Medicine and Biology. 2018; 63(5).
- Li, Y, Cercueil, JP, Yuan, J, et al. Liver intravoxel incoherent motion (IVIM) magnetic resonance imaging: a comprehensive review of published data on normal values and applications for fibrosis and tumor evaluation. Quantitative Imaging in Medicine and Surgery. 2017;7(1):59-78.
Figures