0547
Detection of abnormal glucose uptake and metabolism in perinatal hypoxia using glucoCEST MRI1Howard University, Washington, DC, United States, 2Children's National Medical Center, Washington, DC, United States
Synopsis
Perinatal brain injury, such as perinatal hypoxia from chronic lung disease, results in devastating, neurologic impairment. The immediate and long-term effects on brain energy metabolism of glucose – a major source of energy for the brain - are not known. Previous studies have shown that perinatal brain injury from perinatal hypoxia results in long-term decreases in neuronal oxidative metabolism of glucose and decreased synthesis of N-acetylaspartate. In this study, we utilized dynamic glucoCEST enhancement MRI to investigate the pattern of glucose uptake and metabolism between the mice of normoxic and hypoxic treatment.
Introduction
Perinatal brain injury, such as perinatal hypoxia from chronic lung disease, results in devastating, neurologic impairment. The immediate and long-term effects on brain energy metabolism of glucose – a major source of energy for the brain - are not known. Using 13C-MRS, previous studies have shown that perinatal brain injury from perinatal hypoxia results in long-term decreases in neuronal oxidative metabolism of glucose and decreased synthesis of N-acetylaspartate [1]. In this study, we utilized dynamic glucoCEST enhancement to investigate the pattern of glucose uptake and metabolism between the mice of normoxic and hypoxic treatment.Materials and Methods
Perinatal mice were undergo hypoxic or normoxic treatment (n=3/group), followed by glucoCEST in young adult stages of life. For the hypoxia treatment, mice were exposed to 11% O2 in a chamber from postnatal day (P) 1 to P11 – a period of time that corresponds in humans to the third trimester, when chronic lung disease is prevalent. The normoxic controls are housed in the same room but not exposed to hypoxia. At the time (P30) for imaging experiments, a dose of 0.55 mg/g of metabolizable D-glucose was delivered intraperitoneally to the mice. GlucoCEST datasets were acquired in vivo using a Bruker 9.4T scanner by 2D fast spin echo (TR/TE 3.1s/10.4ms; rare factor 4; in plane resolution: 200µm2, thickness: 0.8mm) with (MT) and without (M0) MT saturation pulses (2μT/2s). The MT offset frequences (Δω) were set from -1.6kHz to +1.6kHz with 40Hz stepping to sample 81 points covering the frequency offset range from -4ppm to +4ppm to detect the proton metabolites of glucose. CEST data were calibrated for B0/B1 field inhomogeneity using WASSR [2] technique (0.8µT, 500ms) and spectral interpolation. The glucoCEST contrast were derived by asymmetry of magnetization transfer ratio (MTRasym) calculating the area under the curve at 1.2ppm, 2.1ppm, 2.9ppm for mapping the glucose levels in brain overtime [3]. The glucoCEST data were acquired prior to the glucose delivery, 0.5, 2.0 and 3.5 hr after glucose injection. Data were examined by one-way ANOVA using Prism v6.0 and Matlab scripts.Results
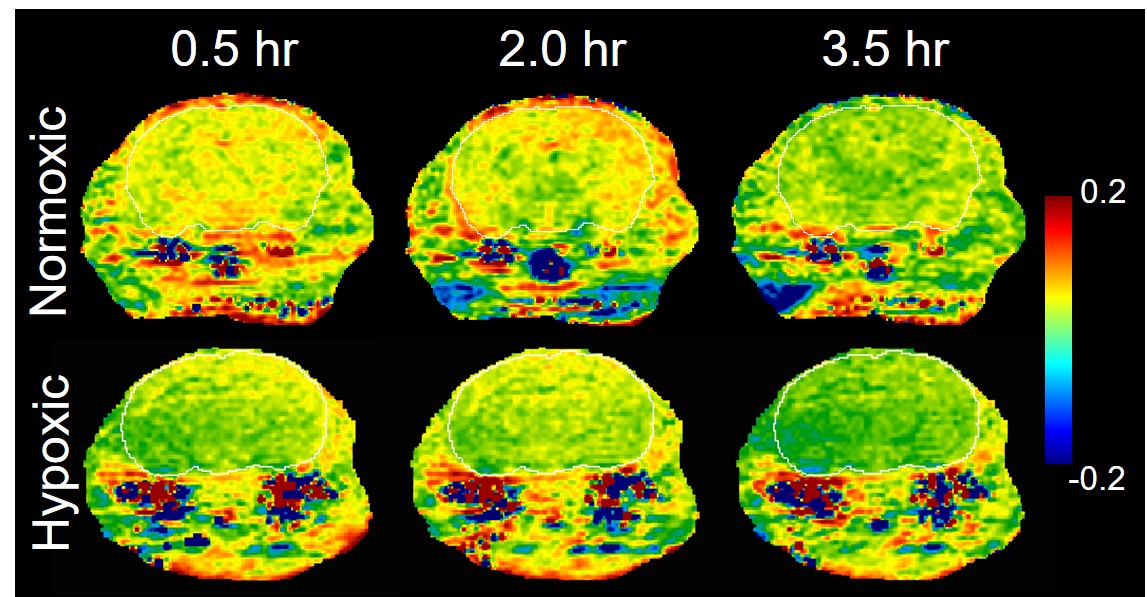
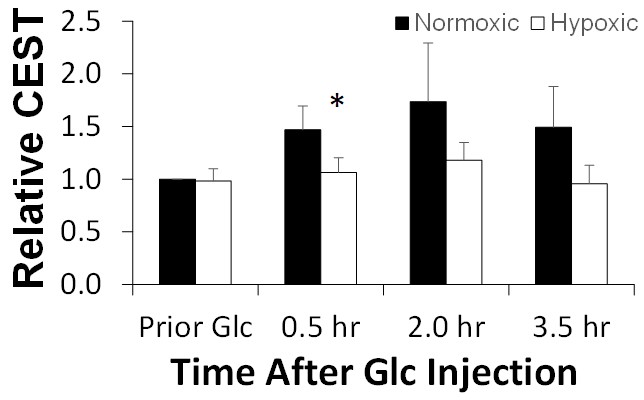
Figure 1 compared the in vivo glucoCEST map in various time points after glucose injection. The normoxic brain showed clear contrast enhancement starting from 0.5 hr after glucose injection, and reached the highest contrast in 2.0 hr. The glucoCEST contrast disappeared after 3.5 hr post injection. The hypoxic brain endured fewer contrast enhancements after the glucose injection. The group averaged data indicated a ~30%reduction of the glucoCEST contrast in the normoxic brain (Fig. 2).Discussion and Conclusion
The common underlying pathogenesis in perinatal hypoxia causes injury to vulnerable neurons and glia affecting approximately 40% of children born premature with significant, permanent neurologic deficits. The perinatal injury due to hypoxia causes perturbation to cerebral glucose metabolism impaired the balance of brain energy supply and consumption, increased apoptosis and arrested development of cerebral progenitor cells. This study demonstrated that the glucoCEST imaging is capable of detecting the glucose uptake deficit and abnormal metabolism in the hypoxic brain. The future work will utilize current glucoCEST imaging technique and compare with 13C-NMR acquisition in various brain structures to examine the regional metabolic changes in the normal developing brain and after perinatal hypoxia.Acknowledgements
No acknowledgement found.References
1. Brooks et al., the Journal of head trauma rehabilitation. 2001;16(2):149-164.2.
2. Kim et al., MRM 2009 61:1441-1450.
3. Tu et al., Scientific Report 12 2018;8(1):669.
Figures