0498
Effects of Tetrahydrobiopterin on Limb Blood Flow and Muscle Metabolism in Patients with COPDStephen Decker1, Oh-Sung Kwon2, Taylor S Thurston3, Yann Le Fur4, Eun-Kee Jeong5, and Gwenael Layec1
1Kinesiology, University of Massachusetts Amherst, Amherst, MA, United States, 2Internal Medicine, University of Utah, Salt Lake City, UT, United States, 3Nutrition and Integrative Physiology, University of Utah, Salt Lake City, UT, United States, 4Centre de Resonance Magnetique Biologique et Medicale, Marseille, France, 5Radiology and Imaging Services, University of Utah, Salt Lake City, UT, United States
Synopsis
Exercise intolerance is an important predictor of mortality in patients with COPD, and evidence shows reduced nitric oxide (NO) bioavailability is a contributing factor. Thus, restoration of NO using BH4, a cofactor involved in NO production, is a novel therapy for improving oxygenation and metabolism in these patients. Patients with COPD performed dynamic plantar flexion exercise with 31P-MRS and vascular Doppler ultrasound assessments following supplementation of BH4. Limb blood flow during exercise was unchanged, however, exercise-induced changes in metabolic measurements were improved with BH4 supplementation. Therefore, BH4 supplementation in patients with COPD appears a promising therapy to improve muscle metabolism.
Introduction
Exercise intolerance is a frequent complaint and an important predictor of mortality in patients with Chronic Obstructive Pulmonary Disease (COPD). Though several factors have been implicated in the development of muscle dysfunction with COPD, chronic oxidative stress and reduced nitric oxide (NO) bioavailability have been previously suggested to be key factors involved in impaired muscular function. Thus, restoration of the redox balance and NO bioavailability using tetrahydrobiopterin (BH4), an essential cofactor involved in the production of NO and free-radicals, appears to represent a novel therapeutic target for improving muscle oxygenation and metabolism in patients with COPD.Methods
We determined the effects of an acute BH4 supplementation (10 mg.kg-1) on peripheral O2 delivery and muscle metabolism in the plantar flexor muscles of patients with COPD. In a single-blinded, placebo-controlled crossover trial, 7 patients with clinically diagnosed COPD performed dynamic plantar flexion exercise at 40% of maximal work rate with phosphorus magnetic resonance spectroscopy (31P-MRS), and vascular Doppler ultrasound assessments following oral supplementation of BH4 or placebo (PL). Experimental procedures consisted of 1 minute of resting baseline, followed by 4 minutes of dynamic plantar flexion exercise at 40% peak work rate and 5 minutes of recovery. 31P-MRS was performed using a clinical 2.9T MRI system (Tim-Trio; Siemens Medical Solutions) operating at 49.9 MHz with a dual-tuned 31P-proton surface coil placed under the calf at its maximum diameter. The experimental setup is shown in Figure 1. Measurements of popliteal artery blood velocity and vessel diameter were performed in the exercising leg with Doppler ultrasound (Logiq e7, GE Healthcare).Results
Limb blood flow during exercise was not significantly different between BH4 and PL. In contrast, exercise-induced changes in pH (PL: 6.86 ± 0.05; BH4: 6.92 ± 0.03, P=0.08), inorganic phosphate (Pi) (PL: 8.9% ± 0.96%; BH4: 5.0% ± 1.2%, P<0.05), and phosphocreatine (PCr) recovery τ (PL: 57.8s ± 4.9; BH4: 36.4s ± 3.4, P<0.05) showed attenuated responses with BH4 supplementation.Discussion
In individuals diagnosed with COPD, acute oral supplementation with BH4 did not result in significant alterations to the hyperemic response during or following 4 minutes of dynamic PF exercise. However, the metabolic disturbance during exercise appears to be blunted and the reliance on anaerobic metabolism reduced. Additionally, improved PCr recovery kinetics following exercise with BH4 supplementation is indicative of improved mitochondrial function.Conclusion
Acute oral BH4 supplementation in patients with COPD appears a promising therapy to, at least partially, restore skeletal muscle metabolism, thus potentially contributing to improved exercise tolerance and quality of life.Acknowledgements
This work was funded in part by grants from the Flight Attendant Medical Research Institute (FAMRI), NIH National Heart, Lung, and Blood Institute (K99HL125756, HL-103786, HL-116579, HL-091830) and VA Merit Awards E6910-R and E1697-R, and VA SPiRe Award E1433-P.References
No reference found.Figures
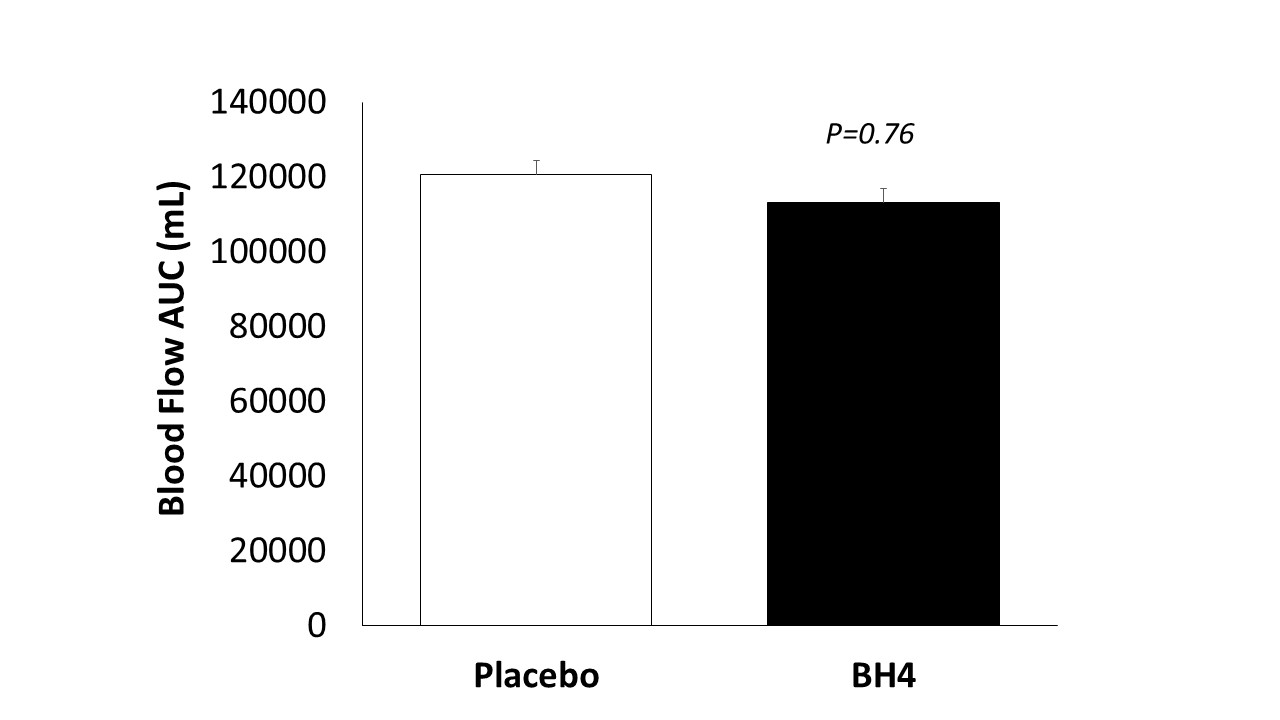
Lower
limb blood flow AUC during plantar flexion exercise. Data are shown as mean ± SEM
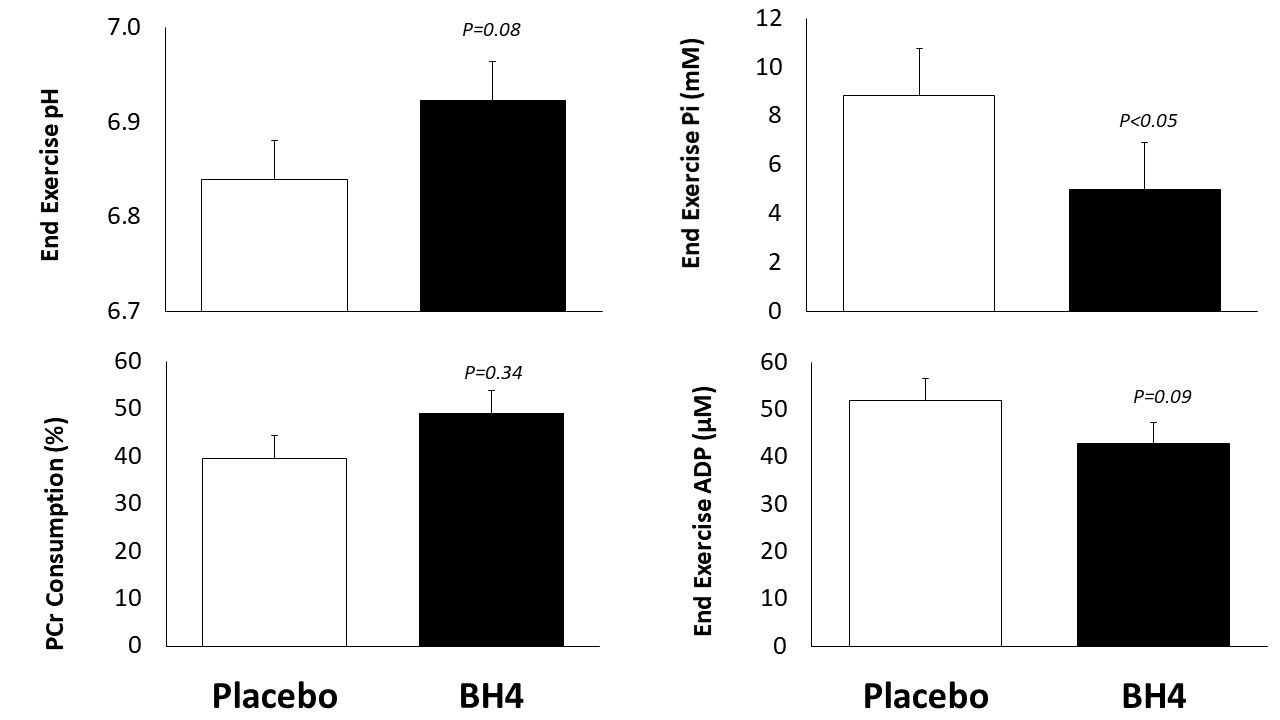
Plantar flexor muscle metabolism assessed by 31P-MRS. Exercise-induced changes in skeletal muscle pH, inorganic phosphate (Pi), phosphocreatine (PCr), and adenosine diphosphate (ADP). Data are shown as mean ± SEM.
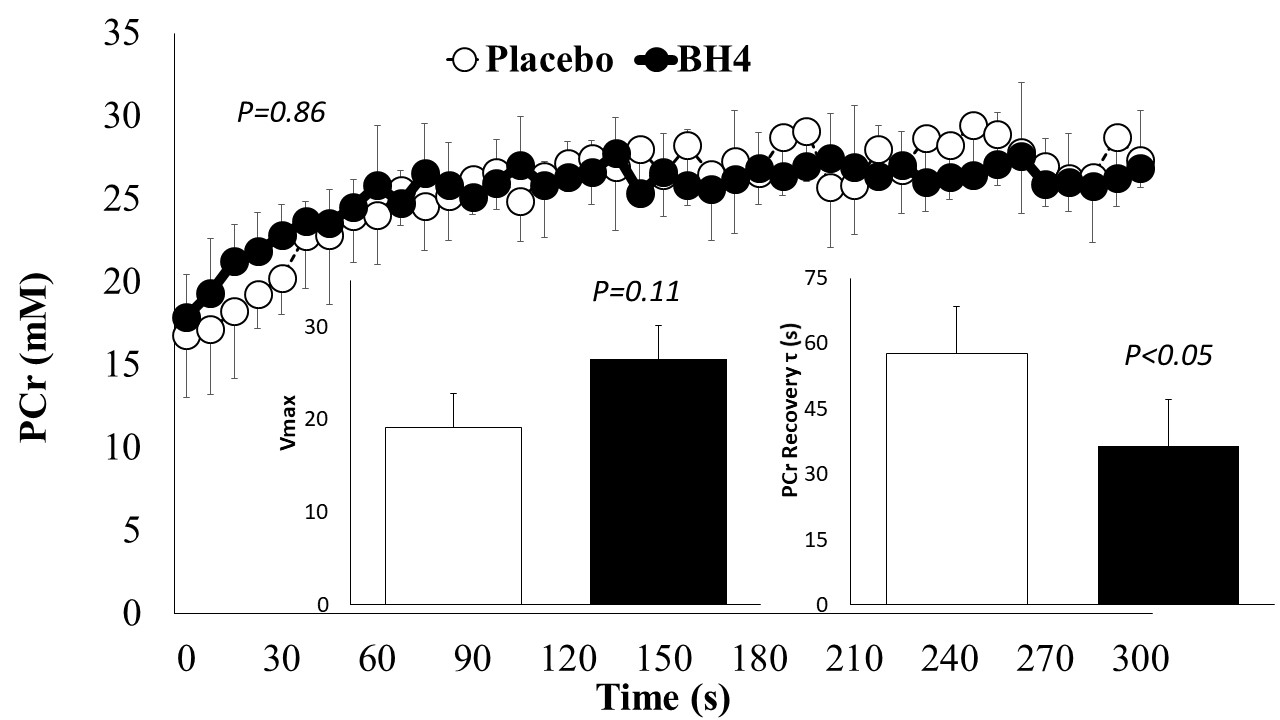
PCr recovery kinetics following dynamic plantar flexion exercise. The figure inserts represent the PCr recovery time constant and peak rate of oxidative ATP synthesis (Vmax). Data are shown as mean ± SEM.