0487
Quantitative 23Na MRI of the human liver at 7 Tesla1Medical Physics in Radiology, German Cancer Research Center (DKFZ), Heidelberg, Germany, 2Faculty of Physics and Astronomy, University of Heidelberg, Heidelberg, Germany, 3Institute of Radiology, University Hospital Erlangen, Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU), Erlangen, Germany, 4Institute of Medical Physics, Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU), Erlangen, Germany, 5Faculty of Medicine, University of Heidelberg, Heidelberg, Germany
Synopsis
Sodium (23Na) MRI has been proposed as a potential imaging modality for the characterization of hepatic tumors and for monitoring therapy response. Up to now, only one study has been performed on implanted hepatocellular carcinomas in rats. In the present work, in-vivo 23Na MRI of the healthy human liver is performed and to the best of our knowledge, the hepatic tissue sodium concentration is estimated for the first time. For quantitative 23Na MRI correction methods were applied such as self-gating and B1+ correction. The mean sodium concentration for three volunteers was estimated to be (27±5) mM in the liver.
Introduction
The tissue sodium (23Na) concentration is associated with the viability of cells(1). 23Na MRI may provide noninvasive information about tumor characterization and early therapy response(2). Hence, 23Na MRI has been proposed as a potential imaging modality for the investigation of hepatic tumors(3). However, abdominal 23Na MRI is challenging due to low NMR sensitivity, low in-vivo concentrations, short transverse relaxation times and respiratory motion. Up to now, only one study has been performed on implanted hepatocellular carcinomas in rats(3). In the presented work, in-vivo 23Na MRI of the healthy human liver is performed and to the best of our knowledge, the hepatic tissue sodium concentration (TSC) is estimated for the first time.Methods
23Na abdominal images were acquired for three healthy volunteers (2 female, 1 male, mean age: 27.3±1.5 years) on a 7T whole-body system (MAGNETOM 7T, Siemens Healthcare GmbH, Erlangen, Germany) with an oval-shaped birdcage coil tailored for torso examinations(4). Density-adapted 3D radial sampling(5) and a golden angle distribution of projections(6) were applied with the following parameters: pulse duration tp=1.8 ms, TE/TR=1.00 ms/150 ms, nominal spatial resolution (∆x)3=(5 mm)3, flip angle α=61°, readout time tRO=5 ms. For concentration determination, two reference vials with NaCl solutions (20 mM, 50 mM) were used. To generate B1+ maps, the dual-angle method(7) was applied (tp=3 ms, TE/TR=1.55 ms/150 ms, (∆x)3=(10 mm)3, α=45°/90°, tRO=10 ms). The total acquisition time was about 60 min.
Full datasets were reconstructed with a Non-Uniform Fast Fourier Transform (NUFFT)(8) without and with a Hamming filter as well as with a Dictionary-Learning Compressed Sensing reconstruction (DLCS)(9). The influence of respiratory motion blurring was reduced by applying a self-gating method(4,10) together with a separate DLCS reconstruction of the exhaled state. Datasets for B1+ maps were Gauss-filtered (σ=20 mm), interpolated and corrected for T1 relaxation effects in the vials, since 5∙T1NaCl=5∙56 ms > TR=150 ms(11). For liver tissue full relaxation was assumed (TR>>T1liver).
The exhaled sodium DLCS reconstruction was corrected for B1+ effects as well as for T1 relaxation effects in the reference vials. TSC in liver, renal medulla and renal cortex were determined using the known concentrations in the reference vials. Fig.1 displays the workflow from the reconstruction to the final sodium concentration in the liver.
Results
Image noise is reduced in 23Na abdominal images by using a NUFFT reconstruction with a Hamming filter or the DLCS reconstruction (Fig.2). Compared to the NUFFT image with Hamming filter, the DLCS reconstruction shows less blurring. The exhaled DLCS reconstruction shows sharper edges e.g. in the border region between liver and lung (Fig.2, white lines and line plots).
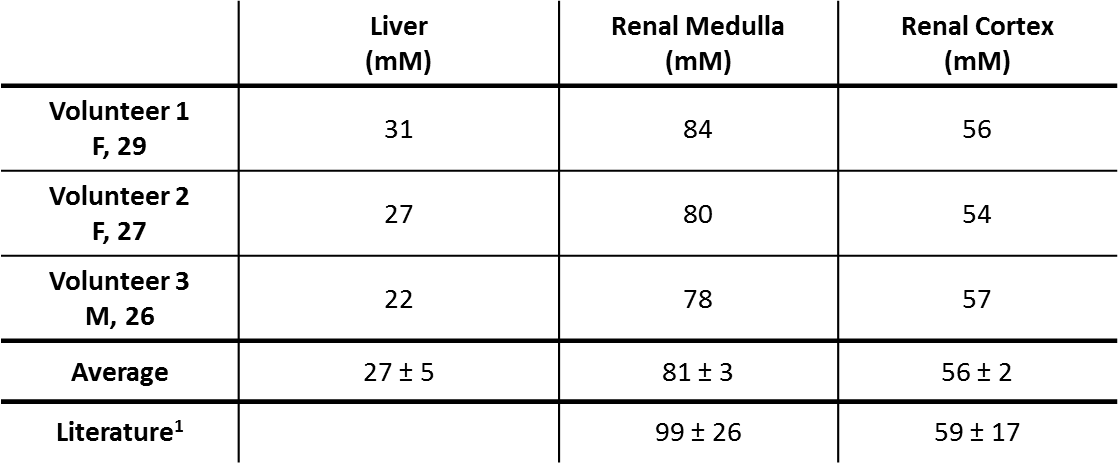
Iterative 23Na reconstructions for the exhaled state are illustrated in Fig.3 for all three volunteers. The mean TSC was estimated to be (27±5) mM in the liver, (81±3) mM in renal medulla and (56±2) mM in renal cortex (Table 1).
Discussion & Conclusion
Sodium abdominal MRI shows the expected signal distribution with high values in renal medulla, moderate values in renal cortex and low values in the liver. Quantitative 23Na MRI of the abdomen benefits from high magnetic fields (B0=7 T), self-gated iterative reconstructions and the applied signal corrections. Haneder et al.(12) reported a TSC of (99±26) mM in renal medulla and (59±17) mM in renal cortex. Hence, the renal concentrations determined here are in good agreement with literature, indicating that the method of quantitation is reasonable. Thus, the obtained values of TSC in the liver can be considered as a first estimate.
However, the limitations of this method are: 1) The B1+ maps determined in-vivo can deviate slightly from real conditions due to motion. 2) The coil has a Tx-only birdcage mode and separate receive hardware(4). Thus, determining B1- is challenging in-vivo, and a correction of B1- effects was not performed. 3) Correction of T1 and T2* relaxation effects in hepatic tissue was not performed because relaxation times at 7 T are thus far not known. However, full relaxation was assumed for liver tissue (TR>>T1liver).
In conclusion, quantitative 23Na MRI of the liver is feasible, and a first estimate of hepatic tissue sodium concentration was achieved. In the future, quantitative hepatic 23Na MRI may contribute to characterizing tumors in the liver and to monitoring therapy response(3).
Acknowledgements
This work was supported by iMed – the Helmholtz Initiative on Personalized Medicine.References
1. Madelin G, Regatte RR. Biomedical applications of sodium MRI in vivo. J Magn Reson Imaging 2013;38(3):511-529.
2. Schepkin VD. Sodium MRI of glioma in animal models at ultrahigh magnetic fields. NMR in Biomedicine 2016;29(2):175-186.
3. Babsky AM, Ju SH, Bennett S, George B, McLennan G, Bansal N. Effect of implantation site and growth of hepatocellular carcinoma on apparent diffusion coefficient of water and sodium MRI. NMR in Biomedicine 2012;25(2):312-321.
4. Platt T, Umathum R, Fiedler TM, Nagel AM, Bitz AK, Maier F, Bachert P, Ladd ME, Wielputz MO, Kauczor HU, Behl NGR. In vivo self-gated (23)Na MRI at 7 T using an oval-shaped body resonator. Magn Reson Med 2018;80(3):1005-1019.
5. Nagel AM, Laun FB, Weber MA, Matthies C, Semmler W, Schad LR. Sodium MRI using a density-adapted 3D radial acquisition technique. Magn Reson Med 2009;62(6):1565-1573.
6. Chan RW, Ramsay EA, Cunningham CH, Plewes DB. Temporal stability of adaptive 3D radial MRI using multidimensional golden means. Magn Reson Med 2009;61(2):354-363.
7. Insko EK, Bolinger L. Mapping of the Radiofrequency Field. J Magn Reson Ser A 1993;103(1):82-85.
8. Fessler JA, Sutton BP. Nonuniform fast Fourier transforms using min-max interpolation. IEEE Trans Signal Process 2003;51(2):560-574.
9. Behl NG, Gnahm C, Bachert P, Ladd ME, Nagel AM. Three-dimensional dictionary-learning reconstruction of (23)Na MRI data. Magn Reson Med 2016;75(4):1605-1616.
10. Behl NG, Nagel AM, Umathum R, Maier F, Ladd ME, Wielputz MO, Kauczor HU, Platt T. Dynamic 23Na-Imaging of the human Lung with Fully Flexible Intrinsic Respiratory Gating. Proc Intl Soc Mag Reson Med 2018;26:0627.
11. Nagel AM, Amarteifio E, Lehmann-Horn F, Jurkat-Rott K, Semmler W, Schad LR, Weber MA. 3 Tesla Sodium Inversion Recovery Magnetic Resonance Imaging Allows for Improved Visualization of Intracellular Sodium Content Changes in Muscular Channelopathies. Investigative Radiology 2011;46(12):759-766.
12. Haneder S, Kettnaker P, Konstandin S, Morelli JN, Schad LR, Schoenberg SO, Michaely HJ. Quantitative in vivo 23Na MR imaging of the healthy human kidney: determination of physiological ranges at 3.0T with comparison to DWI and BOLD. MAGMA 2013;26(6):501-509.
Figures