0464
Dynamic Evaluation of Flow in the Lower Extremity Peripheral Arteries using Cine Fast Interrupted Steady-State in Combination with Arterial Spin Labeling.1Radiology, McGaw Medical Center of Northwestern University, Chicago, IL, United States, 2Radiology, NorthShore University HealthSystem, Evanston, IL, United States, 3Radiology, University of Chicago Pritzker School of Medicine, Chicago, IL, United States, 4Vascular Surgery, NorthShore University HealthSystem, Evanston, IL, United States, 5Feinberg School of Medicine of Northwestern University, Chicago, IL, United States
Synopsis
For non-invasive evaluation of peripheral artery disease in the lower extremities prior to revascularization, physicians rely on contrast-enhanced CT angiography and magnetic resonance angiography which generate static images in the arterial phase and do not reveal blood flow. We adapted a prototype non-contrast MRA technique, cine fast interrupted steady-state in combination with arterial spin labeling (cine FISS ASL), to facilitate dynamic visual and quantitative flow evaluation of the lower extremity peripheral arteries. In-plane flow patterns were well visualized and there was very strong positive correlation between peak flow velocities measured by cine FISS ASL and 2D phase contrast MRA.
Introduction
Peripheral artery disease (PAD) is a huge global health issue, affecting approximately 202 million people globally.1 For non-invasive evaluation of peripheral artery disease in the lower extremities prior to revascularization, physicians rely on contrast enhanced CT angiography (CTA) and magnetic resonance angiography (MRA) which generate static images in the arterial phase which are evaluated for degree of stenosis. We adapted a prototype non-contrast MRA technique, cine fast interrupted steady-state in combination with arterial spin labeling (cine FISS ASL) to display in-plane flow patterns and quantify flow velocities.2, 3 We hypothesized that cine FISS ASL could be used to efficiently evaluate vascular morphology and qualitatively and quantitatively evaluate flow in the lower extremity peripheral arteries without use of radiation or intravenous contrast.Methods
We performed an IRB-approved, prospective study on 6 healthy volunteers after obtaining informed, written consent. Scanning was performed on a 1.5 T MR system (Avanto, Siemens Healthineers). Scout imaging was performed using a quiescent interval single-shot (QISS) non contrast ECG-gated MRA at 9 stations throughout the lower extremities. QISS imaging of the pelvis included a single breath hold. ECG-gated cine FISS ASL imaging was performed with tags placed at 4 stations: in the distal thigh, mid-thigh, thigh-pelvis and pelvis with free breathing. For comparison of flow quantification measurements, through plane phase contrast imaging was performed at the same 4 stations. 4, 5 Peak velocity was compared at each level for cine FISS ASL and 2D cine phase contrast (2DPC).Results
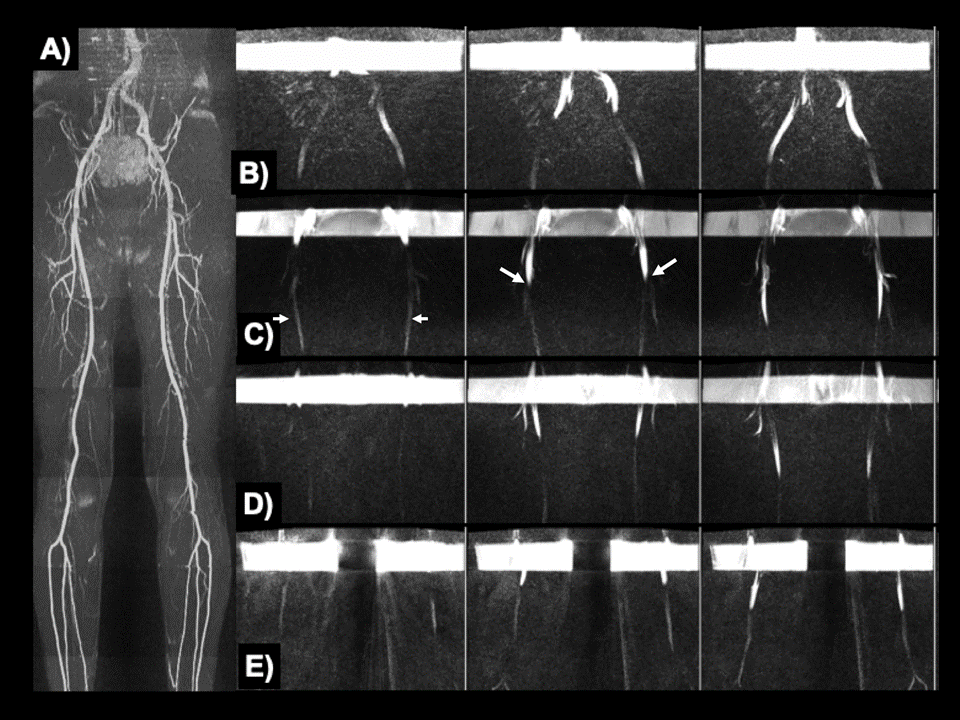
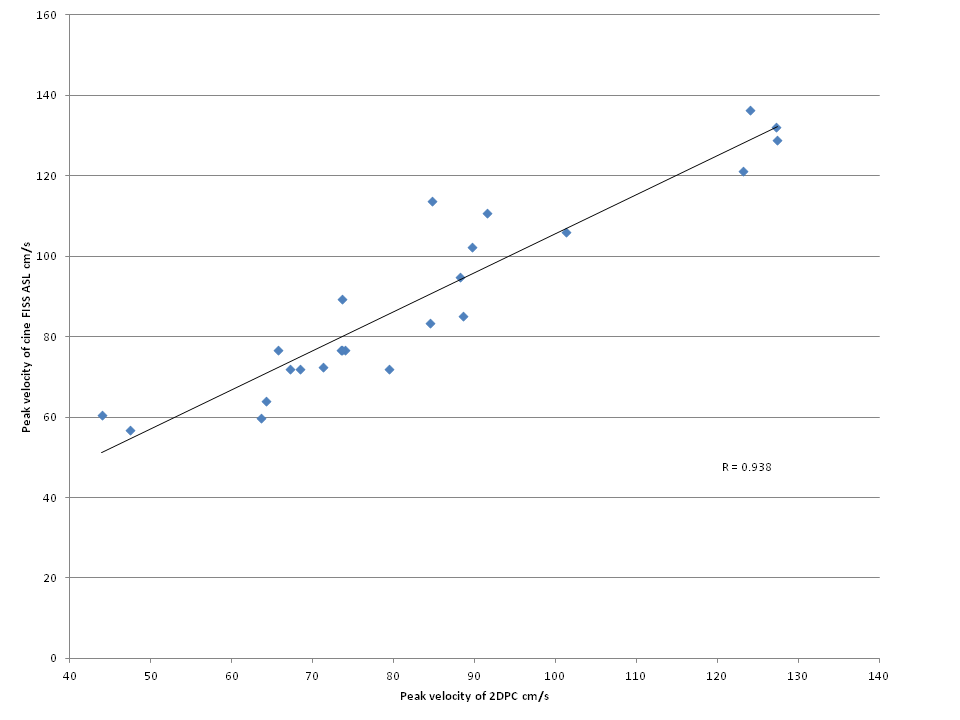
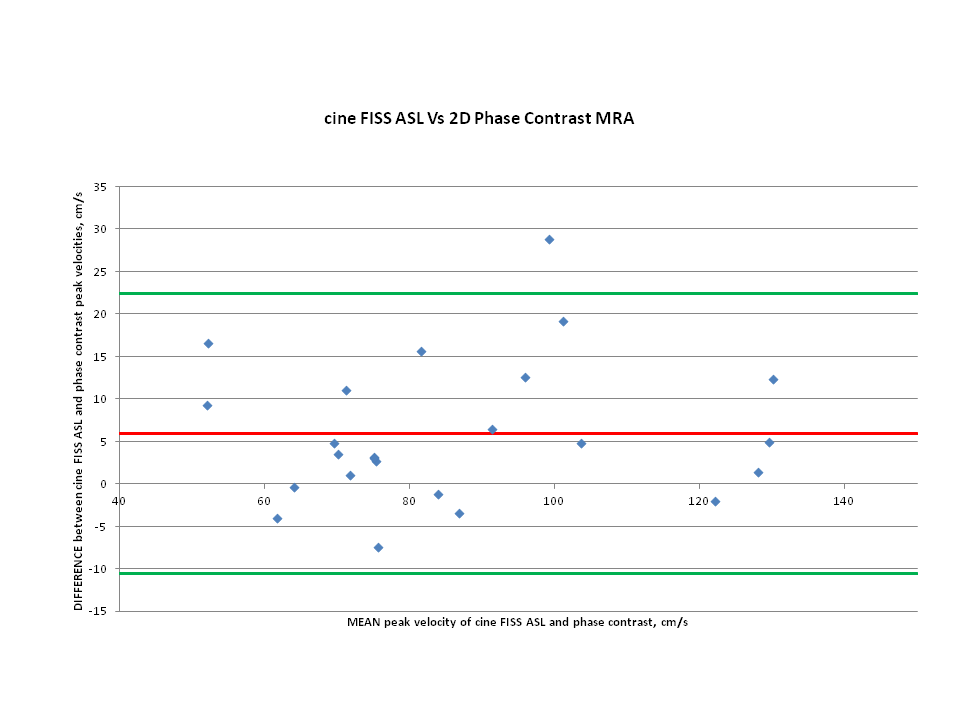
Using cine FISS ASL, in-plane flow patterns were well visualized in all peripheral arterial stations (Figure 1). Unlike 2DPC, cine FISS ASL provided a visually-appealing display of hemodynamic patterns along extensive lengths of the peripheral arteries. There was very strong positive correlation between peak flow velocities measured by cine FISS ASL and 2DPC (r=0.938) (Figure 2). Bland-Altman analysis of reproducibility of cine FISS ASL and 2DPC measurements at all levels revealed a mean velocity difference of 6 cm/s (SD=8.4; 95% limits of agreement -10.5/22.5 cm/s) (Figure 3).Discussion
Our results suggest that non-enhanced cine FISS ASL can efficiently evaluate vascular morphology and flow in the lower extremity peripheral arteries without use of radiation or intravenous contrast. To our knowledge this technique has not previously been described for evaluation of flow in the lower extremities. Although non-contrast 4D flow MRA is also possible in the lower extremities, and has previously been performed in the pelvic and proximal thigh arteries, it is limited in smaller peripheral vessels which require imaging over long segments due to time required for scanning and post-processing.6 Limitations with the cine FISS ASL technique include artifacts from off-resonance effects, respiratory motion and accurate detection of the leading edge of the labeled bolus in very small vessels with rapid flow.Conclusion
This preliminary feasibility study suggests that non contrast cine FISS ASL imaging technique may have a role in non-invasive dynamic lower extremity angiography. It provides an efficient, visually-appealing display of in-plane flow patterns over extensive segments of the lower extremity peripheral arteries without contrast or radiation. Moreover, there was very strong positive correlation and excellent agreement between peak flow velocities measured by cine FISS ASL and 2DPC so it may also provide an alternative to phase contrast imaging for flow quantification in the lower extremities. Further studies will be required to determine the value of this technique in patients with peripheral arterial disease.Acknowledgements
FUNDING SOURCES: NIH grants R01 HL137920 and R01 HL130093
We wish to acknowledge Dr Wei Li and Nondas Leloudas for assisting with data collection and phase contrast analysis.
References
- Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2163–2196.
- Edelman RR, Serhal A, Pursnani A, et al. Cardiovascular cine imaging and flow evaluation using Fast Interrupted Steady-State (FISS) magnetic resonance. J Cardiovasc Magn Reson. 2018; 20(1): 12.
- Koktzoglou I, Edelman RR. Radial fast interrupted steady-state (FISS) magnetic resonance imaging. Magn Reson Med 2018; 79: 2077-86.
- Reimer P, Boos M. Phase-contrast MR angiography of peripheral arteries: technique and clinical application. Eur Radiol 1999; 9: 122-7.
- Steffens JC, Link J, Müller-Hülsbeck S, et al. Cardiac-gated two-dimensional phase-contrast MR angiography of lower extremity occlusive disease. American Journal of Roentgenology 1997; 169: 749-54.
- Frydrychowicz A, Winterer J T, Zaitsev M, et al. Visualization of iliac and proximal femoral artery hemodynamics using time-resolved 3D phase contrast MRI at 3T. Journal of Magnetic Resonance Imaging 2007; 25(5): 1085-92.
Figures