0463
Quantitative Measurements of Carotid Atherosclerotic Plaque Compositions using in vivo T1 Mapping: Validation by Histology1Center for Biomedical Imaging Research, Department of Biomedical Engineering, Tsinghua University School of Medicine, Beijing, China, 2Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 3China National Clinical Research Center for Neurological Diseases, Beijing, China, 4School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 5Department of Neurosurgery, Peking University Third Hospital, Beijing, China, 6Department of Radiology, Peking University Third Hospital, Beijing, China
Synopsis
Plaque compositional features are effective indicators for vulnerability and associated with ischemic stroke risk. Multicontrast vessel wall imaging has been utilized to characterize plaque compositions but this technique is time consuming and dependent on reviewer’s experience. Therefore, it is important to characterize plaque compositions with time-efficient imaging approach. This study sought to determine T1 values of carotid plaque components determined by quantitative imaging validated by histology. We found that the T1 values of intraplaque hemorrhage, necrotic core, and loose matrix were distinguishable. Our findings suggest that carotid plaque components might be distinguishable and automatically segmented on quantitative MR imaging.
Introduction
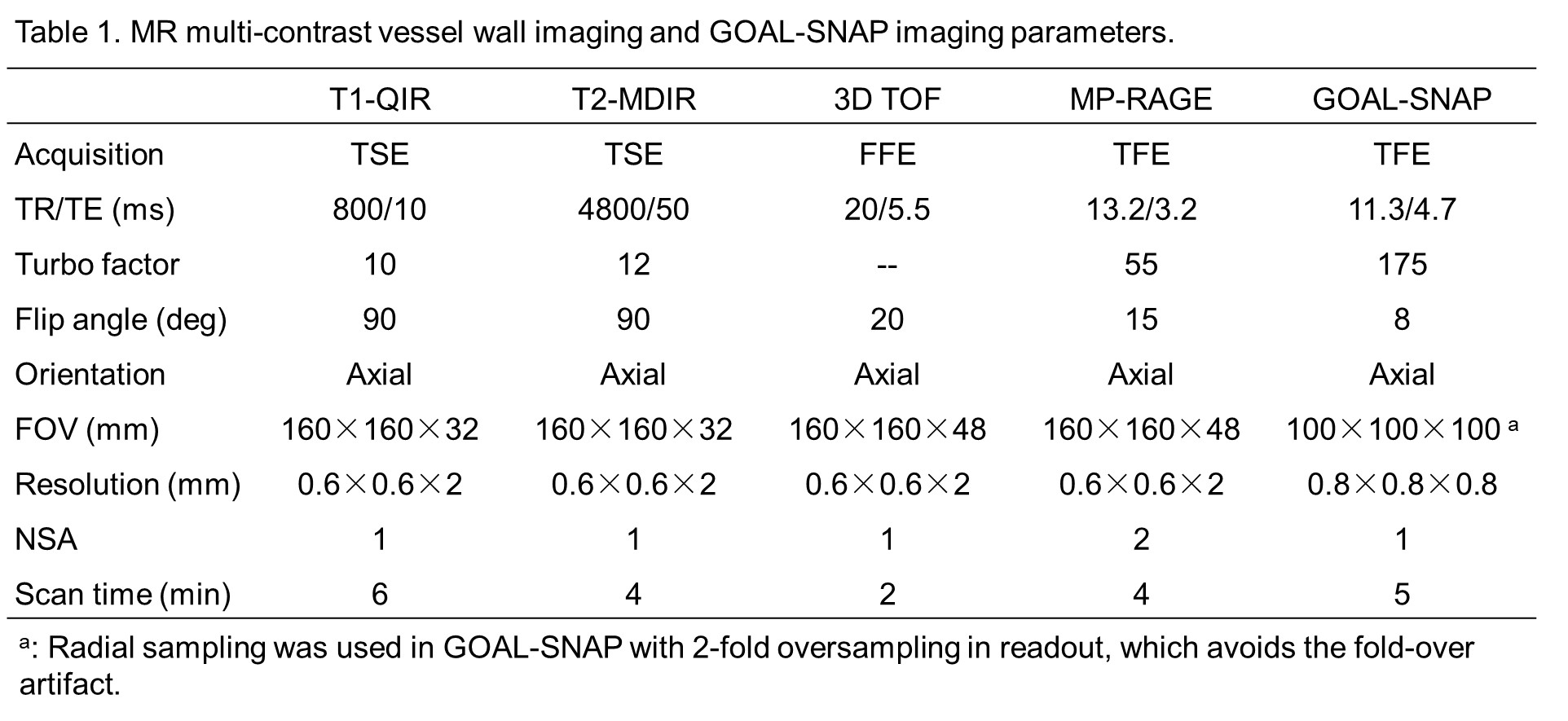
Vulnerability of carotid artery atherosclerotic plaques is associated with ischemic stroke risk. Histologically, vulnerable plaques are characterized by presence of intraplaque hemorrhage (IPH), large lipid-rich necrotic core (LRNC) or fibrous cap rupture.1,2 Therefore, it is important to characterize vulnerable plaques prior to occurrence of events. Currently, MR multi-contrast vessel wall imaging has been demonstrated to be an ideal non-invasive modality to identify plaque compositions.3 However, this technique is time consuming and its quantitative analysis is heavily dependent on reviewer’s experience. Recently, 3D golden angle radial k-space sampling (GOAL-SNAP) has been proposed for vessel wall T1 mapping.4 The T1 mapping may yield more quantitative reproducible features which can be potentially used to identify plaque components. This study sought to determine the T1 values of carotid atherosclerotic plaque components determined by quantitative imaging validated by histology.Methods
Study sample: Fifteen subjects (mean age, 64.5 ± 6.2 years; 13 males) with carotid atherosclerotic disease (50%-70% symptomatic stenosis or >70% stenosis) referred to CEA were enrolled in this study. All the subjects underwent MR imaging within 1 week before CEA surgery. MR imaging: All carotid arteries were imaged on 3.0T MR scanner (Achieva TX, Philips Healthcare) with a custom-designed 36-channel cerebrovascular coil or an 8-channel carotid coil. Multi-contrast MR vessel wall and GOAL-SNAP4 imaging was performed with the parameters detailed in Table 1. The series of GOAL-SNAP images along the IR curve were reconstructed using sliding window and KWIC methods5, similar to the previous study. 4 Then, T1 map can be estimated from the series of IR images.4 Histologic sample processing and analysis: The CEA specimens were fixed in 10% neutral buffered formalin within 4 hours after excision, decalcified in 10% formic acid, and embedded a bloc in paraffin. Sections (10 μm thickness) were excised every 0.5 mm through the length of the specimen and stained with hematoxylin-eosin (H&E). The histologic sections were matched to the MR images by an experienced histologist and a radiologist with consensus base on the features of lumen, wall, and plaque components. Loose matrix (LM), IPH and necrotic core (NC) were identified and quantified on each matched histologic section by an experienced histologist using ImageJ software. The IPHs were classified into two types according to the proportion of area of fresh hemorrhage in the whole area of IPH on each section: type 1, fresh hemorrhage ≥50% of area of IPH; type 2, fresh hemorrhage <50% of area of IPH. Image analysis: The reconstructed GOAL-SNAP images were reformatted to 2 mm axial slices with the same geometry to T1-QIR images for analysis. The boundaries of lumen and wall were outlined on each slice by two radiologists with >5 years’ experience in cardiovascular MR imaging using “CASCADE” (UW, Seattle, USA). T1 fitting was performed on the wall regions. All the marks of LM, IPH and NC, which were identified on histologic sections, were mapped onto the T1 fitting images by the two radiologists. The T1 value of intraplaque calcification was not calculated due to poor reliability. Statistical analysis: The T1 values of LM, IPH (two types) and NC were calculated and compared using Mann-Whitney U test.Results
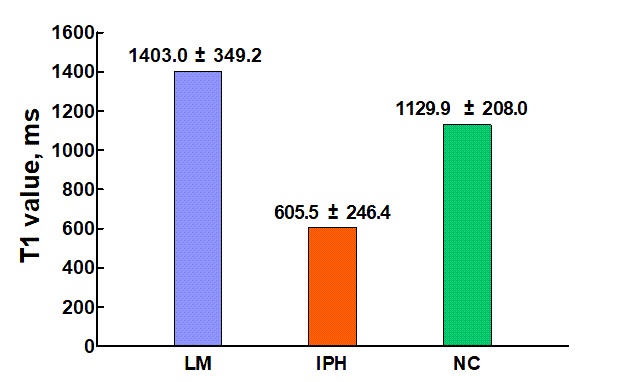
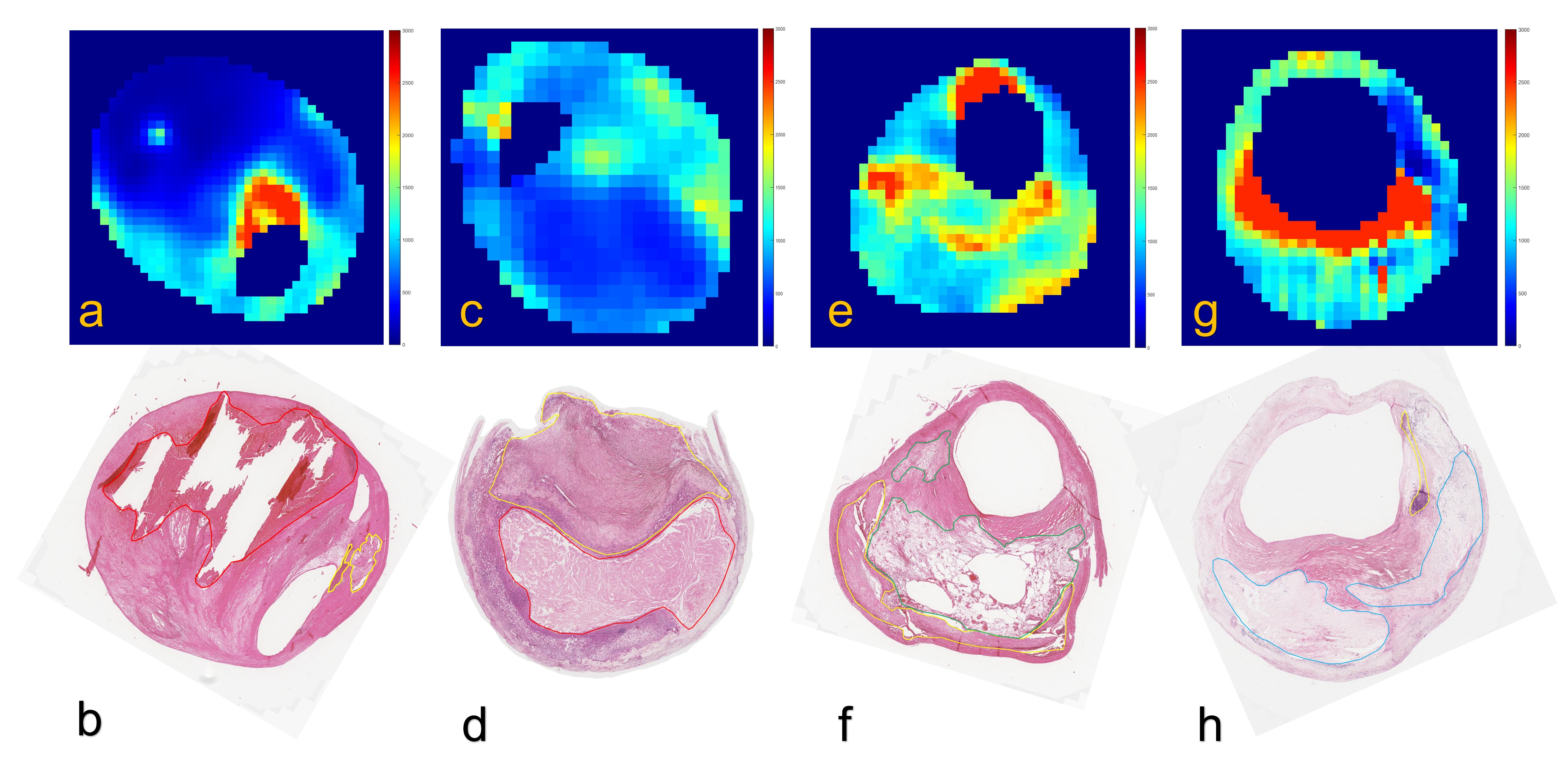
In 15 patients, 44 slices with acceptable image quality were included in analysis. Of 44 slices, 20 (45.5%) had LM, 29 (65.9%) had IPH, and 26 (59.1%) had NC on histology. The mean T1 value of IPH, NC, and LM was 605.5 ± 246.4 ms, 1129.9 ± 208.0 ms, and 1403.0 ± 349.2 ms, respectively (all p <0.01, Fig. 1). Of 29 slices with IPH, 11 (37.9%) were classified into type 1 and 18 were classified into type 2. The T1 value for type 1 and type 2 IPH was 363.1 ± 141.0 ms and 753.6 ± 164.5 ms, respectively (p <0.001). Typical carotid atherosclerotic plaque images with LM, IPH and NC on both histologic sections and T1 fitting images are shown in Fig. 2.Discussion and Conclusion
This study investigated the T1 values of carotid plaque components validated by histology. We found that the T1 values of different plaque components including intraplaque hemorrhage, necrotic core, and loose matrix were distinguishable. In addition, the fresh intraplaque hemorrhage had significantly lower T1 values than old intraplaque hemorrhage. Our findings suggest that carotid plaque components might be distinguishable and automatically segmented on quantitative MR imaging.Acknowledgements
NoneReferences
1. Zavodni AE, Wasserman BA, McClelland RL, et al. Carotid artery plaque morphology and composition in relation to incident cardiovascular events: the Multi-Ethnic Study of Atherosclerosis (MESA). Radiology. 2014;271:381-389.
2. Saam T, Hetterich H, Hoffmann V, et al. Meta-analysis and systematic review of the predictive value of carotid plaque hemorrhage on cerebrovascular events by magnetic resonance imaging. J Am Coll Cardiol. 2013;62:1081-1091.
3. Cai JM, Hatsukami TS, Ferguson MS, et al. Classification of human carotid atherosclerotic lesions with in vivo multicontrast magnetic resonance imaging. Circulation. 2002;106:1368-1373.
4. Qi H, Sun J, Qiao H, et al. Carotid Intraplaque Hemorrhage Imaging with Quantitative Vessel Wall T1 Mapping: Technical Development and Initial Experience. Radiology. 2018;287:276-284.
5. Neumann D, Breuer FA, Völker M, et al. Reducing contrast contamination in radial turbo-spin-echo acquisitions by combining a narrow-band KWIC fi lter with parallel imaging. Magn Reson Med. 2014;72:1680-1686.
Figures