0460
XD-ORCCA for BOOST: accelerated motion-compensated simultaneous bright- and black-blood 3D whole-heart coronary MRI1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Frimley, United Kingdom
Synopsis
Recently, a novel free-breathing 3D whole-heart sequence, called T2-prepared BOOST, was proposed for non-contrast enhanced bright-blood and black-blood coronary MR imaging, for simultaneous coronary lumen and coronary thrombus/ intraplaque hemorrhage visualization. However, high-resolution fully-sampled BOOST acquisitions require long scan times of ~20min. Here, we propose to use a modified version of XD-ORCCA, a highly efficient respiratory-resolved motion-corrected framework, to accelerate BOOST acquisitions. XD-ORCCA exploits the sparsity in a motion-corrected domain to acquire high-quality respiratory-resolved bright- and black-blood BOOST images in ~6min. Hence, high-resolution free-breathing BOOST imaging is achieved within clinically feasible acquisition times.
Introduction
MRI has shown great potential for noninvasive detection of coronary luminal stenosis1 and high-risk plaque characteristics, such as intra-plaque hemorrhage and thrombus.2 Bright-blood coronary MR angiography (CMRA) and black-blood T1-weighted acquisitions are usually performed sequentially for coronary lumen and thrombus/hemorrhage visualization, respectively. Moreover, to reduce respiratory motion artifacts in free-breathing 3D whole-heart acquisitions, 1D diaphragmatic navigator gating and tracking is commonly used, leading to long and unpredictable scan times.3
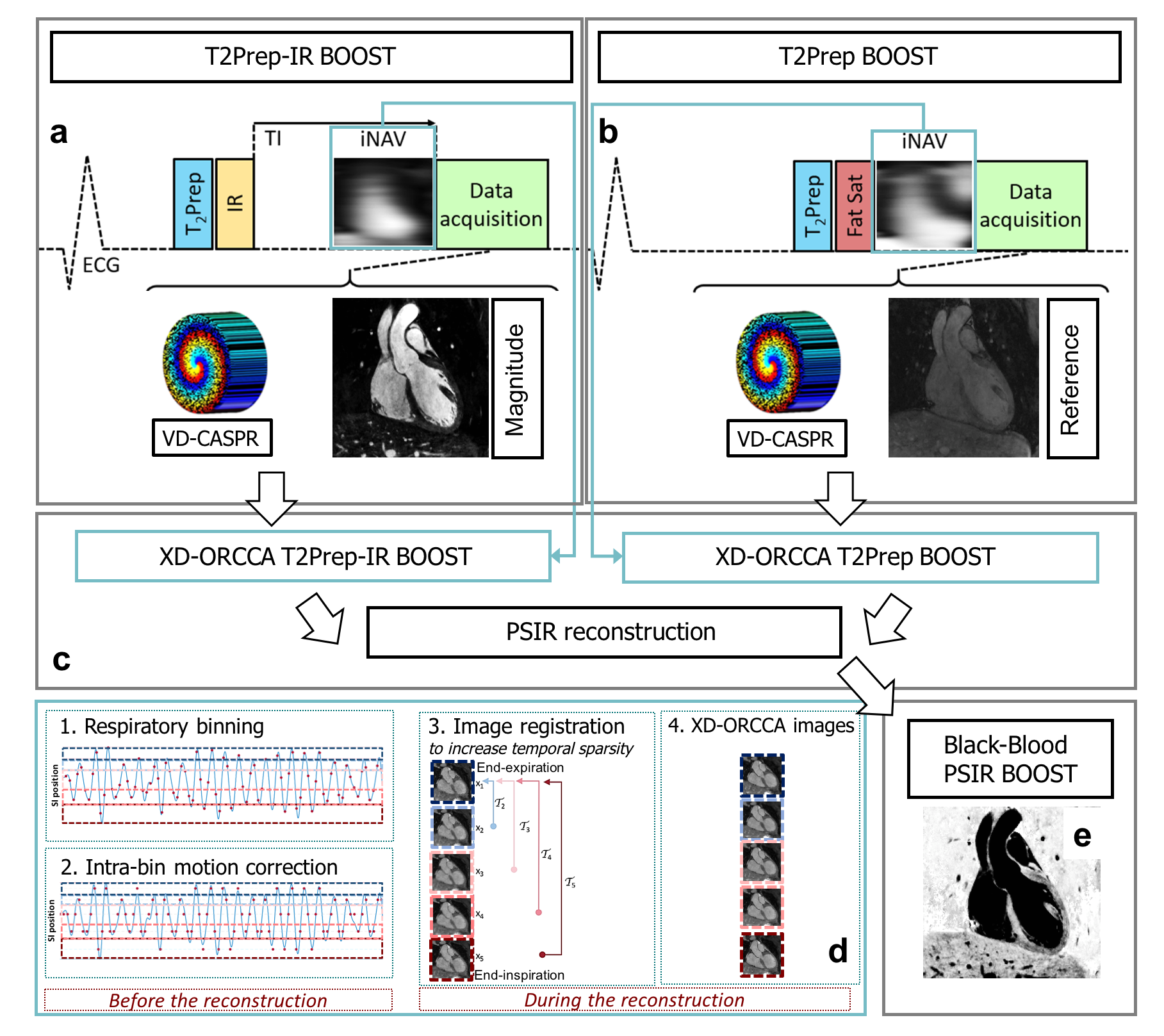
Recently, the 3D T2-prepared whole-heart Bright-blood and black-blOOd phase SensiTive (T2-prepared BOOST)4 inversion recovery sequence has been proposed for simultaneous non-contrast enhanced coronary lumen and thrombus/hemorrhage visualization. This free-breathing sequence alternates between a bright-blood T2-prepared Inversion Recovery (T2Prep-IR) and a bright-blood T2-prepared (T2Prep) 3D whole-heart acquisition. These datasets are combined in a phase-sensitive inversion recovery (PSIR)-like reconstruction, to obtain a co-registered black-blood volume (Fig. 1). Additionally, 2D image navigators (iNAVS)5 are used to correct for translational respiratory motion and to obtain co-registered images within a predictable scan time. However, high-resolution fully-sampled T2-prepared BOOST still requires long acquisition times of ~20min. Here, we propose to accelerate T2-prepared BOOST to a clinically feasible timeframe (<10min). This is achieved by extending a robust and highly efficient respiratory-resolved motion-corrected framework (XD-ORCCA),6 which was originally proposed for fully-sampled 3D Cartesian CMRA. This method uses translational motion information from 2D iNAVS to increase the sparsity in the respiratory dimension and to compensate for residual motion within each respiratory bin (Fig. 1). The proposed method was tested in six healthy subjects for different acceleration factors.
Methods
Accelerated 3D T2-prepared BOOST uses a prototype variable-density Cartesian trajectory with spiral profile order (VD-CASPR),7,8 which samples the ky-kz plane with spiral interleaves on a Cartesian grid with variable density sampling along each spiral arm. The BOOST sequence alternates the acquisition of a T2Prep-IR module in odd heartbeats and a T2Prep module in even heartbeats. Low-resolution 2D iNAVs are acquired at every heartbeat, before each spiral interleaf of the 3D BOOST acquisition. The 2D iNAVS are used to estimate beat-to-beat 2D translational motion (superior-inferior: SI and left-right) and obtain the respiratory signal, which is used to distribute each BOOST dataset into five equally populated respiratory bins (Fig. 1). Respiratory-resolved images $$$\mathbf{x}$$$ for each BOOST dataset are obtained by solving a modified version of XD-ORCCA: $$$\hat{\mathbf{x}}=\arg\min\limits_{\mathbf{x}}\left\{\frac{1}{2}\left\|\mathbf{E}\mathbf{x}-\mathbf{d}\right\|^2_2+\alpha\,\Psi_{\textrm{t}}\left(\mathcal{R}\mathbf{x}\right)+\beta \,\Psi_{\textrm{-t}}\left(\mathcal{R}\mathbf{x}\right)+\gamma \,\Psi_{\textrm{s}}\left(\mathbf{x}\right) \right\}$$$, where $$$\mathbf{d}$$$ are the undersampled 2D intra-bin translational motion-corrected k-space data, $$$\Psi_{\textrm{s}}$$$ is the 3D spatial total variation (TV) function, $$$\alpha$$$, $$$\beta$$$ and $$$\gamma$$$ are regularization parameters, $$$\mathcal{R}\mathbf{x}=\mathcal{T}_b\mathbf{x}_b$$$ is the translational motion-corrected domain, where $$$\mathcal{T}_b$$$ is the 2D translation transform that maps the respiratory bin image $$$\mathbf{x}_b$$$ to the reference image $$$\mathbf{x}_1$$$ (end-expiration), $$$\Psi_{\textrm{t}}=\left\| \mathcal{T}_b\mathbf{x}_b - \mathcal{T}_{b+1}\mathbf{x}_{b+1}\right\|_1$$$ and $$$\Psi_{\textrm{-t}}=\left\| \mathcal{T}_b\mathbf{x}_b -\mathcal{T}_{b-1}\mathbf{x}_{b-1}\right\|_1$$$ are 1D temporal TV functions. The operator $$$\mathbf{E}=\mathbf{A}_b\mathbf{FS}$$$ incorporates the sampling matrix $$$\mathbf{A}_b$$$ for each bin $$$b$$$, Fourier transform $$$\mathbf{F}$$$ and coils sensitivities $$$\mathbf{S}$$$.
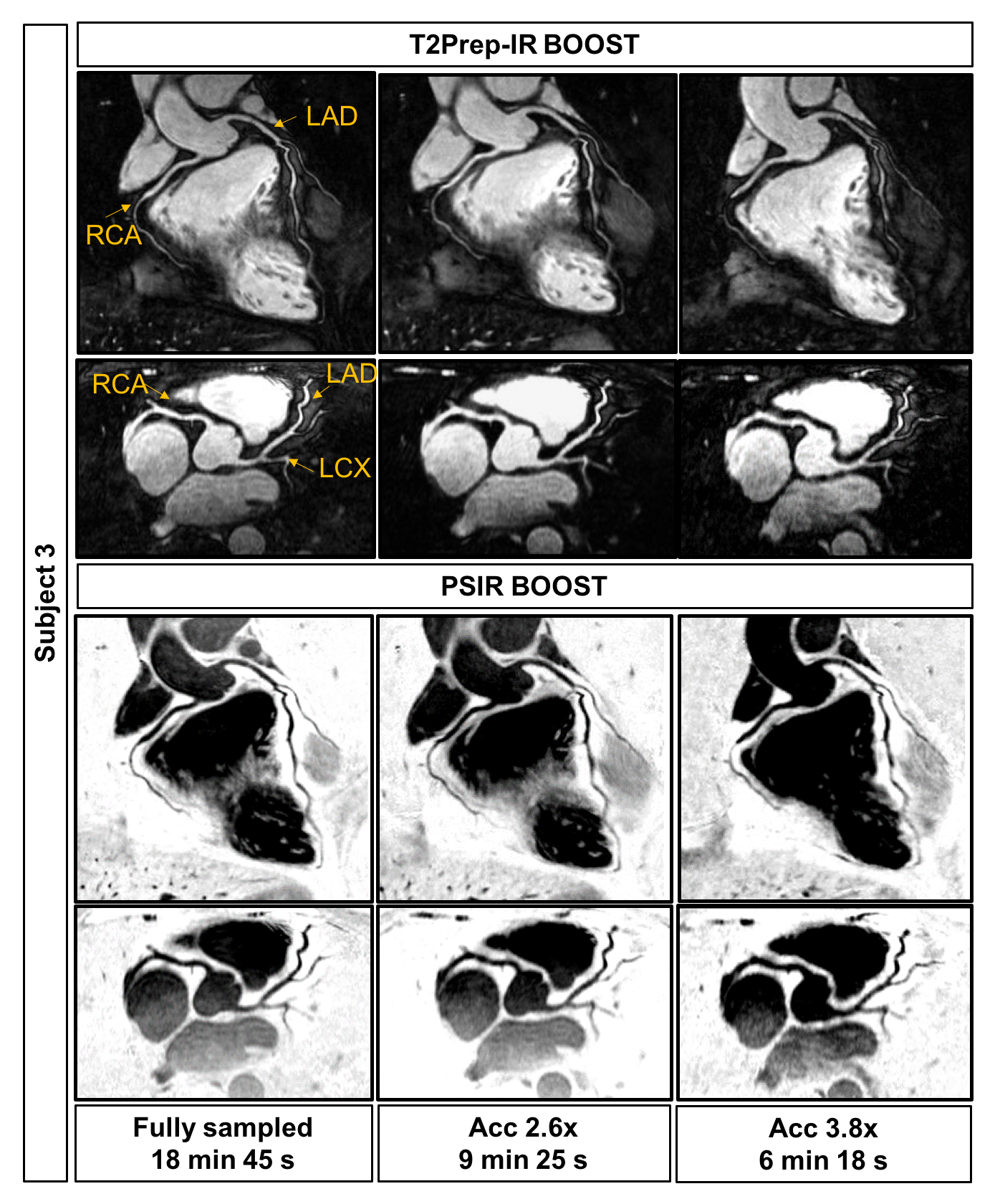
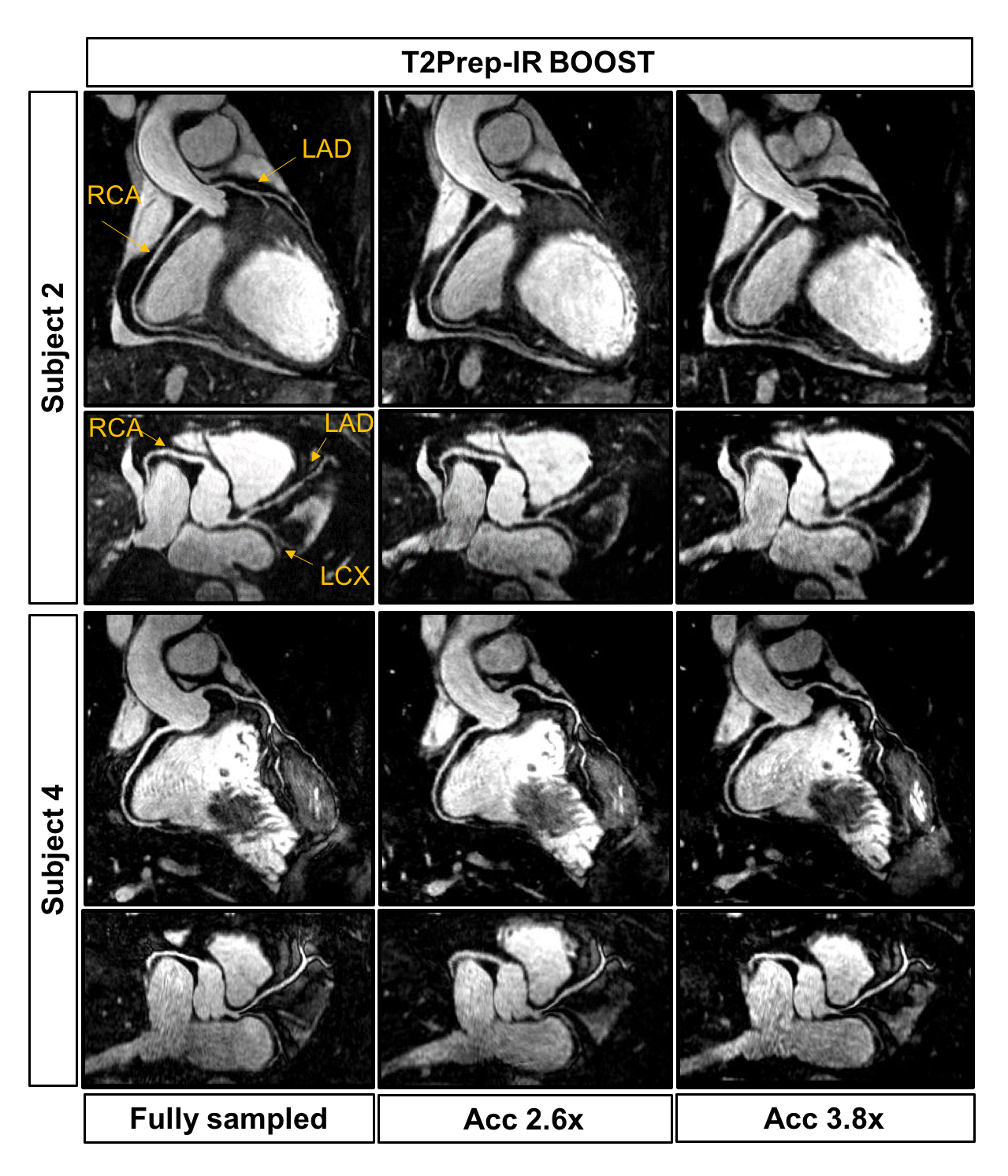
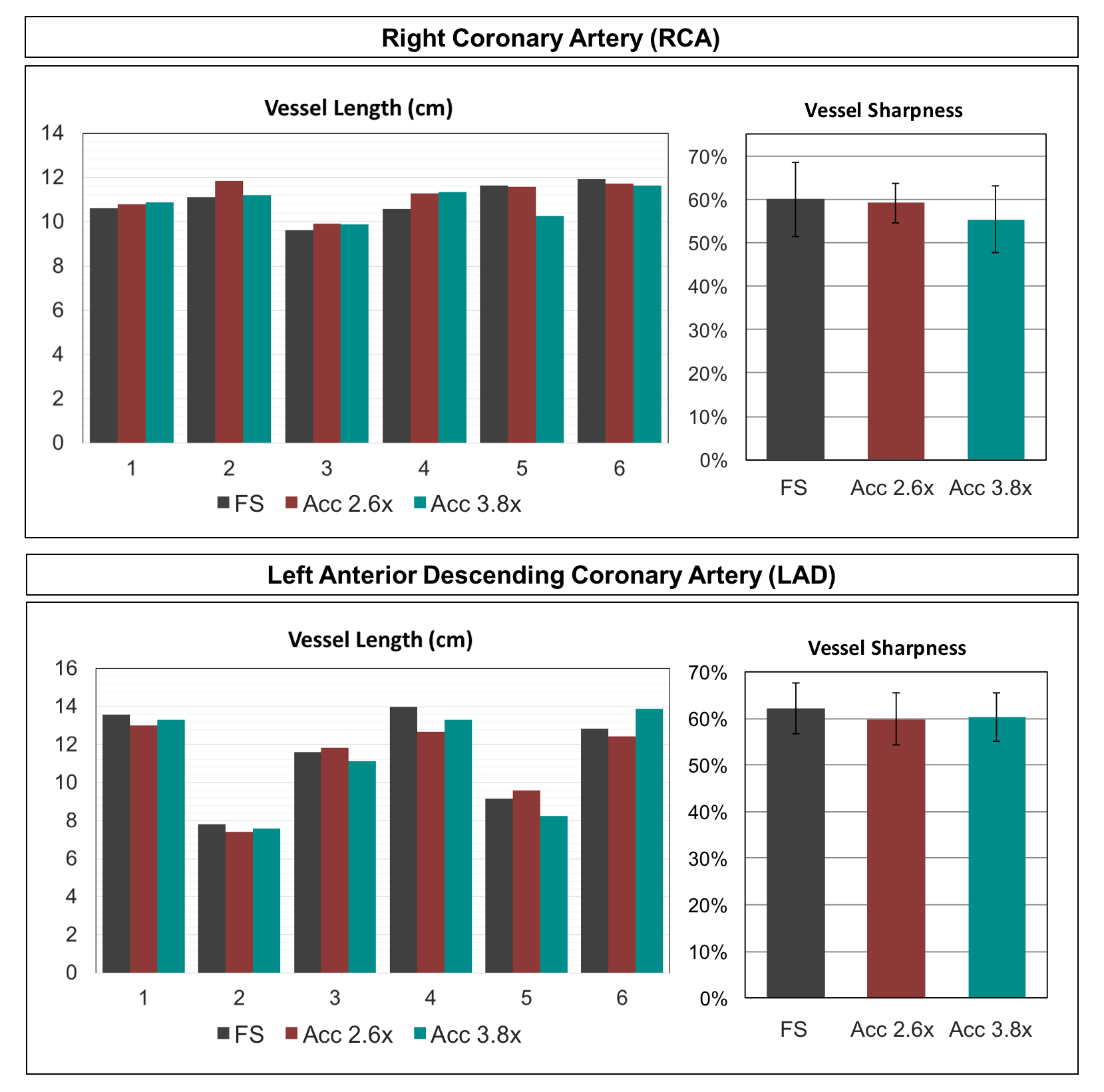
In-vivo free-breathing experiments were performed in six healthy subjects on a 1.5T scanner (Siemens Magnetom Aera). Fully-sampled BOOST (with elliptical shutter, ~18min), 2.6x (~9min) and 3.8x (~6min) accelerated acquisitions were performed for each subject using the following parameters: coronal orientation, FOV=320x320x96-112mm3, resolution=1x1x2mm3, TR/TE=3.6/1.56ms, flip angle=90°, TI=110ms, T2-prep=40ms, 2D iNAV with 14 bSSFP startup echoes. Coronary vessel sharpness and length were quantified for all acquisitions in the bright blood images using SoapBubble.9
Results
Reformatted bright- and black-blood images obtained with XD-ORCCA (respiratory bin with the smallest SI respiratory displacements) are displayed in Fig. 2 for a representative healthy subject. Moreover, Fig. 3 shows the T2Prep-IR (bright-blood) reformatted images obtained for two subjects. Coronal views of T2Prep-IR and PSIR BOOST images are shown in Fig. 4 for another subject. The proposed method produces images from accelerated acquisitions with comparable quality to those obtained from fully-sampled acquisitions. No significant differences in the vessel length and sharpness were identified for both coronary arteries between the fully-sampled reference images and the images obtained from undersampled data (Fig. 5).Conclusions
The proposed framework provides high‐resolution, motion‐compensated non-contrast enhanced 3D whole-heart bright-blood and black-blood images, for thrombus and coronary lumen visualization, from a single free-breathing acquisition in a clinically feasible scan time of about 6min. This was achieved by combining the XD-ORCCA respiratory-resolved reconstruction approach with 3D whole-heart Cartesian BOOST undersampled acquisitions. Future work will include the evaluation of this approach in patients with acute coronary syndrome and coronary artery plaques.Acknowledgements
This work was supported by EPSRC (EP/L015226/1, EP/P001009, EP/P007619, EP/P032311/1) and Wellcome EPSRC Centre for Medical Engineering (NS/A000049/1)References
1. Kim WY, Danias PG, Stuber M, Flamm SD, Plein S, Nagel E, Langerak SE, Weber OM, Pedersen EM, Schmidt M, Botnar RM, Manning WJ. Coronary magnetic resonance angiography for the detection of coronary stenosis. N Engl J Med 2001; 345:1863-1869
2. Jansen CH, Perera D, Makowski MR, Wiethoff AJ, Phinikaridou A, Razavi RM, Marber MS, Greil GF, Nagel E, Maintz D, Redwood S, Botnar RM. Detection of intracoronary thrombus by magnetic resonance imaging in patients with acute myocardial infarction. Circulation 2011; 124:416-24.
3. Ehman RL, Felmlee JP. Adaptive technique for high‐definition MR imaging of moving structures. Radiology 1989; 173:255–263.
4. Ginami G, Neji R, Phinikaridou A, Whitaker J, Botnar RM, Prieto C. Simultaneous bright- and black-blood whole-heart MRI for noncontrast enhanced coronary lumen and thrombus visualization. Magn Reson Med 2018; 79:1460-1472.
5. Henningsson M, Koken P, Stehning C, Razavi R, Prieto C, Botnar RM. Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magn Reson Med 2012; 67:437-445.
6. Correia T, Ginami G, Cruz G, Neji R, Rashid R, Botnar RM, Prieto C. Optimized respiratory‐resolved motion‐compensated 3D Cartesian coronary MR angiography. Magn Reson Med 2018; 80:2618-2629.
7. Correia T, Cruz G, Schneider T, Botnar RM, Prieto C. Accelerated nonrigid motion-compensated isotropic 3D coronary MR angiography. Med Phys 2018; 45:214-222.
8. Bustin A, Ginami G, Cruz G, Correia T, Ismail T, Rashid I, Neji R, Botnar RM, Prieto C. Five-minute whole-heart coronary MRA with sub-millimeter isotropic resolution, 100% respiratory scan efficiency, and 3D-PROST reconstruction. Magn Reson Med 2018; 80:2618-2629.
9. Etienne A, Botnar RM, Van Muiswinkel AM, Boesiger P, Manning WJ, Stuber M. Soap‐Bubble visualization and quantitative analysis of 3D coronary magnetic resonance angiograms. Magn Reson Med. 2002; 48:658‐666.
Figures