0459
Fat-free free-running coronary MRA at 1.5T using LIBRE water excitation pulses1Department of Radiology, Lausanne University Hospital (CHUV) and University of Lausanne (UNIL), Lausanne, Switzerland, 2Advanced Clinical Imaging Technology, Siemens Healthcare AG, Lausanne, Switzerland, 3LTS5, Ecole Polytechnique Fédérale de Lausanne (EPFL), Lausanne, Switzerland, 4Center for Biomedical Imaging (CIBM), Lausanne, Switzerland
Synopsis
Previously published work in fully self-gated free-breathing 3D radial coronary MRA at 1.5T with cardiac-and-respiratory-motion-resolved reconstruction (Free-running framework) suffered from the disadvantage of requiring interrupted bSSFP with ramp-up and fat saturation pre-pulses. Using numerical simulations, in vitro and in vivo scans, we successfully tested the hypothesis that LIBRE, a new water excitation technique, obviates the need for such pre-pulses, improves time efficiency when compared to earlier approaches, and provides both superior fat saturation and vessel delineation relative to more conventional water excitation.
Introduction
For visualization of the coronary arteries, fully self-gated free-breathing 3D radial data acquisition with cardiac-and-respiratory-motion-resolved reconstruction (=Free-running framework) has been previously implemented using a periodically interrupted balanced steady-state free precession (bSSFP) sequence with ramp-up and fat saturation pre-pulses1,2. The disadvantages of such an approach include sub-optimal fat suppression, increased specific absorption rate (SAR), and scan time inefficiency2. Lipid-insensitive binomial off-resonant RF excitation (LIBRE) is a new broadband fat suppression technique3,4. LIBRE was shown to null lipid signal and improve vessel detection in ECG-triggered coronary MR angiography (cMRA) at 3T using GRE5, indicating potential for bSSFP cMRA. Therefore, we tested the hypothesis that LIBRE improves time efficiency when compared to earlier approaches, and that, compared to both no fat suppression and 1-2-1 water excitation, it better attenuates fat signal and improves vessel sharpness in uninterrupted bSSFP for free-running cMRA at 1.5T.Methods
Bloch equation simulations
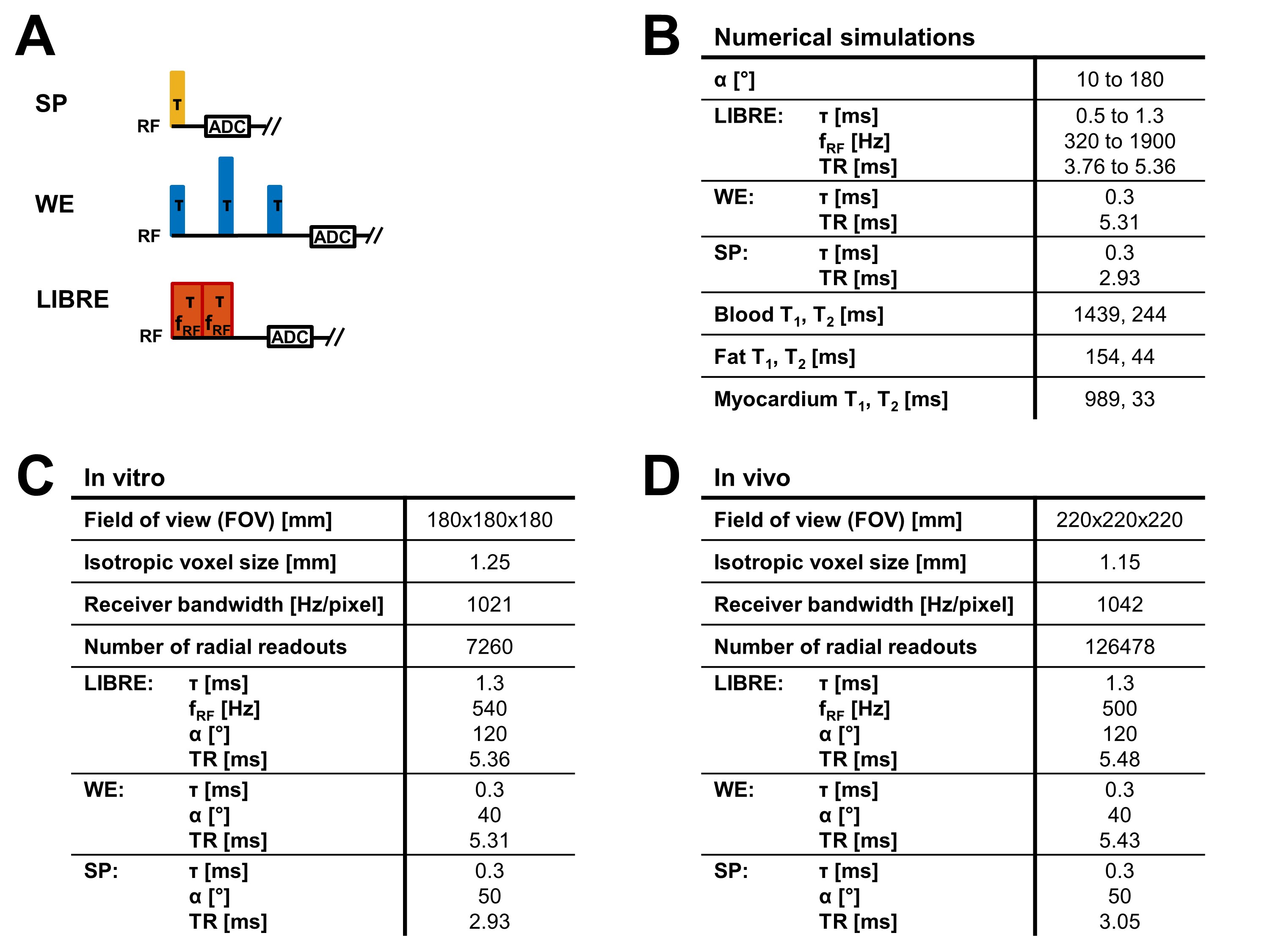
The LIBRE pulse consists of two rectangular pulses having variable off-resonance RF frequency (fRF), subpulse duration (τ), and RF excitation angle (α)3.
Bloch equation simulations were performed to determine the LIBRE parameters (fRF, τ, α) that maximize blood-fat contrast in bSSFP, while ensuring the simulated range for the repetition time (TR) was <6ms to minimize the risk of banding artefacts6 in the heart. For a non-fat suppressing rectangular excitation pulse (SP), spectrally-selective 1-2-1 water excitation (WE), and LIBRE (Fig. 1A), the steady-state transverse magnetization was simulated for blood, fat, and myocardium (parameters in Fig. 1B). WE and SP were optimized for blood-fat contrast and blood signal, respectively.
Phantom experiments
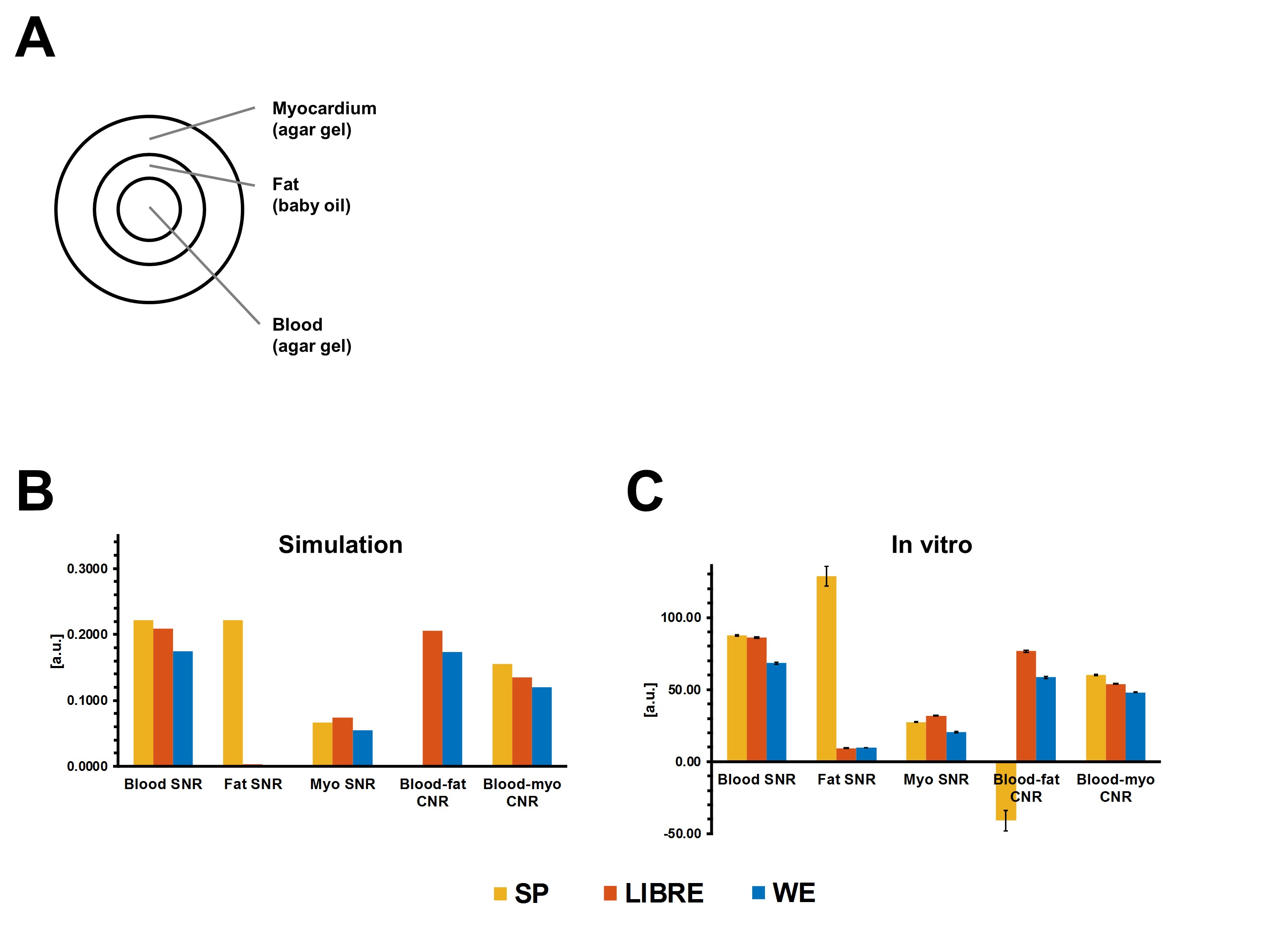
To validate the numerically optimized LIBRE parameters, scans were performed on a phantom containing blood, fat, and myocardial tissue compartments (Fig. 3A). Six runs for LIBRE, WE, and SP were performed at 1.5T (MAGNETOM Aera, Siemens Healthcare AG, Erlangen, Germany) with a prototype 3D radial7 bSSFP sequence (parameters in Fig. 1B).
Signal-to-noise ratios (SNRs) and contrast-to-noise ratios (CNRs) were calculated for the different compartments.
Volunteer experiments
The validated LIBRE parameters were implemented as part of a free-running cMRA sequence and applied to 13 healthy adult volunteers. Scans were performed using a 3D radial bSSFP sequence8 (same as above) using LIBRE, WE, and SP at 1.5T (parameters in Fig. 1C). Scan time and specific absorption rate (SAR) were recorded. Cardiac-and-respiratory-motion-resolved 3D images were then reconstructed using compressed sensing as described previously9,10.
A 3D volume corresponding to mid-diastole and end-expiration was retrospectively extracted from each dataset. The number of volunteers in whom a proximal ≥2cm segment of the right coronary artery (RCA) was visually identified were counted for LIBRE, WE, and SP, and RCA vessel length and sharpness of these datasets were determined using SoapBubble11. Statistical significance was assessed using a two-tailed paired t-test (p<0.05 considered significant).
Results
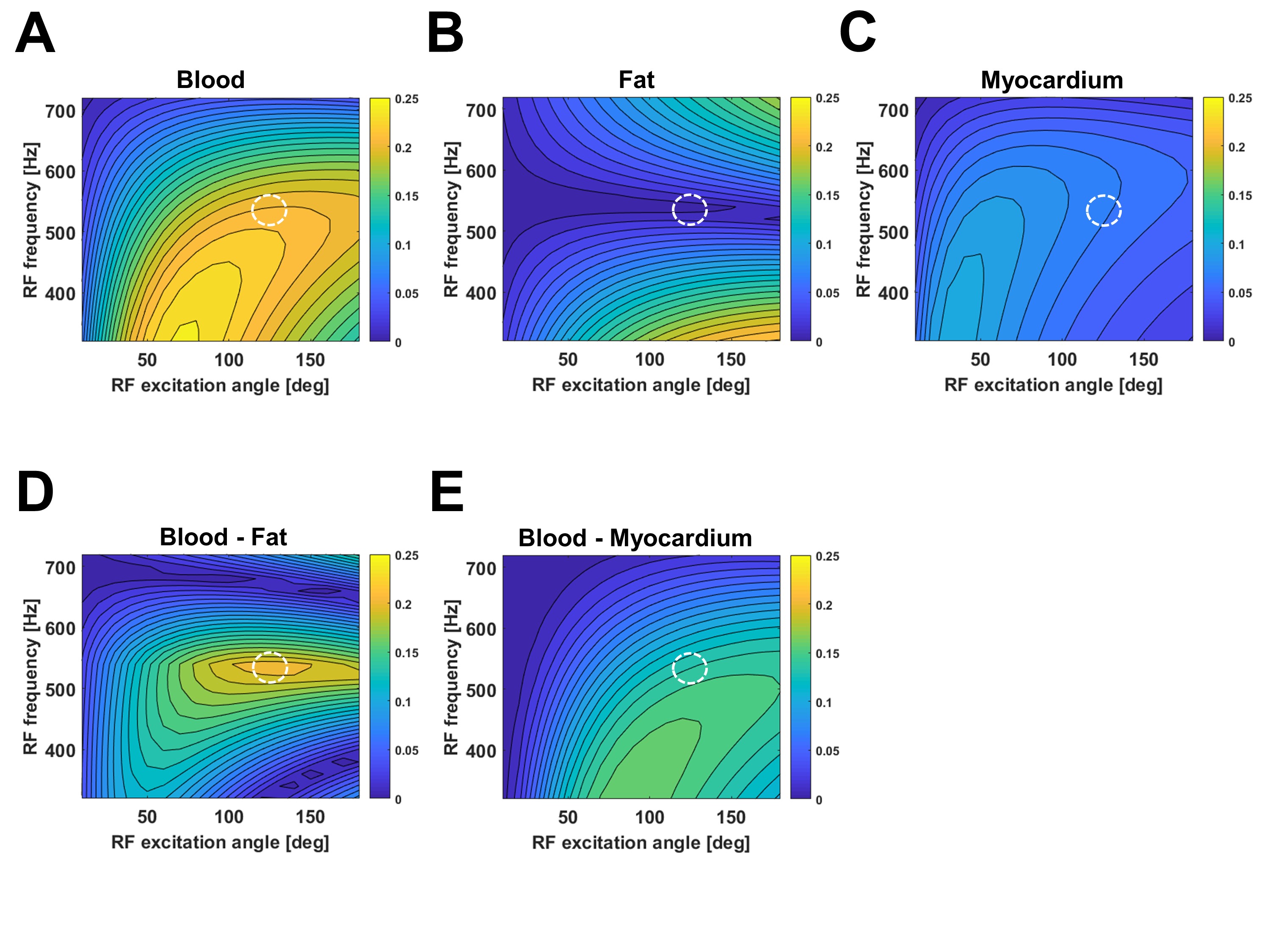
Numerical simulations determined that the optimal LIBRE parameters are τ=1.3ms, fRF=540Hz, and α=120°, which maximized blood-fat contrast (Fig. 2D) and did not compromise performance for other signal criteria (Fig. 2A,B,C,E). The results of the comparison of the optimized LIBRE, SP, and WE pulses were highly consistent between simulations and in vitro scans (Fig. 3B,C); LIBRE was the only pulse that simultaneously provided high blood signal and fat suppression.
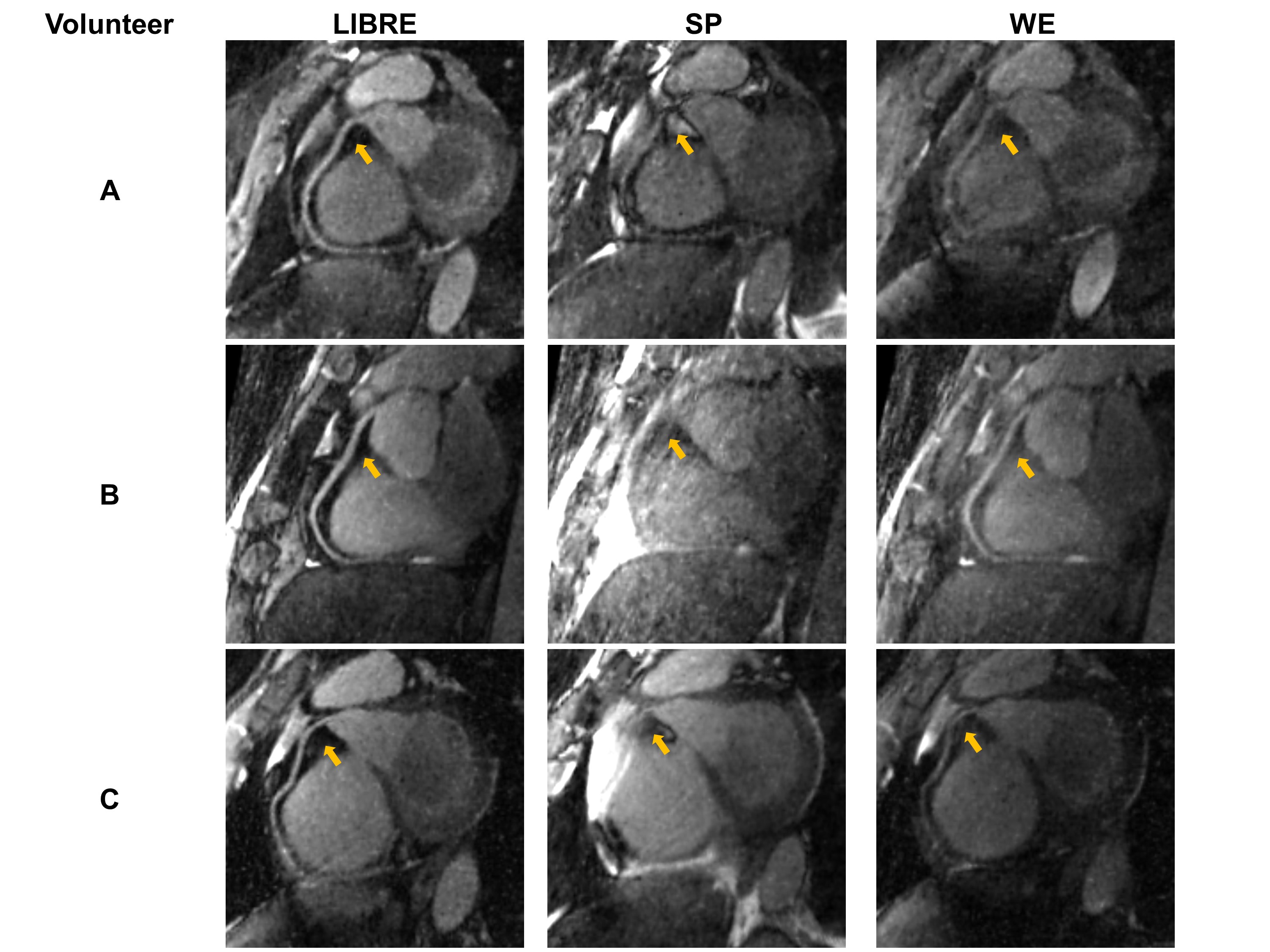
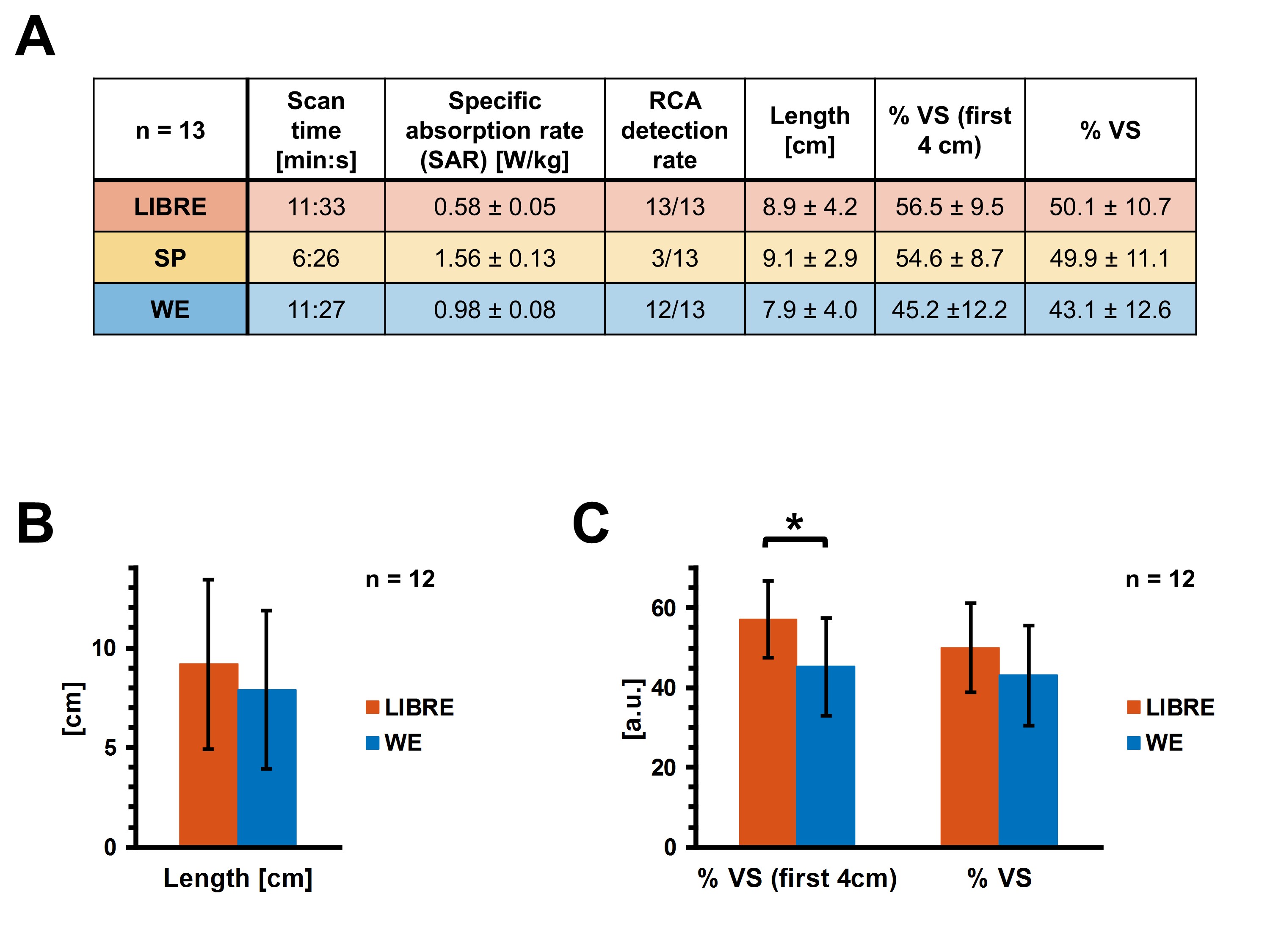
In vivo, acquisition times were 11min33s for LIBRE, 11min27s for WE, and 6min26s for SP (Fig. 5A). LIBRE SAR was significantly lower than that of SP and WE (p<0.001, Fig. 5A), while LIBRE provided effective epicardial fat suppression and improved RCA vessel delineation (Fig. 4) compared to WE and SP. LIBRE was the only pulse with which the RCA was detected in all volunteers (Fig. 5A), and had significantly higher vessel sharpness in the first 4cm than WE (p=0.006, Fig. 5C).
Discussion
Numerical optimization of LIBRE provided a framework that was successfully validated in vitro and informed the parameters for subsequent in vivo scans. Compared to SP and WE, LIBRE (Fig. 2) consistently provided both high blood signal and fat suppression in simulations and in vitro (Fig. 3). In vivo, LIBRE critically enabled delineation of the RCA in all volunteers, and provided significantly higher vessel sharpness than WE (Fig. 4). Notably, LIBRE SAR was significantly lower than that of SP and WE, due to its long pulse duration, and was 85% lower than that of the previously published interrupted bSSFP protocol1. When compared to the latter, LIBRE also supports anatomical and functional imaging albeit at a 19%-reduced scanning time. The scan time depends only on TR and is independent of physiological parameters.Conclusions
The LIBRE pulse was numerically optimized for blood-fat contrast in bSSFP, validated in vitro, and shown to improve vessel sharpness in in vivo free-running bSSFP cMRA at 1.5T, while SAR was reduced and time efficiency improved compared to previously published work.Acknowledgements
No acknowledgement found.References
1. Coppo S, Piccini D, Bonanno G, et al. Free-Running 4D Whole-Heart Self-Navigated Golden Angle MRI: Initial Results. Magn Res Med. 2015; 74:1306–1316.
2. Feng L, Coppo S, Piccini D, et al. 5D Whole-Heart Sparse MRI. Magn Res Med. 2018; 79:826–838. DOI: 10.1002/mrm.26745.
3. Bastiaansen J A M, and Stuber M. Flexible water excitation for fat-free MRI at 3 Tesla using lipid insensitive binomial off-resonant RF excitation (LIBRE) pulses. Magn Res Med. 2018; 79:3007–3017. DOI: 10.1002/mrm.26965.
4. Colotti R, Omoumi P, van Heeswijk R. B., et al. Simultaneous Fat-Free Isotropic 3D Anatomical Imaging and T2 Mapping of Knee Cartilage With Lipid-Insensitive Binomial Off-Resonant RF Excitation (LIBRE) Pulses. J Magn Reson Imaging. 2018; DOI: 10.1002/jmri.26322.
5. Bastiaansen J A M, Piccini D, van Heeswijk R, et al. Lipid insensitive free-breathing self-navigated coronary MR angiography at 3T using a novel water excitation method. Soc Card Magn Res. 2017.
6. Bieri O and Scheffler K. Fundamentals of Balanced Steady-State Free Precession MRI. J Magn Res Imaging. 2013; 38:2-11.
7. Piccini D, Littmann A, Nielles-Vallespin S, et al. Spiral Phyllotaxis: The Natural Way to Construct a 3D Radial Trajectory in MRI. Magn Res Med. 2011; 66:1049–1056.
8. Piccini D, Monney P, Sierro C, et al. Respiratory Self-navigated Postcontrast Whole-Heart Coronary MR Angiography: Initial Experience in Patients. Radiology. 2014; 270(2):378-386.
9. Di Sopra L, Piccini D, Coppo S, et al. Motion-resolved 5D imaging of the heart: time to get rid of the ECG? Intl Soc Magn Res Med. 2017.
10. Feng L, Axel L, Chandarana H, et al. XD-GRASP: Golden-Angle Radial MRI with Reconstruction of Extra Motion-State Dimensions Using Compressed Sensing. Magn Res Med. 2016; 75:775–788.
11. Etienne A, Botnar R M, van Muiswinkel A M C, et al. “Soap-Bubble” Visualization and Quantitative Analysis of 3D Coronary Magnetic Resonance Angiograms. Magn Res Med. 2002; 48:658–666.
Figures