0458
Dual-echo 2D Image Navigators for Respiratory Motion-Corrected Whole-Heart Water/Fat CMRA1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare GmbH, Frimley, United Kingdom
Synopsis
Whole-heart water/fat coronary MR angiography (CMRA) is a promising technique for improved visualisation of the cardiac anatomy and epicardial and pericardial fat. However, respiratory motion remains a challenge for its integration into clinical routine. Here we propose a respiratory motion-corrected whole-heart water/fat CMRA approach based on dual-echo 2D image navigators (iNAVs) and a combined 2D translational and 3D non-rigid motion corrected reconstruction scheme. Results from healthy subjects indicate that out-of-phase iNAVs produce accurate respiratory translational motion estimation, and that motion-corrected water/fat CMRA images are comparable to reference diaphragmatic-gated images, but are acquired in a significantly shorter scan time.
Introduction
Whole-heart water/fat coronary MR angiography (CMRA) imaging has shown potential for better depiction of the coronary arteries by improving fat suppression and enhancing visualization of the cardiac anatomy in the water images, while simultaneously providing a complementary fat image that carries additional diagnostic information1. Recent studies have suggested that increased pericoronary adipose tissue is associated with increased risk of adverse cardiovascular events2. Despite the potential of water/fat CMRA, current approaches have relied on conventional 1D diaphragmatic respiratory gating to enable whole-heart imaging1,3, resulting in long and unpredictable examination times, and therefore preventing widespread clinical translation.
Here we extend our recently proposed image-navigator (iNAV)-based beat-to-beat translational plus bin-to-bin non-rigid respiratory motion correction approach4-5 to a dual-echo 3D water/fat CMRA approach. The acquisition includes a 2D dual-echo iNAV, which enables 100% respiratory scan efficiency (no data rejection) and predictable scan time. These dual-echo 2D iNAVs provide in-phase, out-of-phase, water and fat low-resolution images from which translational respiratory motion can be estimated. In this work, the accuracy of the 2D translational motion estimated from each of these four iNAVs was investigated, in order to find the best iNAV for respiratory motion-corrected water/fat CMRA.
Methods
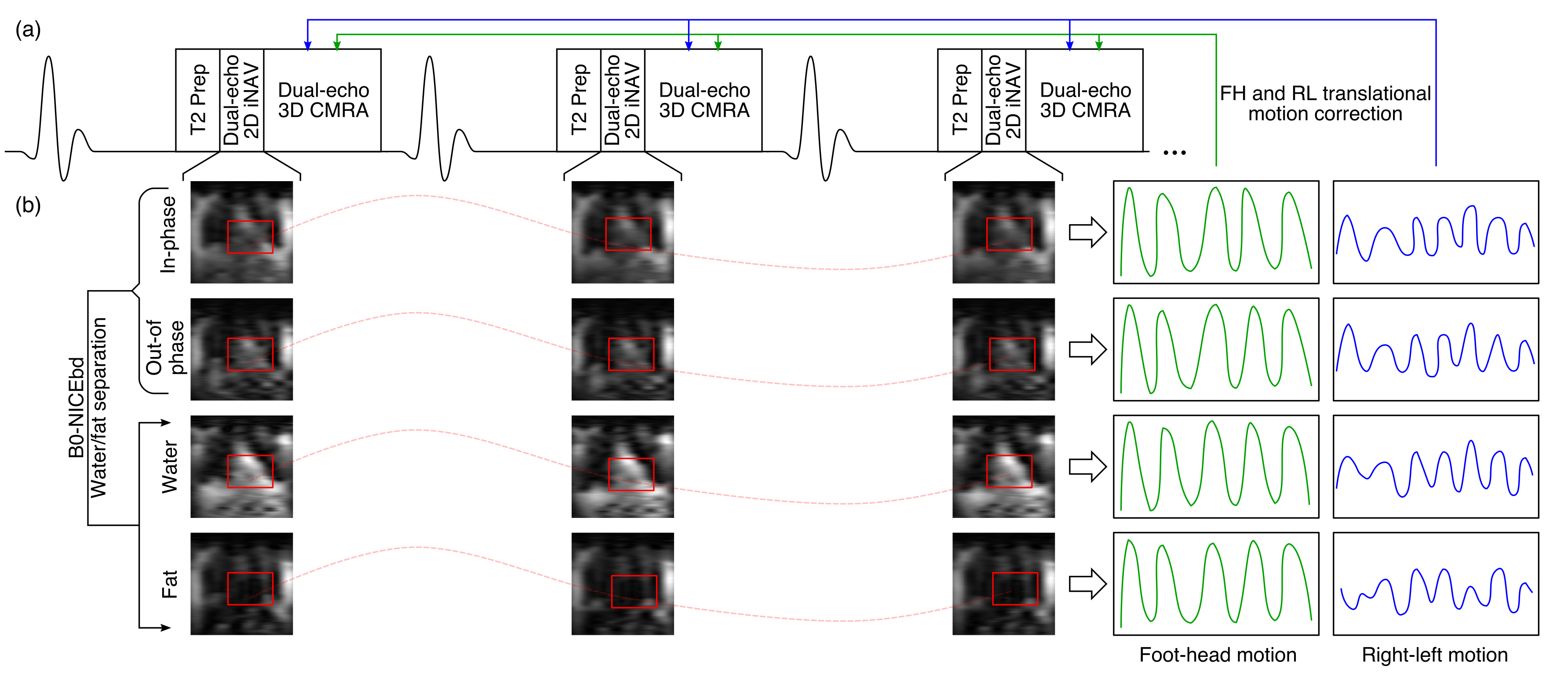
Acquisition consists of an ECG-triggered dual-echo 3D spoiled gradient echo sequence (Fig1a). 3D dual-echo CMRA data is acquired with a fully sampled golden-step Cartesian trajectory with spiral profile order sampling6, while 2D dual-echo iNAVs are acquired by spatially encoding low flip-angle lines before the 3D acquisition. Water and fat iNAVs were obtained from in-phase and out-of-phase iNAVs using the B0-NICEbd7 water/fat separation method, resulting in four iNAVs with varying contrasts. Foot-head (FH) and right-left (RL) motion was then estimated for each iNAV using the same tracking template (Fig1b). In order to study the performance of each iNAV for motion estimation, translationally motion-corrected (TC) 3D CMRA dual-echo images were obtained by applying a shift in k-space according to the FH and RL displacements estimated from each iNAV, and the B0-NICEbd method was used to obtain corresponding TC water/fat CMRA images. These water/fat CMRA images were reformatted to visualise the right (RCA) and left (LAD) coronary arteries, and visually assessed in terms of artefacts and appearance of the vessels. Furthermore, vessel sharpness was computed for both RCA and LAD in the water images.
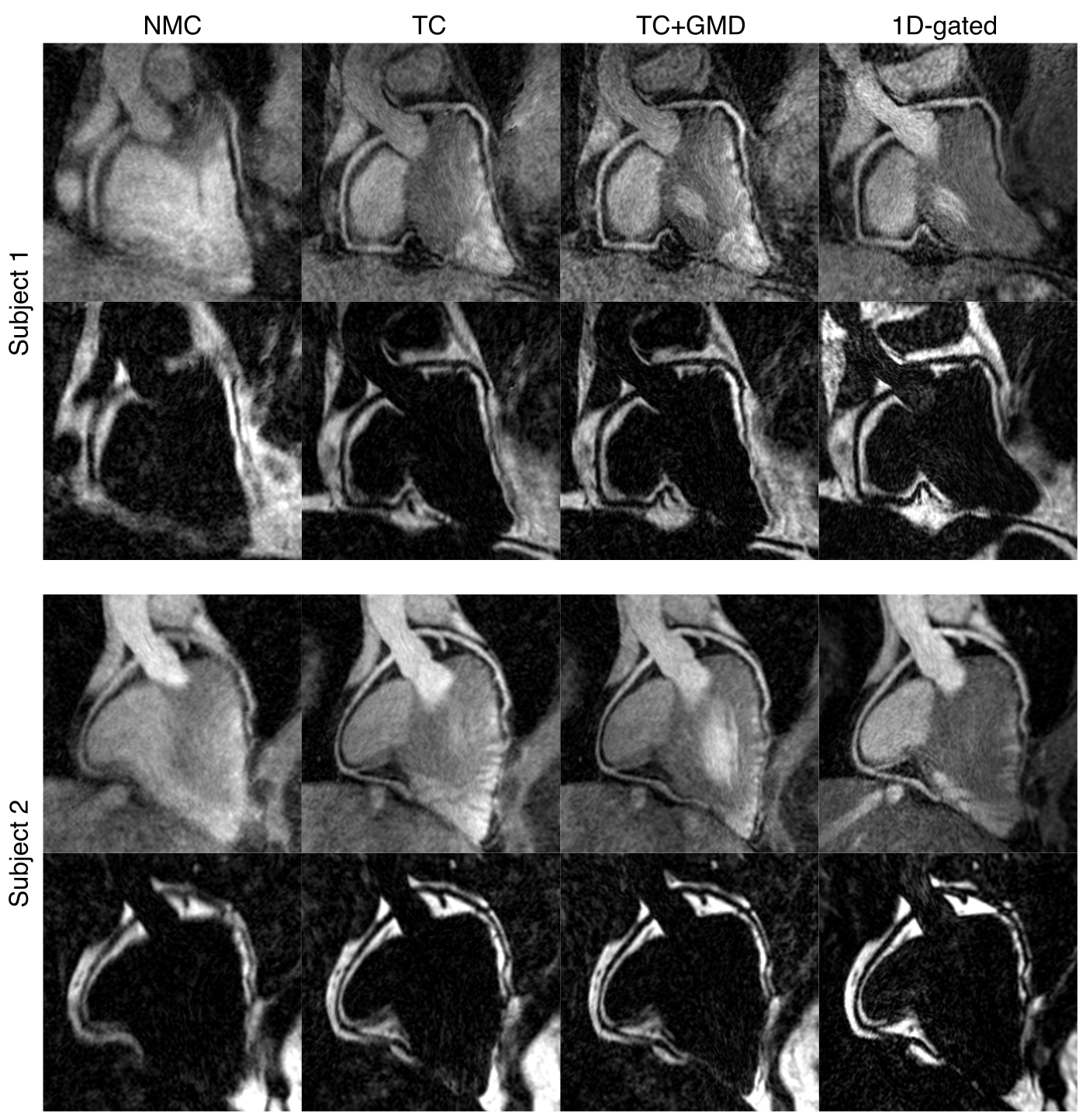
After identifying the iNAV that produced the best FH and RL motion estimates, translational plus non-rigid respiratory motion corrected (TC+GMD) water/fat CMRA images were reconstructed. Water/fat CMRA images without motion correction (NMC) were also obtained for comparison purposes.
Six healthy subjects were scanned on a 3T scanner (Biograph mMR, Siemens Healthcare, Erlangen, Germany) using a prototype implementation of the proposed dual-echo iNAV-based 3D CMRA sequence (coronal orientation, resolution=1.3mm isotropic, FOV=312×312×78-104mm, TR/TE1/TE2=5.26/2.46/3.69ms, FA=20°, T2prep=50ms). A subject-specific trigger delay and acquisition window (95-115ms) were set coinciding with the mid-diastolic rest period. Additionally, a Cartesian ECG-gated dual-echo 3D CMRA scan with a 1D diaphragmatic gating and tracking (1D-gated: 6 mm gating window, tracking factor of 0.6, 2x-accelerated using GRAPPA) and matching imaging parameters was performed for comparison purposes.
Results
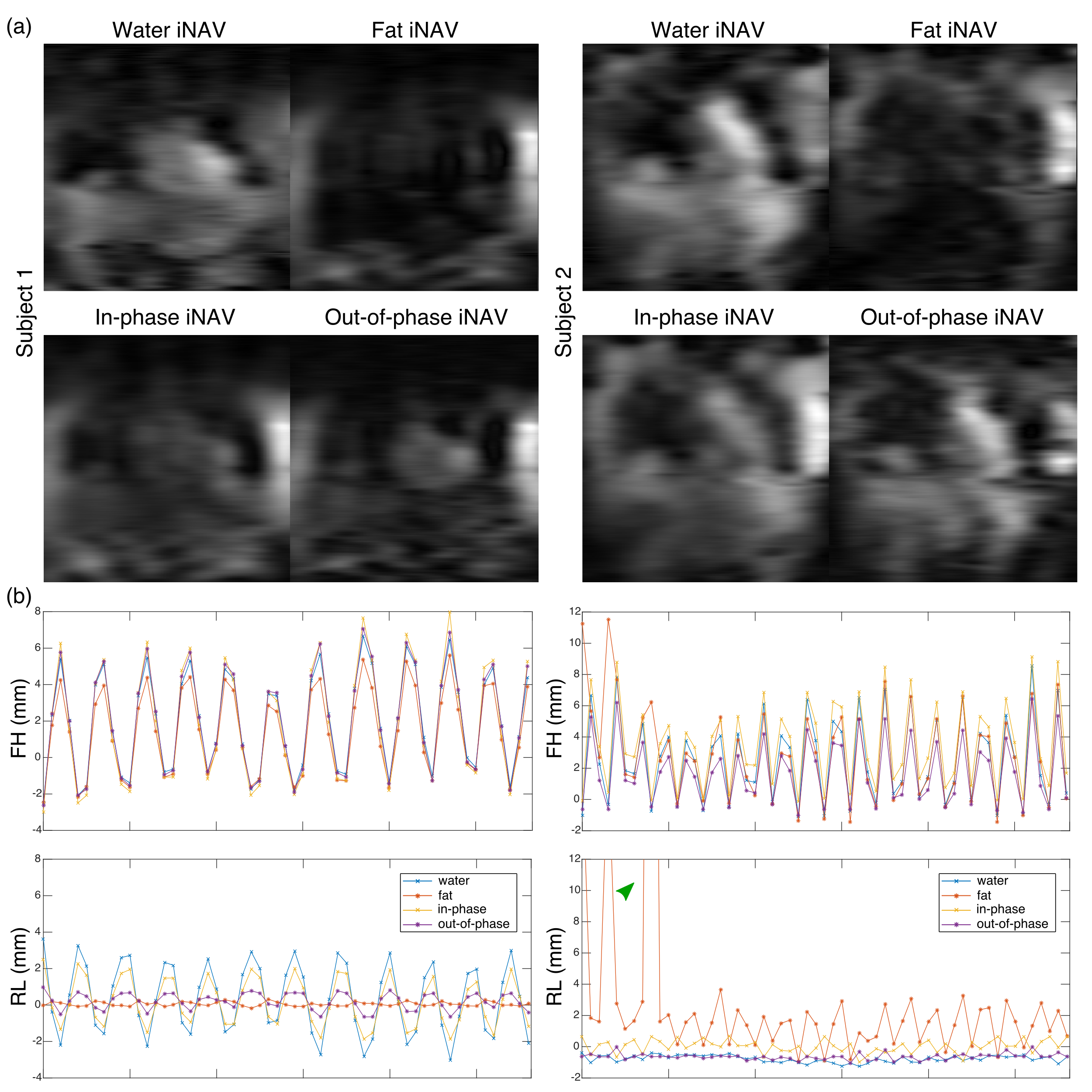
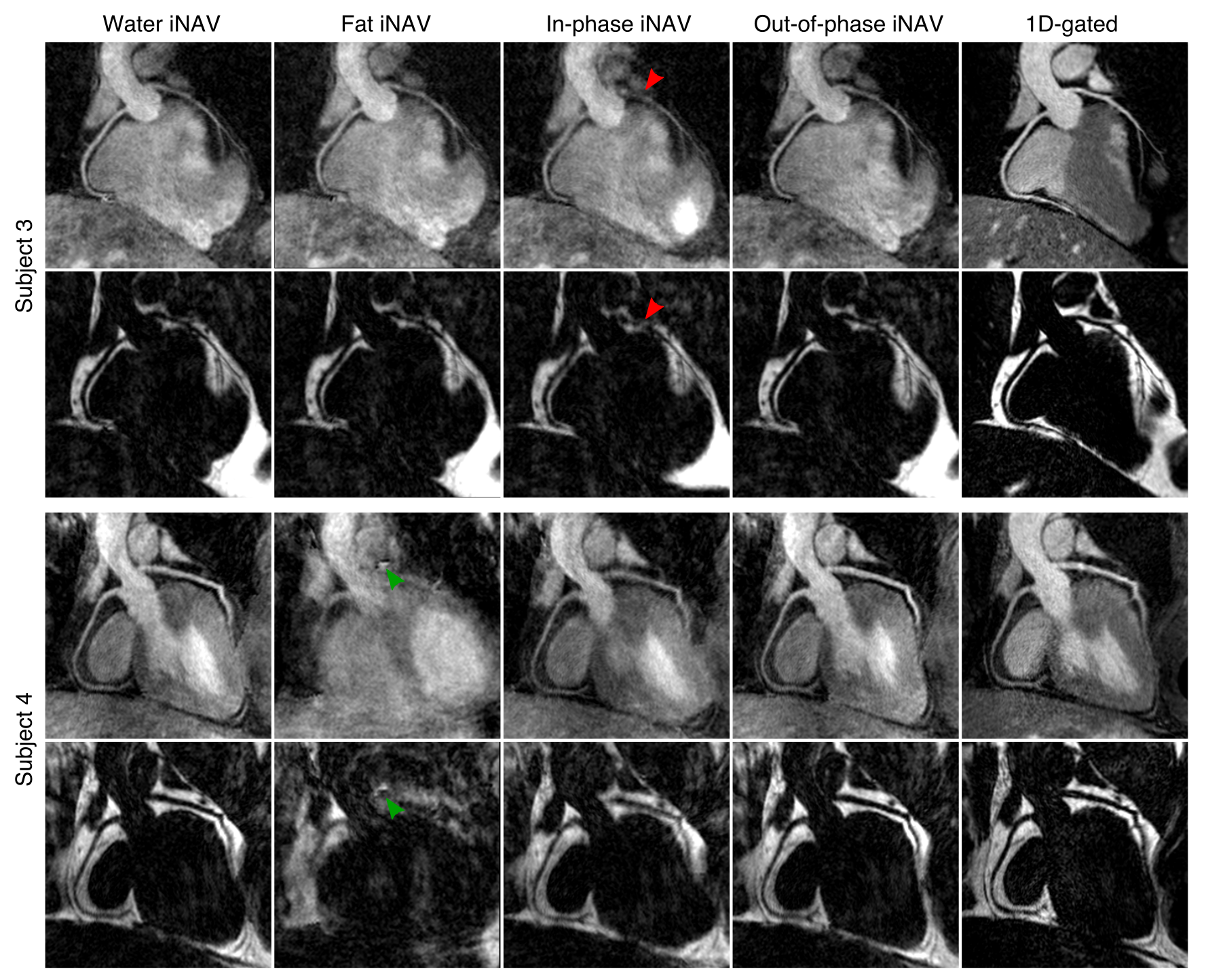
Fig2 shows example iNAVs and corresponding FH and RL motion estimates for two subjects. While estimation of FH motion is consistent across the different iNAVs in both cases, differences are apparent in RL motion estimation, impacting image quality in TC water/fat CMRA images. Average vessel sharpness for both coronaries in the water CMRA images when using water, fat, in-phase and out-of-phase iNAVs was 33.7±7.6%, 29.3±9.0%, 31.1±6.5% and 37.1±7.4%, respectively. The increased vessel sharpness with out-of-phase iNAVs is most likely related to the black-rim chemical-shift artefacts, that may facilitate motion tracking. Overall, out-of-phase iNAVs resulted in good image quality and vessel depiction (Fig3), and were therefore used for estimating translational respiratory motion for the remainder of the study. Compared to NMC water/fat images, improvements in vessel delineation are observed when applying TC (Fig4). Further improvements are obtained with the TC+GMD approach, which results in images comparable to the 1D-gated (Fig4). The motion correction approach results in good quality water/fat CMRA images (Fig5), from an efficient acquisition with predictable scan time.Conclusion
Here we present a framework for respiratory motion-corrected whole-heart water/fat CMRA. This approach is based on the use of dual-echo 2D iNAVs for 100% respiratory scan efficiency. From the four different iNAVs studied, out-of-phase iNAVs resulted in the most accurate motion estimates for all subjects, producing sharp water/fat CMRA images without visible artefacts due to local water/fat swaps. The translational plus non-rigid respiratory motion correction approach results in water/fat CMRA images comparable to conventional 1D-gated water/fat images, but in a shorter and predictable scan time.Acknowledgements
This work was supported by EPSRC (EP/L015226/1, EP/P001009, EP/P007619, EP/P032311/1) and Wellcome EPSRC Centre for Medical Engineering (NS/A000049/1).References
1. Nezafat M, Henningsson M, Ripley DP, et al. Coronary MR angiography at 3T: fat suppression versus water-fat separation. Magn Reson Mater Physics, Biol Med 2016;29:733–738.
2. Goeller M, Achenbach S, Cadet S, et al. Pericoronary Adipose Tissue Computed Tomography Attenuation and High-Risk Plaque Characteristics in Acute Coronary Syndrome Compared With Stable Coronary Artery Disease. JAMA Cardiol 2018;3:858.
3. Börnert P, Koken P, Nehrke K, et al. Water/fat-resolved whole-heart Dixon coronary MRA: An initial comparison. Magn Reson Med 2014;71:156–163.
4. Cruz G, Atkinson D, Henningsson M, et al. Highly efficient nonrigid motion-corrected 3D whole-heart coronary vessel wall imaging. Magn Reson Med 2017;77:1894–1908.
5. Munoz C, Neji R, Cruz G, et al. Motion-corrected simultaneous cardiac positron emission tomography and coronary MR angiography with high acquisition efficiency. Magn Reson Med 2017;79:339–350.
6. Prieto C, Doneva M, Usman M, et al. Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. J Magn Reson Imaging 2015;41:738–46.
7. Liu J, Peters DC, Drangova M. Method of B0 mapping with magnitude-based correction for bipolar two-point Dixon cardiac MRI. Magn Reson Med 2017;78:1862–1869.
Figures