0456
Dilated Pulmonary Arteries and Wall Shear Stress in Patients with Repaired Tetralogy of Fallot.Han-Jung Liao1, Jung-Hsiu Liu1, Ming-Ting Wu2, Ken-Pen Wang2,3, Mao-Yuan Su4, and Hsu-Hsia Peng1
1National Tsing Hua University, Hsinchu, Taiwan, 2Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, 3National Yang-Ming University, Taipei, Taiwan, 4National Taiwan University Hospital, Taipei, Taiwan
Synopsis
We aimed to investigate the impact of pulmonary area on wall shear stress (WSS) and oscillatory shear index (OSI) to explore the altered vascular characteristics in patients repaired tetralogy of Fallot (rTOF). rTOF patients with pulmonary dilatation presented decreased axial WSS and increased axial OSI. The correlations between pulmonary area and axial WSS and OSI were missing in rTOF patients, depicting the abnormal endothelial regulation function in response to axial WSS and OSI. In conclusion, the correlation analyses between pulmonary area, axial WSS and OSI might provide helpful information in investigating the altered vascular characteristics in patients with rTOF.
Introduction
Patients with repaired tetralogy of Fallot (rTOF) show impaired endothelial function in branchial artery and histological abnormalities in pulmonary trunk.1,2 Wall shear stress (WSS), describing a drag force of blood flow along the vessel wall, and oscillatory shear index (OSI) are well-known as regulating factors of the vascular remodeling.3 Previous studies reported that patients with aortic dilatation or different vascular structures could have impact on WSS, flow patterns, and the developments of aneurysm dissection or rupture.4-6 Currently, the relationship between pulmonary dilatation and the WSS of pulmonary arteries in patients with rTOF has not been discussed thoroughly. We aimed to investigate the impact of pulmonary area on WSS and OSI to explore the altered vascular characteristics in patients with rTOF.Method
This study recruited 20 rTOF patients (22±3 y/o, male/female: 12/8) and 22 age-matched normal controls (22±1 y/o, male/female: 14/8) without known cardiovascular diseases. Images were acquired at a 3.0-T MR scanner (Tim Trio or Skyra, Siemens, Erlangen, Germany). 4D flow was performed with TR/TE=10.8/2.9 ms, flip angle=7°, VENC=1.5 m/s, voxel size=1.2×1.2×3.5 mm3. Twelve 2D planes were determined in the main, right and left pulmonary arteries (MPA, RPA, LPA) for calculation of flow-related parameters (Figure 1). A threshold of pulmonary dilatation was set as mean+standard deviation of M8 area of the normal group. Patients with rTOF were divided into rTOF-1 (n=11) and rTOF-2 (n=9) to represent patients without and with pulmonary dilatation, respectively. The axial WSS and axial OSI is calculated as described by Frydrychowicz A., et al.7 Retrograde flow (RF) fraction is calculated as the percentage of RF divided by total flow during the whole cardiac cycle. Two-tailed Student t test and Pearson correlation were accessed when appropriate. A p<0.05 was considered statistically significant.Results
Table 1 summarizes the demographics of study population. In Figure 2, compared with normal group, rTOF-2 subgroup presented dilated MPA, decreased axial WSS in MPA and LPA, and increased axial OSI. The rTOF-1 subgroup presented increased axial OSI in MPA, RPA, and LPA. Figure 3a-c illustrates that normal group exhibited correlations between axial WSS and pulmonary area in MPA, RPA, and LPA (p≤0.001). The axial WSS was correlated with pulmonary RF in MPA and RPA (p = 0.001) only in rTOF-1 subgroup (Figure 3d-f).Figure 3g-i demonstrates correlations between OSI and pulmonary area in MPA, RPA, and LPA of normal group (p≤0.001). The axial OSI was also correlated with pulmonary RF in MPA of rTOF-1 subgroup (p<0.001) (Figure 3j-l).Discussion and Conclusion
In this study, we quantified the area, RF, axial WSS and OSI in the MPA, RPA, and LPA of rTOF patients. Previous studies demonstrated that he abnormal WSS and OSI were associated with vascular disease and atherosclerosis8,9 and endothelial cells could adapt to the altered blood flow-induced mechanical force by remodel the vascular diameter and wall thickness.10 The dilated area and decreased WSS were found to be associated with proximal pulmonary arterial remodeling in patients with pulmonary hypertension.11 In this study, the rTOF-2 subgroup exhibited increased area, decreased axial WSS, and increased OSI in the MPA, illustrating the dilated area could lead to lower WSS and consequently alter the vascular characteristics in the MPA. We also found there is no correlation between pulmonary area and axial WSS in rTOF-2, describing that different degrees of dilation have similar impact on axial WSS.The significant correlations between pulmonary area and axial WSS and OSI in the normal group might depict the normal endothelial regulation of pulmonary diameter in response to axial WSS and OSI. As for the two rTOF subgroups, the low correlation of pulmonary area with axial WSS and axial OSI might indicate that they are independent factors affecting the remodeling of pulmonary arteries.
The pulmonary RF demonstrated correlations only with axial WSS in the MPA and RPA and with axial OSI in the MPA of rTOF-1 subgroup, indicating a possible negative impact of RF on the vascular characteristics. In rTOF-2 group, a confounding factor of pulmonary dilatation might lead to the absence of correlation between pulmonary RF and axial WSS and OSI.
In conclusion, the correlation analyses between pulmonary area, RF, axial WSS and OSI might provide helpful information in investigating the altered vascular characteristics in patients with rTOF.
Acknowledgements
No acknowledgement found.References
1. Bedard, E., et al., Structural abnormalities of the pulmonary trunk in tetralogy of Fallot and potential clinical implications: a morphological study. J Am Coll Cardiol, 2009. 54.2. de Groot, P.C., et al., Vascular function in children with repaired tetralogy of Fallot. Am J Cardiol, 2010. 106(6): p. 851-5.
3. Chatzizisis, Y.S., et al., Role of endothelial shear stress in the natural history of coronary atherosclerosis and vascular remodeling: molecular, cellular, and vascular behavior. J Am Coll Cardiol, 2007. 49(25): p. 2379-93.
4. Bieging, E.T., et al., In vivo three-dimensional MR wall shear stress estimation in ascending aortic dilatation. J Magn Reson Imaging, 2011. 33.
5. Davies, R.R., et al., Yearly rupture or dissection rates for thoracic aortic aneurysms: simple prediction based on size. The Annals of Thoracic Surgery, 2002. 73(1): p. 17-28.
6. Chern, M.J., M.T. Wu, and S.W. Her, Numerical study for blood flow in pulmonary arteries after repair of tetralogy of Fallot. Comput Math Methods Med, 2012. 2012: p. 198108.
7. Frydrychowicz, A., et al., Three-dimensional analysis of segmental wall shear stress in the aorta by flow-sensitive four-dimensional-MRI. Journal of Magnetic Resonance Imaging, 2009. 30(1): p. 77-84. 8. Malek, A.M., S.L. Alper, and S. Izumo, Hemodynamic shear stress and its role in atherosclerosis. JAMA, 1999. 282(21): p. 2035-2042.
9. Cecchi, E., et al., Role of hemodynamic shear stress in cardiovascular disease. Atherosclerosis, 2011. 214(2): p. 249-256.
10. Alberts B, J.A., Lewis J, et al., Molecular Biology of the Cell. . 2002. 4th edition.(Blood Vessels and Endothelial Cells.).
11. Schafer, M., et al., Main pulmonary arterial wall shear stress correlates with invasive hemodynamics and stiffness in pulmonary hypertension. Pulm Circ, 2016. 6(1): p. 37-45.
Figures
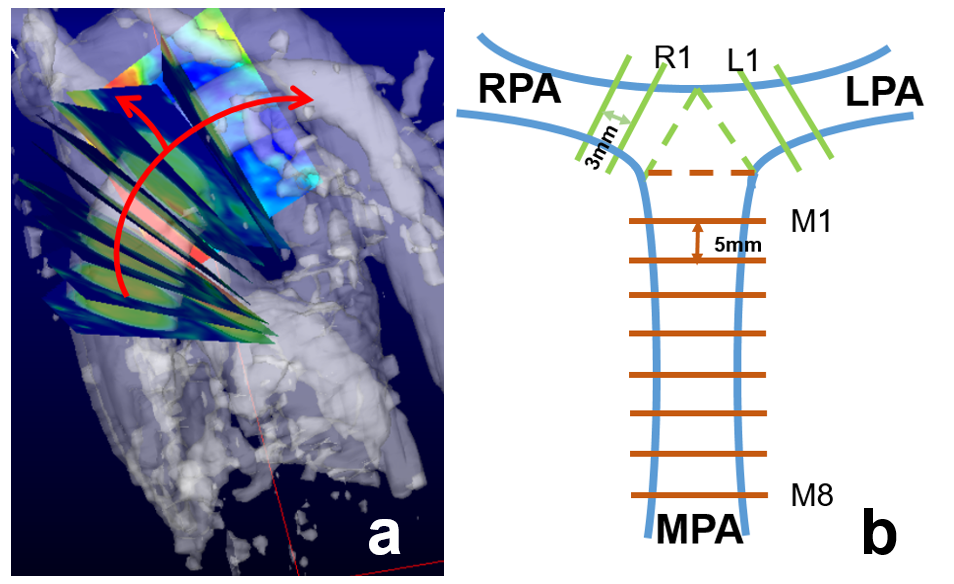
Figure
1. (a,b) The
illustrations of the determined 12 planes determined
in the main, right and left
pulmonary arteries (MPA, RPA, LPA) for calculation of flow-related parameters
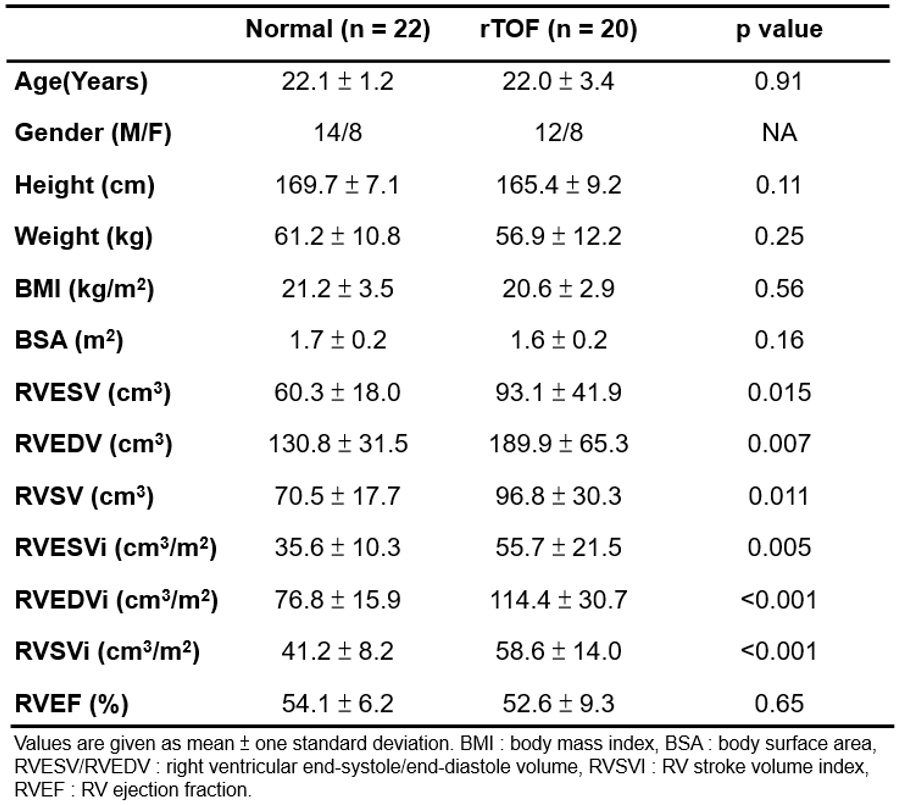
Table 1. Demographic characteristics of the study population.
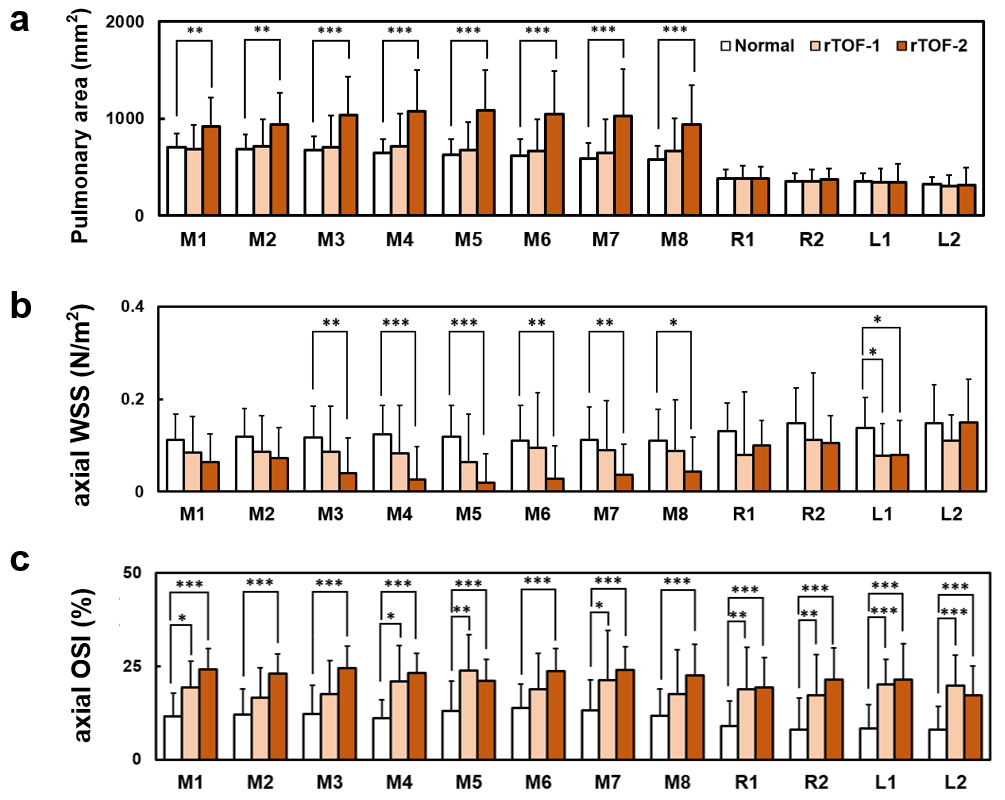
Figure
2. The
pulmonary area (a),
axial wall shear stress (b), and
axial oscillatory shear index (c) in
patients without (rTOF-1) and with (rTOF-2) dilated pulmonary area in main
pulmonary artery.
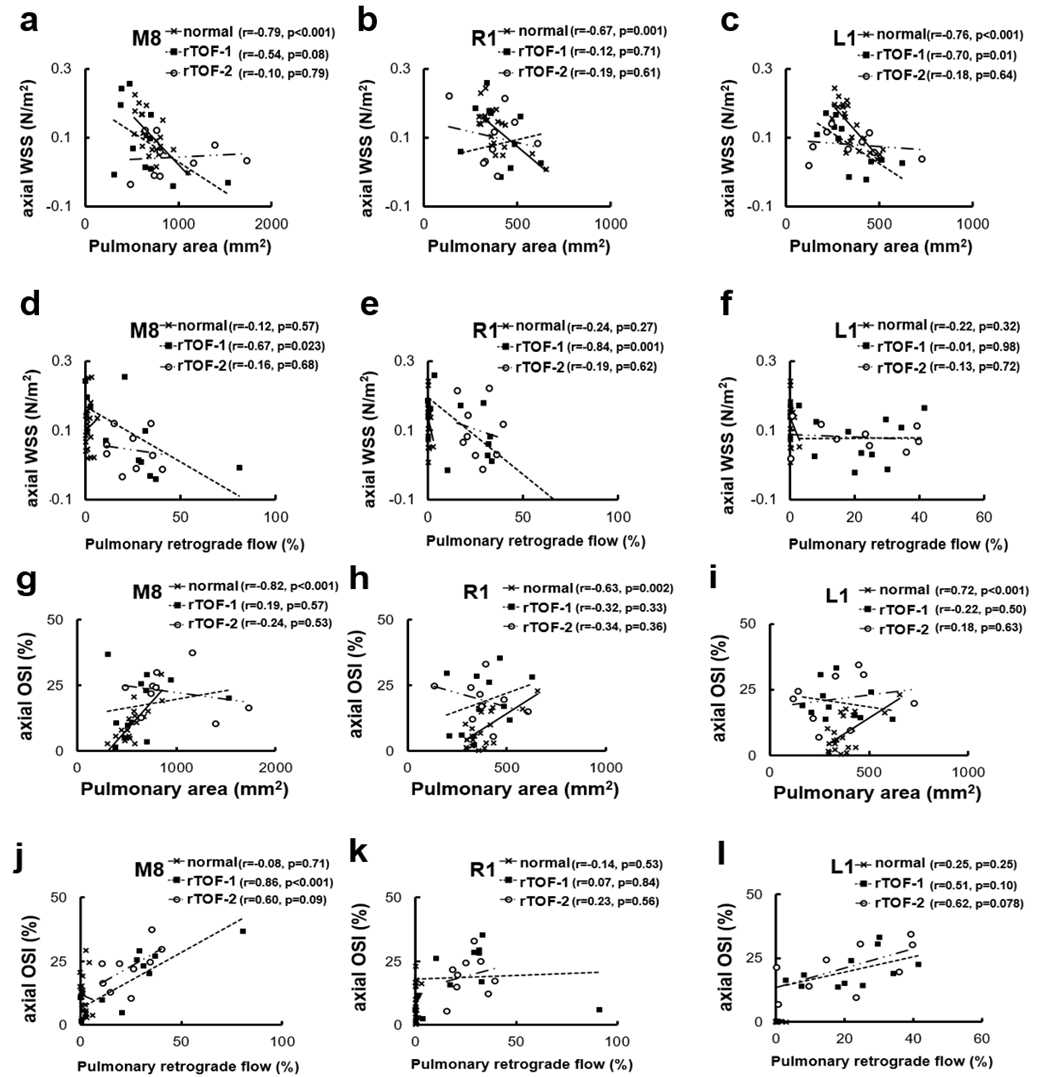
Figure
3. (a-c) The
correlation between axial WSS and
pulmonary area (d-f), between axial WSS and pulmonary retrograde flow (g-i), between axial OSI and pulmonary area (j-l)
and
between axial OSI and pulmonary retrograde flow in the M8, R1, and L1 planes of
normal, rTOF-1, and rTOF-2 groups.