0451
Enhanced non-invasive pressure drop and flow inefficiencies quantification via 4D-flow MRI1School of Biomedical Engineering & Imaging Sciences, Kings College London, London, United Kingdom, 2Division of Cardiovascular Medicine, Radcliffe Department of Medicine, Oxford, United Kingdom
Synopsis
The pressure drop caused by convective effects is the standard clinic method for diagnosis of aortic stenosis using simplified Bernoulli. However simplified Bernoulli results in a reported overestimation that can be resolved with 4D-flow MRI and Simplified Advective Work-energy relative pressure (SAW). This work further refines SAW formulation and proposes an enhanced analysis of the positive and negative components of flow profile. Whereas forward SAW pressure drop correlates better with mean SB (R2=0.951) than full velocity profile by SAW (R2=0.901), backward SAW is totally independent of SB (R2=0.490), which makes the flow efficiency a potential predictive value for disease progression.
Introduction
Aortic valve stenosis (AS) is the most common valvular heart disease, affecting 3% of the world population and the likelihood of increasing with population ageing.1 AS consists of a diminished open valve orifice area resulting in an increased trans-valvular pressure drop (ΔP). In order to access and monitor the valve condition, simplified Bernoulli (SB) by Doppler echocardiography is the standard imaging technique capturing only the peak flow velocity at the effective orifice area plane (EOA).2 As an alternative, Four-dimensional phase-contrast MRI (4D-flow MRI) provides time-resolved blood flow velocities in 3D, and improves the accuracy and precision of ΔP based on the full velocity profile at the EOA.3 However, current 4D-flow MRI method does not account for the presence of backward flow. We thus hypnotised that a ΔP capturing only the forward flow should be more specific to the stenosis and that the ΔP capturing only the backward flow is a surrogate of inefficiencies.Methods
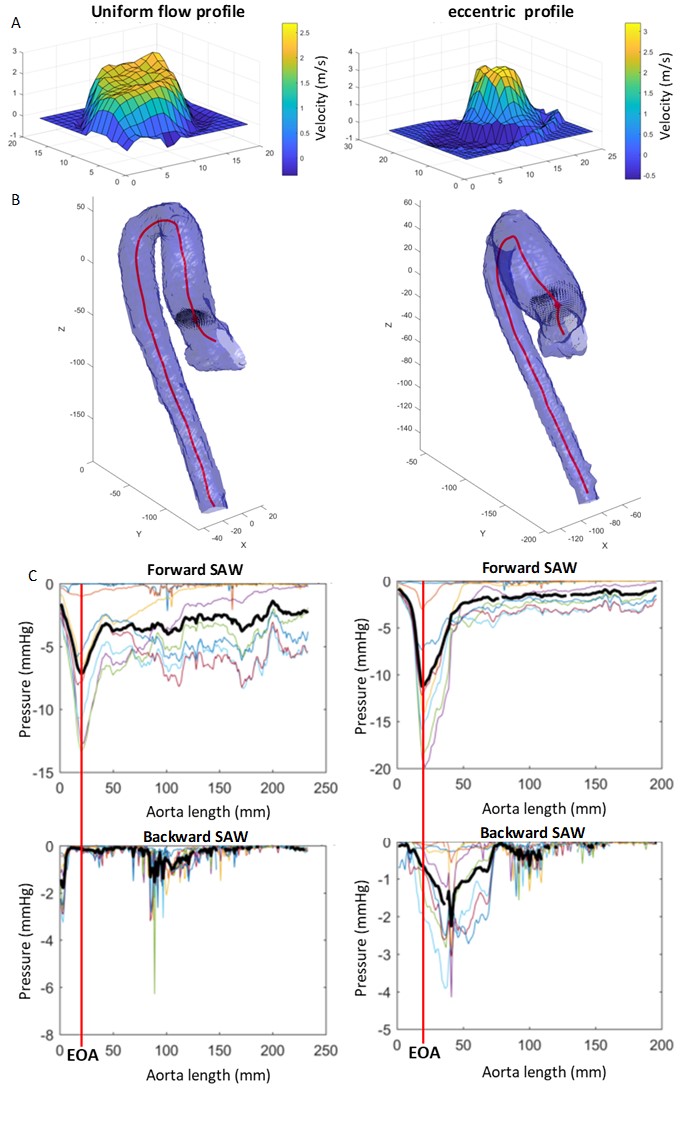
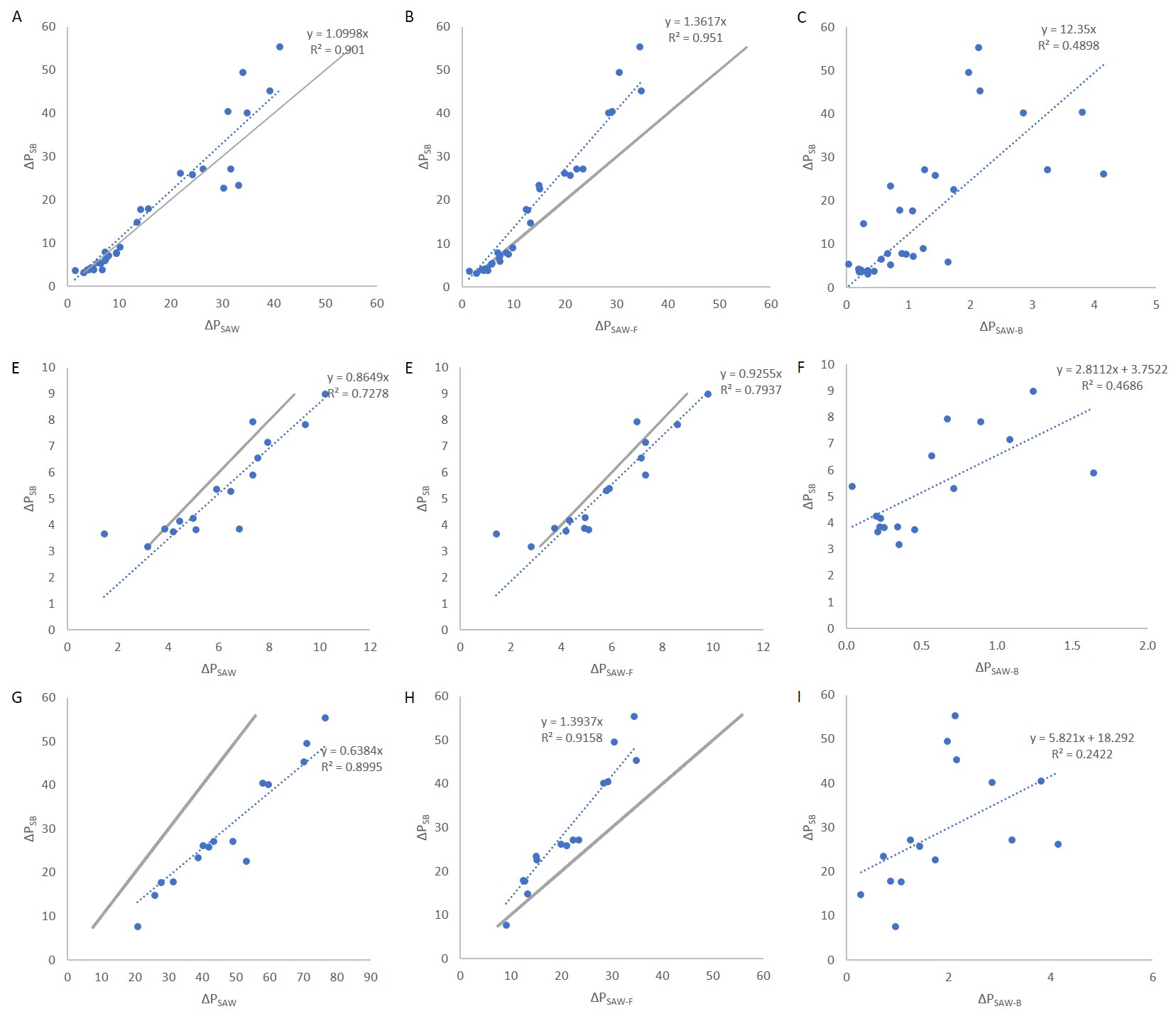
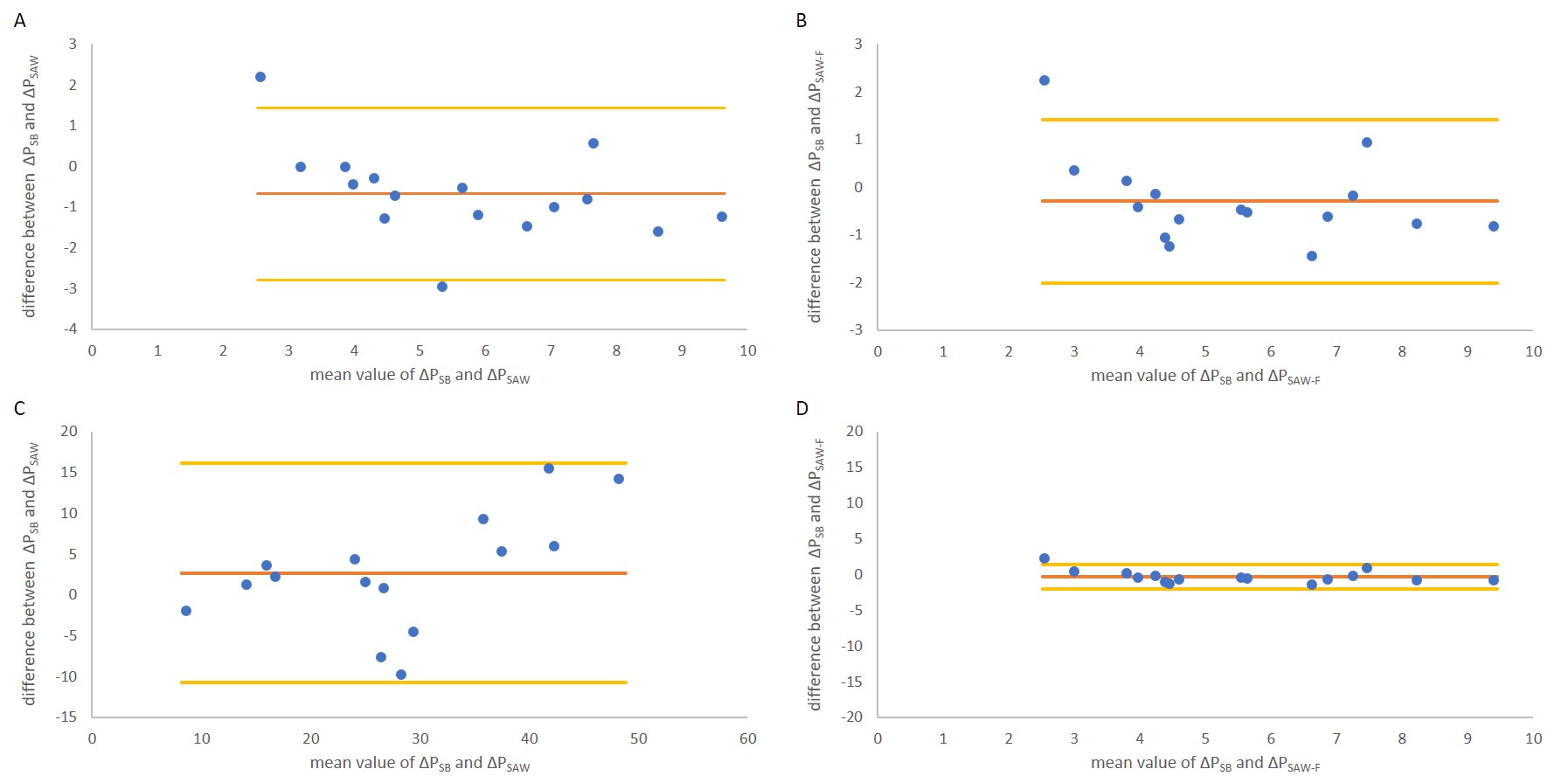
4D-flow MRI velocity vector fields of 31 bicuspid aortic valve patients were processed to compute the ΔP with the Simplified Advective Work-energy relative pressure formulation (SAW): ∆PSAW=-1/Q (Ae), where Q is flow rate and Ae is the advective energy rate.3 Semi-automatic segmentation with manual adjustments was performed based on the average systolic frames of 4D-flow MRI. Along the segmentation centreline, cross-planes were generated every 2cm, and SAW was computed in each based on the complete, the forward or the backward flow profiles (ΔPSAW, ΔPSAW-F and ΔPSAW-B respectively). From these planes, the EOA is automatically identified as the point of maximum full SAW. Maximum velocity at the EOA was used to compute the SB pressure drop (ΔPSB). Mean values along the systolic events are then computed for each of these 4 estimations. Furthermore, we subdivide the patient cohort into clinical relevant (ΔPSB >20mmHg) and non-relevant pressure drop (ΔPSB <20mmHg) as stated in the guidelines.4 Linear regression and Bland-Altman plots between each methodological alternative and are investigated (Figure 1). Results
ΔPSAW-F Forward flow SAW has better agreement with ΔPSB than the original ΔPSAW (correlation presented R2 of 0.951 and 0.901 respectively) also in the clinical (Figure 1). Subdividing the analysis into the two subgroups according to the clinical guidelines we obtained the results shown in (Figures 2 and 3). Whereas ΔPSAW-B. does not show any agreement with ΔPSB in any of the three metrics presented.Discussion
The peak pressure drop (by any formulation, SB or SAW) captures the physics of the spatial acceleration of the blood from the nearly static status in the ventricle to the blood jet at the EOA. SAW is a correction of SB, accounting for the shape of the velocity profile.3 In this work we have refined the definition of SAW, removing the confounding factor of the presence of backward flow at the plane located at the EOA. The removal of this factor increases the agreement of SAW and SB.
The presence of backward flow can be considered a metric of inefficiency since it reflects the creation of blood momentum in the opposite direction. The assumption is that the magnitude of retrograde flow is a good surrogate of the actual viscous losses of the flow (that are generated by viscous or turbulent effects). The preliminary data presented here illustrates that the ΔPSAW-B is independent of the peak pressure drop, and as such could provide additional diagnostic information as MRI enabled estimation of turbulent dissipation.5
The ΔP caused by convective effects is the standard clinic method for diagnosis of aortic stenosis using SB. However, SB results reported overestimation that can be resolved with 4D-flow MRI and SAW. This work further refines SAW formulation and proposes an enhanced analysis of the positive and negative components of the flow profile.
Acknowledgements
This project has received funding from the European Union’s Horizon 2020 Research and innovation programme under the Marie Sklodowska-Curie Grant Agreement: No 764738References
1. Thaden JJ, Nkomo VT, Enriquez-Sarano M. The global burden of aortic stenosis. Prog Cardiovasc Dis 2014;56:565-71.
2. Otto CM. Valvular
aortic stenosis: disease severity and timing of intervention. J Am Coll Cardiol
2006;47:2141-51.
3. Donati F, Myerson
S, Bissell MM et al. Beyond Bernoulli: Improving the Accuracy and Precision of
Noninvasive Estimation of Peak Pressure Drops. Circ Cardiovasc Imaging 2017;10.
4. Vahanian A,
Baumgartner H, Bax J et al. Guidelines on the management of valvular heart
disease: The Task Force on the Management of Valvular Heart Disease of the
European Society of Cardiology. Eur Heart J 2007;28:230-68.
5. Ha H, Lantz J,
Ziegler M et al. Estimating the irreversible pressure drop across a stenosis by
quantifying turbulence production using 4D Flow MRI. Sci Rep 2017;7:46618.
Figures