0450
Longitudinal Study of Aortic Stiffness and Flow Reversal in Patients with Cryptogenic Stroke1Radiology, Northwestern University, Chicago, IL, United States, 2Neurology, Northwestern University, Chicago, IL, United States, 3Radiology, Mayo Clinic, Rochester, MN, United States
Synopsis
Atherosclerotic plaque in the descending aorta has emerged as a potential etiology of embolic stroke due to diastolic flow reversal in this region. This study seeks to investigate 1) whether aortic stiffness assessed by pulse wave velocity (PWV) may be related to flow reversal and 2) the effects of medical therapy on PWV and flow reversal. Twenty cryptogenic stroke patients were included in this 4D flow MRI study. We found relationships between age, PWV and flow reversal. No systematic change in PWV or flow reversal was detected for patients taking medications with potential de-stiffening effects.
Introduction
Despite extensive evaluation, the underlying cause of stroke remains undetermined (i.e. cryptogenic) in 20-30% of patients leading to a high risk for recurrent stroke1, 2. Recently, a new source of stroke has been identified involving aortic plaques and flow reversal in the descending aorta (DAo), i.e. reverse flow carries ruptured DAo plaques back (upward) toward the aortic branches and brain causing embolism. Evidence suggests stiffening of the aortic vessel wall, which occurs with age and atherosclerosis, leads to aortic flow reversal3. However, the relationship between age, aortic stiffness and reverse flow is not fully understood. Furthermore, while some cardiovascular medical therapies have been shown to reduce arterial stiffness (e.g. angiotensin converting enzyme (ACE) inhibitors),4 their impact on aortic stiffness (and thus potential of approved drugs to treat patients with reverse flow and reduce stroke risk) remains unknown. 4D flow MRI (3D time-resolved 3-directional velocity encoding) offers assessment of both aortic stiffness (i.e. by pulse wave velocity, PWV5, 6) and reverse flow7, 8 along the entire aorta based on a single scan. We have developed a comprehensive assessment of global aortic stiffness and regional reverse flow and applied these methods in a cohort of cryptogenic stroke patients. The goal was to 1) investigate relationships between age, PWV and reverse flow in a large cohort of patients and controls and 2) assess impact of medical therapy on PWV and flow reversal in subset of patients.Methods
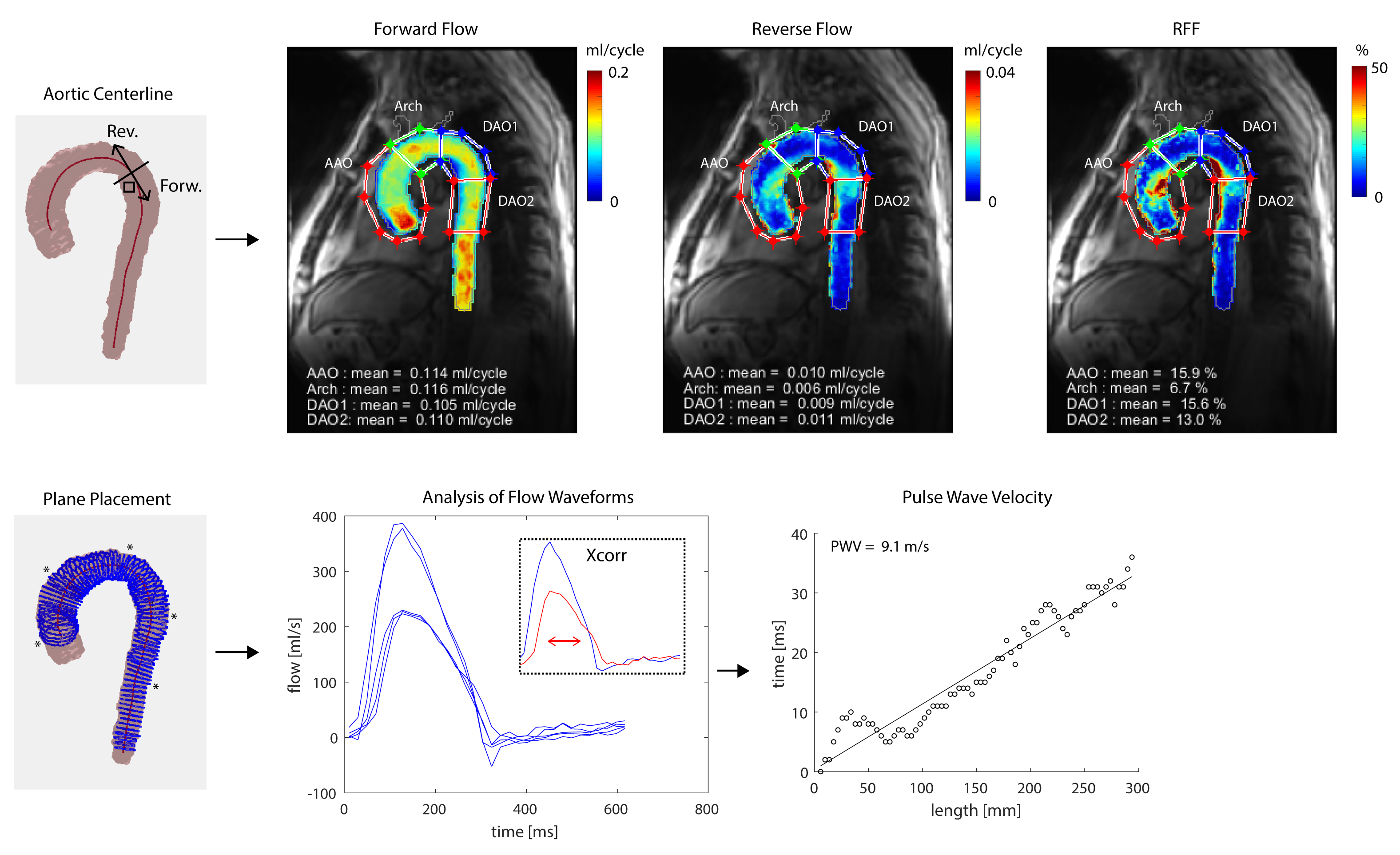
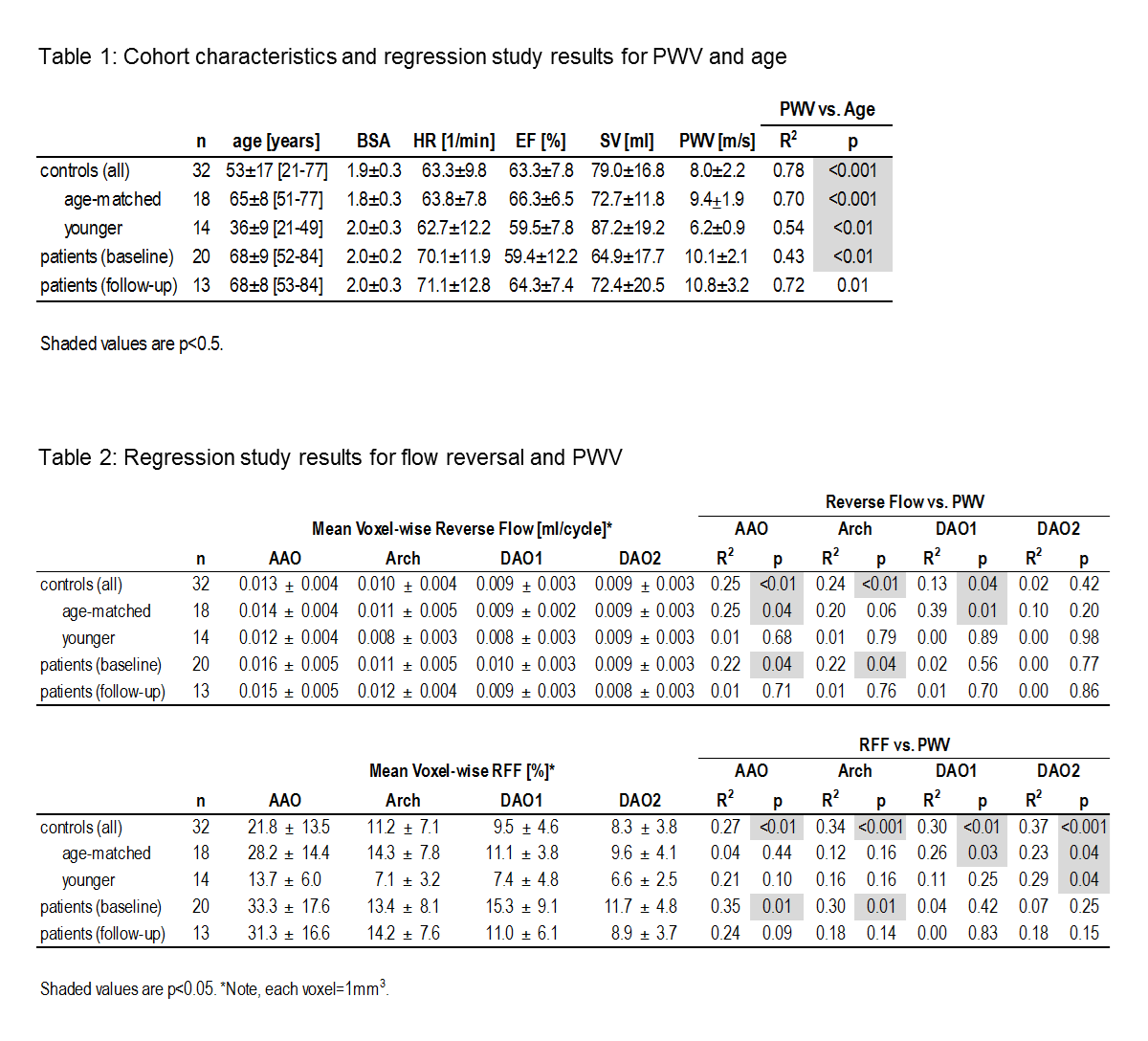
Non-contrast free-breathing 4D flow MRI (spatial resolution=3-3.5 x 2.3-2.6 x 2.6-3 mm3, temporal resolution=19.6 ms, venc=150 cm/s, k-t GRAPPA acceleration R=5, 1.5T MAGNETOM Aera: Siemens Healthcare, Erlangen, Germany) was performed in 20 cryptogenic stroke patients with DAo plaques, 18 age-matched controls and 14 younger controls (Table 1). 13 patients had a follow-up scan at 6±1 [5-8] months. They were treated with one or a combination of medical therapies with potential de-stiffening effects, i.e. ACE inhibitors, angiotensin receptor blockers (ARBs), calcium-channel blockers, beta blockers, statins and acetylsalicylic acid. Cardiac function was assessed using standard cine-MRI. Patients were evaluated for aortic valve regurgitation by Doppler echo. A 3D phase contrast MR angiogram was generated from 4D flow MRI and aortic volume segmented to mask velocities. For global aortic PWV quantification (Figure 1: bottom row), flow waveforms were generated at locations along the aorta and PWV was estimated using the cross-correlation (Xcorr)5, 6, 9 approach. 4D velocity data was regridded to 1 mm3 voxels. For reverse flow analysis (Figure 1: top row), parametric flow maps were generated similar to previously reported data analysis strategies10. Voxel-wise reverse and forward flow were summed over the cardiac cycle and reverse flow fraction ($$$RFF=\frac{Reverse Flow}{Forward Flow}\times100$$$%) calculated. To reduce noise, the lowest 1% of forward flow data was not included in RFF calculation. A 3D median 3-by-3-by-3 filter was applied. Mean intensity projection maps of forward flow, reverse flow, and RFF were generated. Four ROIs were identified (AAo, aortic arch Arch, DAo1, DAo2) and mean forward flow, reverse flow and RFF quantified.Results
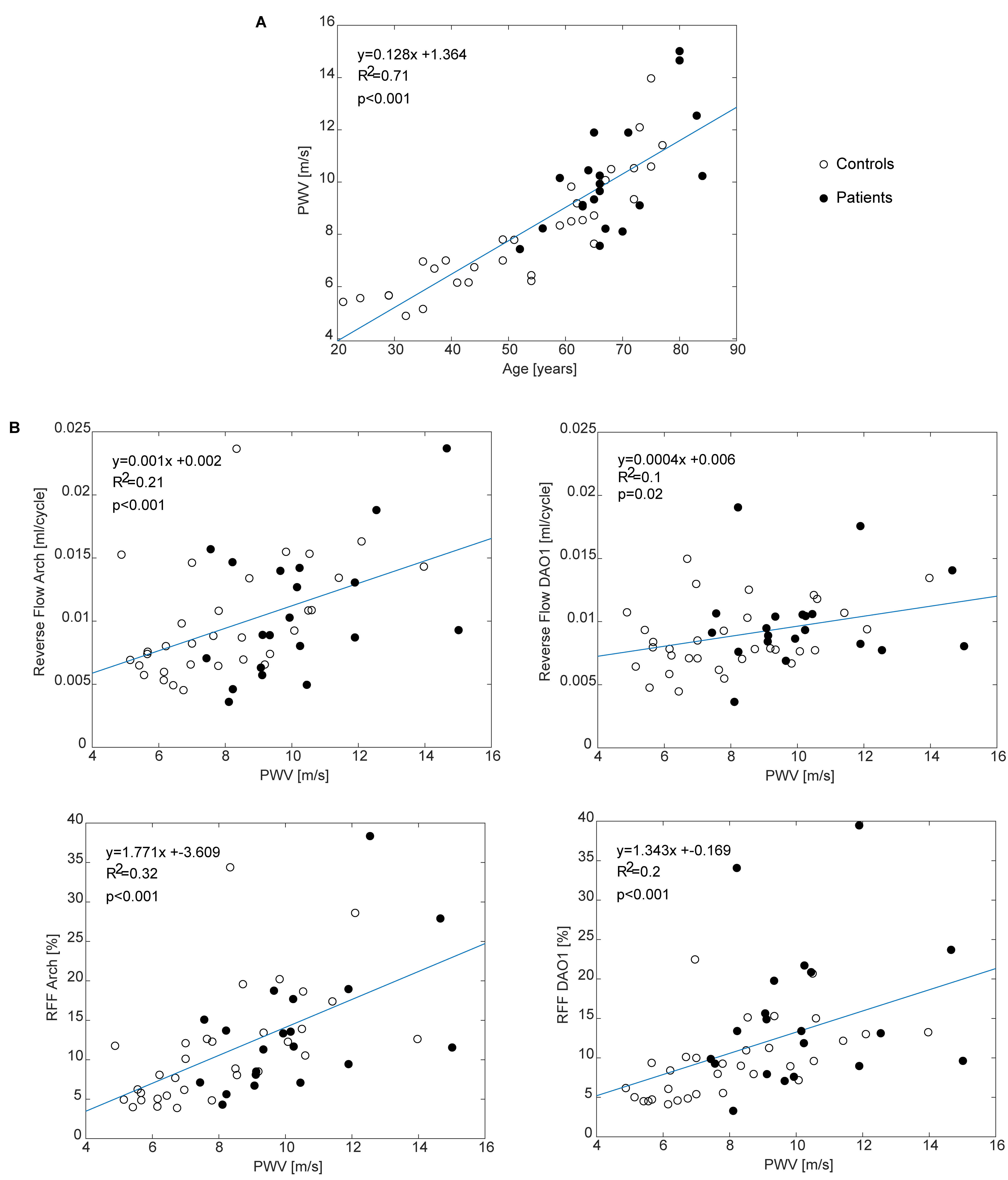
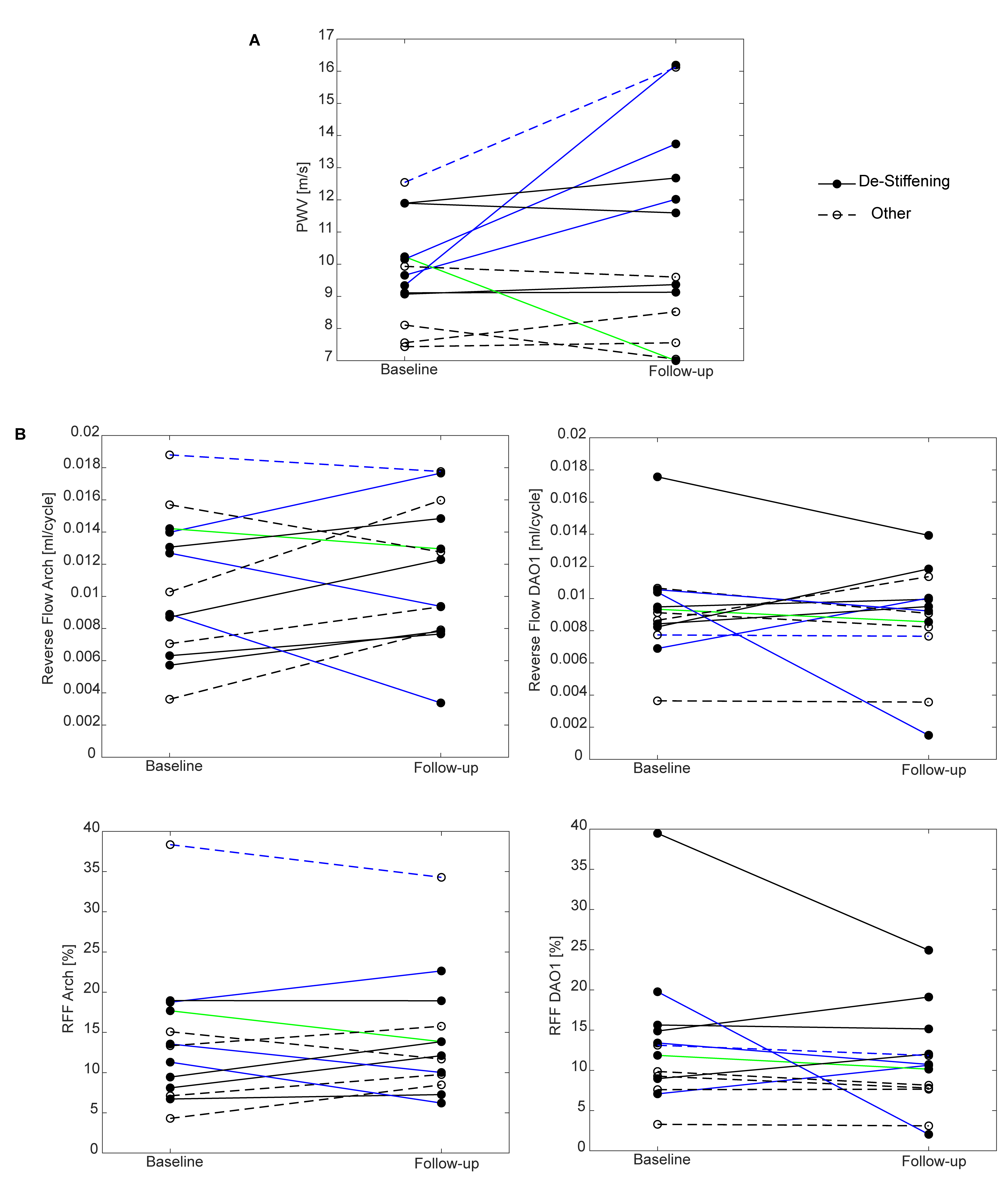
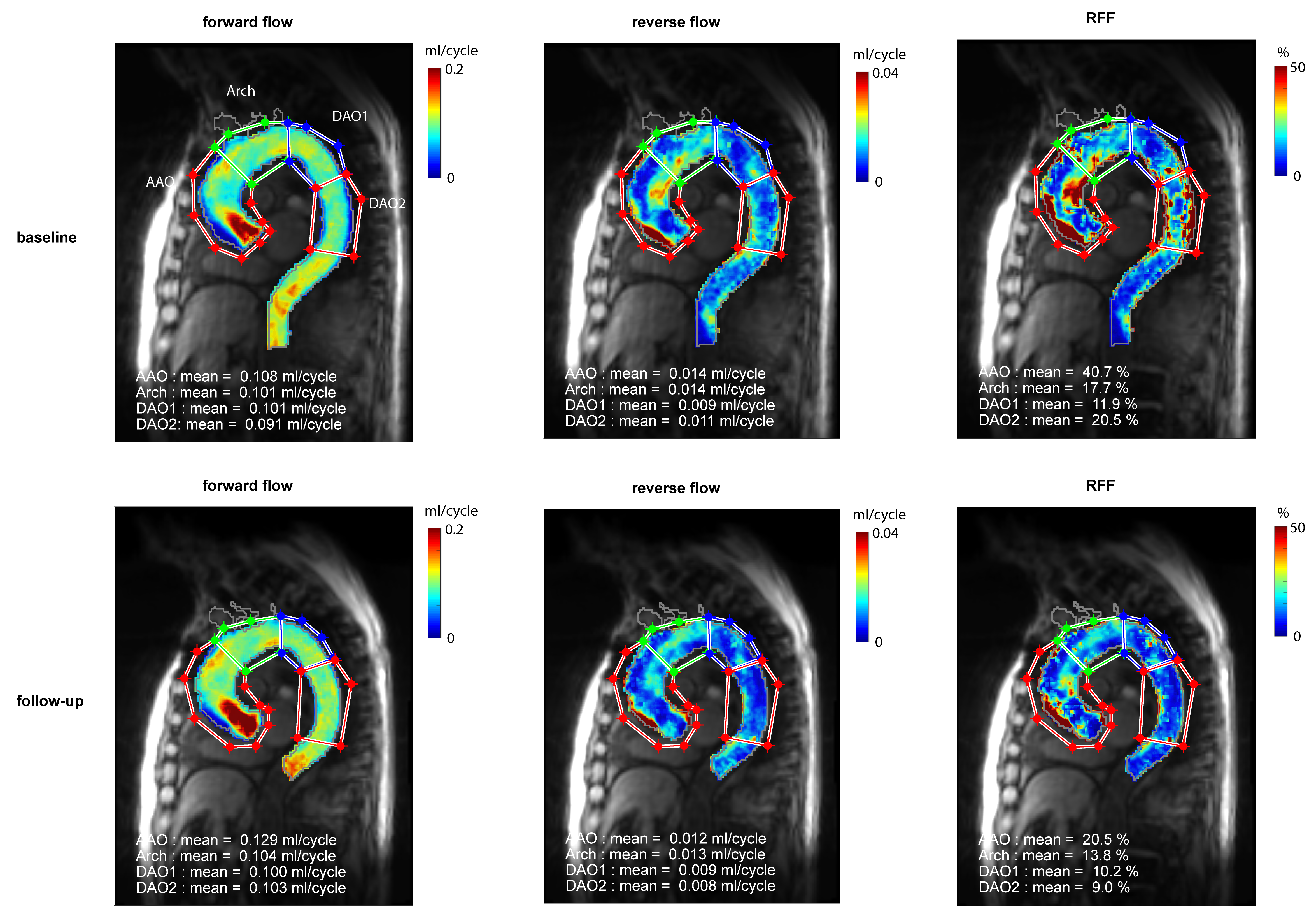
Trivial-mild aortic valve regurgitation was reported in 5 patients. For all subjects (n=52), age was significantly associated with PWV (R2= 0.71, p<0.001). PWV was significantly associated with reverse flow (AAO: R2=0.29, p<0.001, Arch: R2=0.21, p<0.001, DAO1: R2=0.10, p=0.02) and RFF (AAO: R2=0.38, p<0.001, Arch: R2=0.32, p<0.001, DAO1: R2=0.20, p<0.001, DAO2: R2=0.29, p<0.001) (Figure 2). See results by cohort (Table 2). For patients at follow-up compared to baseline (n=13), there was not a significant change in PWV, reverse flow or RFF (Figure 3). Also for the subset of patients (n=8) on medical therapy with well-known de-stiffening effects (i.e. ACE inhibitors, ARBs, calcium-channel blockers), there was not a significant change in PWV, reverse flow or RFF. Overall, four patients had clear worsening (>2m/s) in PWV with mixed changes in flow reversal. One patient had clear improvement (<2m/s) in PWV with slight favorable reductions in flow reversal (Figure 4).Conclusions
This 4D flow MRI study shows the utility of the developed methods for analyzing aortic stiffness (i.e. by PWV) and flow reversal in a large cohort of cryptogenic stroke patients and controls. As expected, PWV increases with age. More importantly, the relationship between PWV and flow reversal appears significant. We suspect aortic stiffness to play a role in the embolic mechanism of flow reversal. Medical treatment with potential de-stiffening effects did not have a systematic effect on PWV or flow reversal for patients in this study, however. Future work will focus on applying this technique in a larger cohort to parse out changes in aortic stiffness, flow reversal and effects of medication over time.Acknowledgements
Grant support by NIH, NHLBI T32 HL134633 and R21 HL132357References
1. Guercini F, Acciarresi M, Agnelli G, Paciaroni M. Cryptogenic stroke: time to determine etiology. J Thromb Haemost 2008;6(4):549-54.
2. Bang OY, Lee PH, Joo SY, Lee JS, Joo IS, Huh K. Frequency and mechanisms of stroke recurrence after cryptogenic stroke. Ann Neurol 2003;54(2):227-34.
3. Hashimoto J, Ito S. Aortic stiffness determines diastolic blood flow reversal in the descending thoracic aorta: potential implication for retrograde embolic stroke in hypertension. Hypertension 2013;62(3):542-9.
4. Janić M, Lunder M, Sabovič M. Arterial stiffness and cardiovascular therapy. Biomed Res Int 2014;2014:621437.
5. Markl M, Wallis W, Brendecke S, Simon J, Frydrychowicz A, Harloff A. Estimation of global aortic pulse wave velocity by flow-sensitive 4D MRI. Magn Reson Med 2010;63(6):1575-82.
6. Wentland AL, Wieben O, Francois CJ, Boncyk C, Munoz Del Rio A, Johnson KM, Grist TM, Frydrychowicz A. Aortic pulse wave velocity measurements with undersampled 4D flow-sensitive MRI: comparison with 2D and algorithm determination. J Magn Reson Imaging 2013;37(4):853-9.
7. Markl M, Semaan E, Stromberg L, Carr J, Prabhakaran S, Collins J. Importance of variants in cerebrovascular anatomy for potential retrograde embolization in cryptogenic stroke. Eur Radiol 2017.
8. Wehrum T, Dragonu I, Strecker C, Schuchardt F, Hennemuth A, Drexl J, Reinhard T, Bohringer D, Vach W, Hennig J, Harloff A. Aortic atheroma as a source of stroke - assessment of embolization risk using 3D CMR in stroke patients and controls. J Cardiovasc Magn Reson 2017;19(1):67.
9. Fielden SW, Fornwalt BK, Jerosch-Herold M, Eisner RL, Stillman AE, Oshinski JN. A new method for the determination of aortic pulse wave velocity using cross-correlation on 2D PCMR velocity data. J Magn Reson Imaging 2008;27(6):1382-7.
10. Shen X, Schnell S, Barker AJ, Suwa K, Tashakkor L, Jarvis K, Carr JC, Collins JD, Prabhakaran S, Markl M. Voxel-by-voxel 4D flow MRI-based assessment of regional reverse flow in the aorta. J Magn Reson Imaging 2018;47(5):1276-1286.
Figures