0409
Free-running 3D Whole Heart Myocardial T1 Mapping with High Isotropic Spatial Resolution1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Center for Biomedical Imaging Research, Department of Biomedical Engineering, Tsinghua University, Beijing, China
Synopsis
Myocardial T1 mapping provides quantitative tissue characterization for the assessment of various cardiomyopathies. However, currently available myocardial T1 mapping techniques still have several limitations such as insufficient coverage, low spatial resolution, and the need of acquiring the data under multiple breath-holds. To overcome these problems, here we propose a free-running (free-breathing, no ECG gating) 3D whole heart T1 mapping technique with high isotropic spatial resolution. This approach allows for myocardial T1 mapping at arbitrary cardiac phases, enabling high-resolution dynamic T1 maps. The feasibility of the proposed sequence was validated against conventional methods in phantom and five healthy subjects.
Introduction
T1 mapping has great potential for myocardial fibrosis characterization (1). Myocardial T1 mapping usually requires breath-holds and ECG-gating to minimize the impact of respiratory and cardiac motion (2). Currently available myocardial T1 mapping techniques also have limitations such as insufficient coverage and/or low spatial resolution. To fully characterize diffuse diseases of the myocardium, free-breathing T1 mapping with whole heart coverage and high isotropic spatial resolution is desired (3). In this study, we propose to combine an inversion recovery (IR)-prepared 3D radial acquisition with low-rank inversion (4) and patch-based reconstruction (5), enabling free-running (free-breathing, no ECG gating) 3D myocardial T1 mapping with high isotropic spatial resolution.Methods
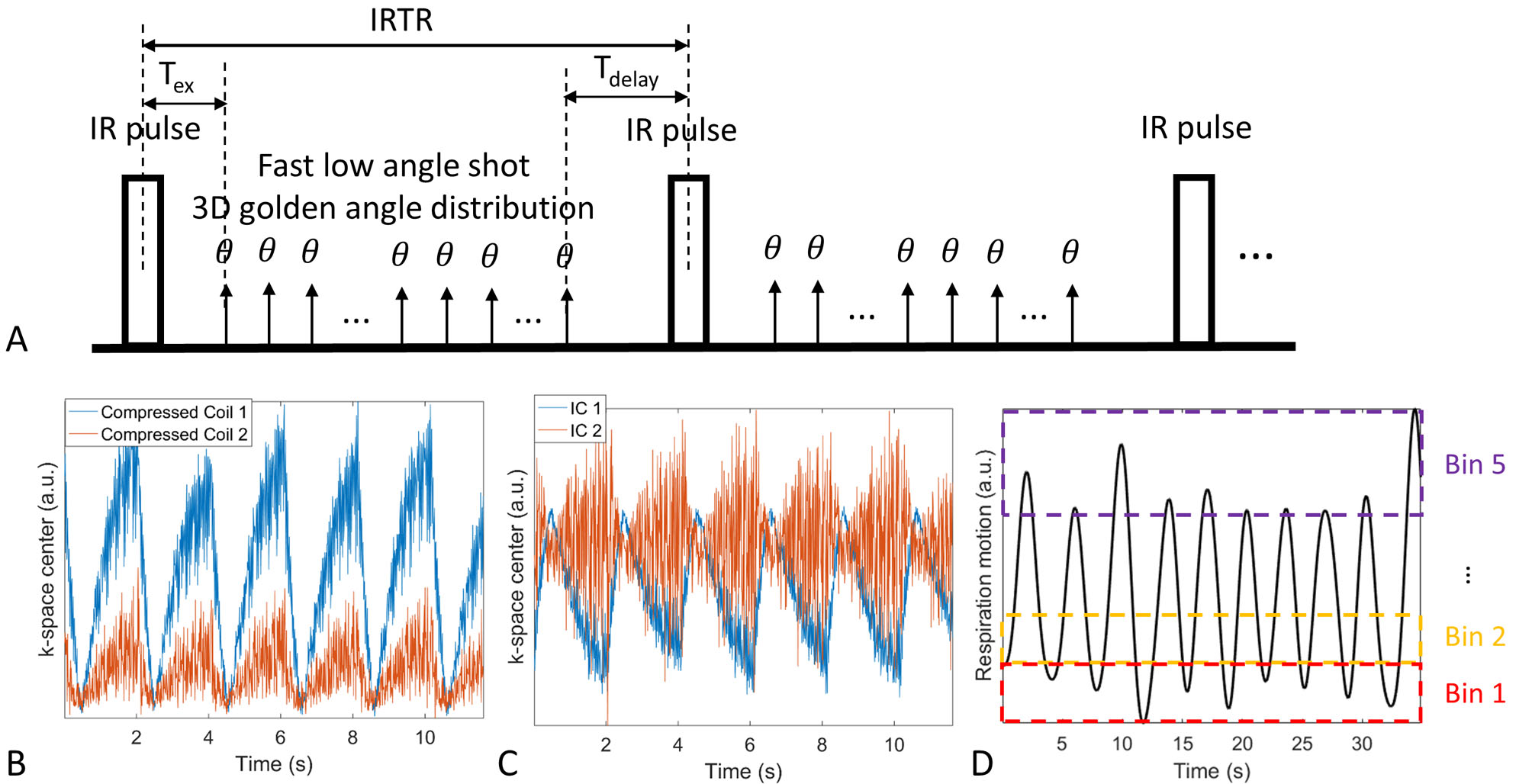
Sequence Design: The proposed IR-prepared 3D radial sequence is shown in Fig.1A. The sequence continuously acquires radial spokes conforming to the 3D golden angle distribution (6) to achieve pseudo-uniform distribution of spokes binned into arbitrary cardiac phases and T1 contrasts. The sequence was implemented on a 1.5T Philips MR scanner. Relevant scan parameters were: FOV=200mm3, spatial resolution=1.5mm3, TR/TE/flip angle=11.6ms/5.1ms/6°, water-excitation, scan time=9.5min.
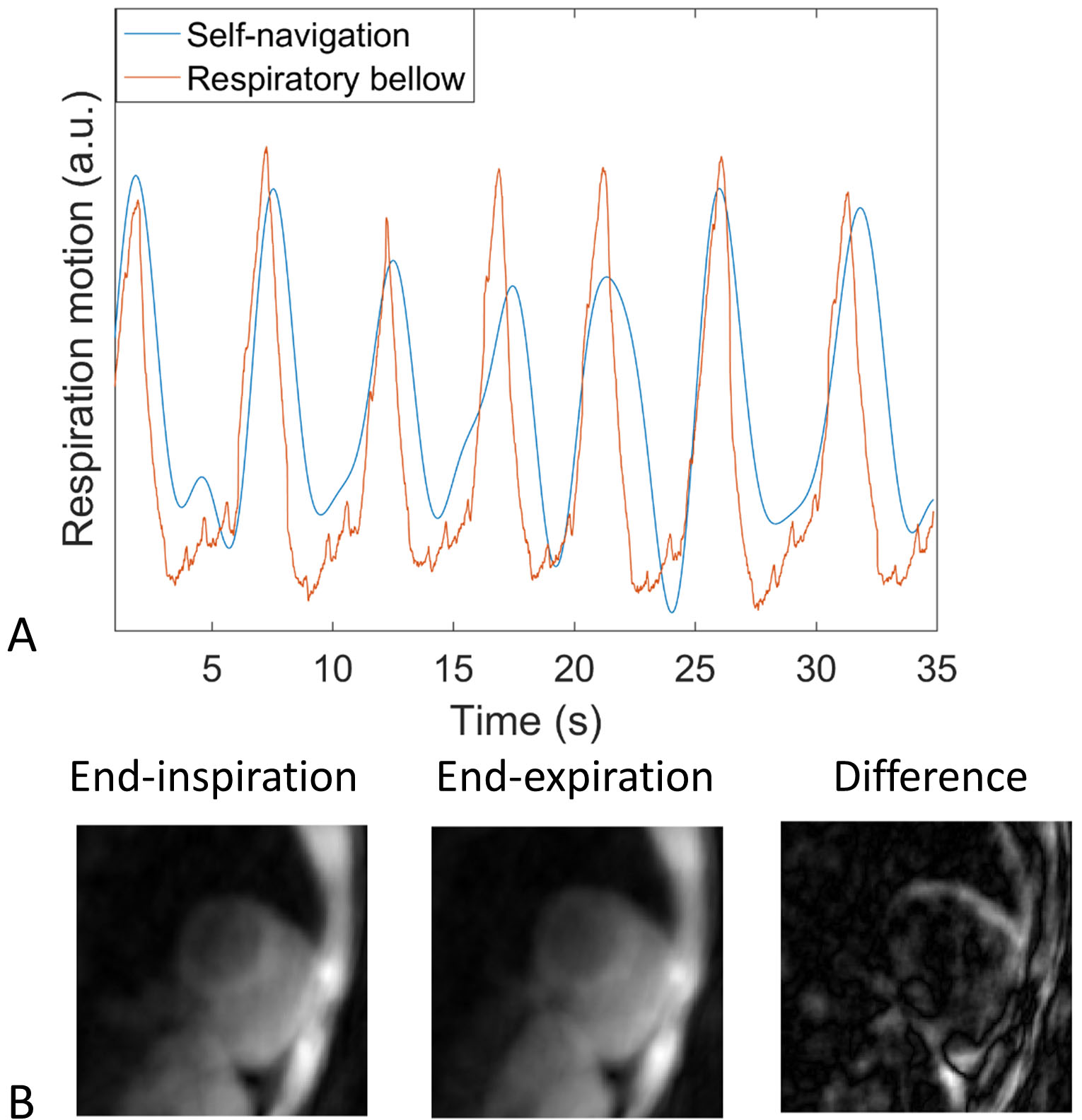
Motion Binning and Reconstruction: Superior-inferior 1D respiratory motion was estimated from the k-space center of all spokes (Fig. 1B, C), and used to bin the k-space data into 5 equally populated respiratory phases (Fig. 1D). This self-navigated respiratory signal was validated against the corresponding respiratory bellow signal (Fig. 2A). The ECG signal was recorded and used to bin the acquired data into different cardiac phases. 3D translational respiratory motion was estimated from the intermediate reconstruction of low-resolution respiratory bin images at diastole cardiac phase (Fig. 2B). Respiratory motion correction was performed by correcting the phase of the k-space data using the estimated 3D translation motion parameters. The respiratory motion corrected k-space data was then binned into different T1 contrasts and cardiac phases. To reconstruct T1 image series at specific cardiac phase, parallel imaging, dictionary-based low-rank inversion (4), which exploits temporal compression along the contrast dimension, and patch-based reconstruction (5), which exploits local and non-local redundancy of 3D patches, were combined. The optimization problem can be formulated as an unconstrained Lagrangian formulation: $$L\left(I,\alpha,Y\right)=argmin\parallel EI-K \parallel_2^2+\lambda\parallel \alpha \parallel_0+\mu\parallel I-P\alpha-Y \parallel_2^2$$where $$$I$$$ denotes the compressed image series; $$$E=AU_{r}FS$$$ is the encoding operator, with $$$S$$$ being sensitivity maps, $$$F$$$ being Fourier Transform, $$$U_{r}$$$ being the low rank operator obtained by truncating the singular value decomposition of the dictionary by Bloch simulation, $$$A$$$ being the k-space sampling operator; $$$K$$$ is the undersampled data; $$$P$$$ is the patch grouping operator and $$$\alpha$$$ are the associated sparse coefficients; $$$Y$$$ is the Augmented Lagrangian multiplier; $$$\lambda$$$ controls the sparsity regularization contribution and $$$\mu$$$ is the penalty parameter. The above equation can be efficiently solved by operator-splitting via alternating direction method of multipliers (ADMM) (5). A dot product matching between the reconstructed singular value images and the dictionary was performed to generate the T1 maps.
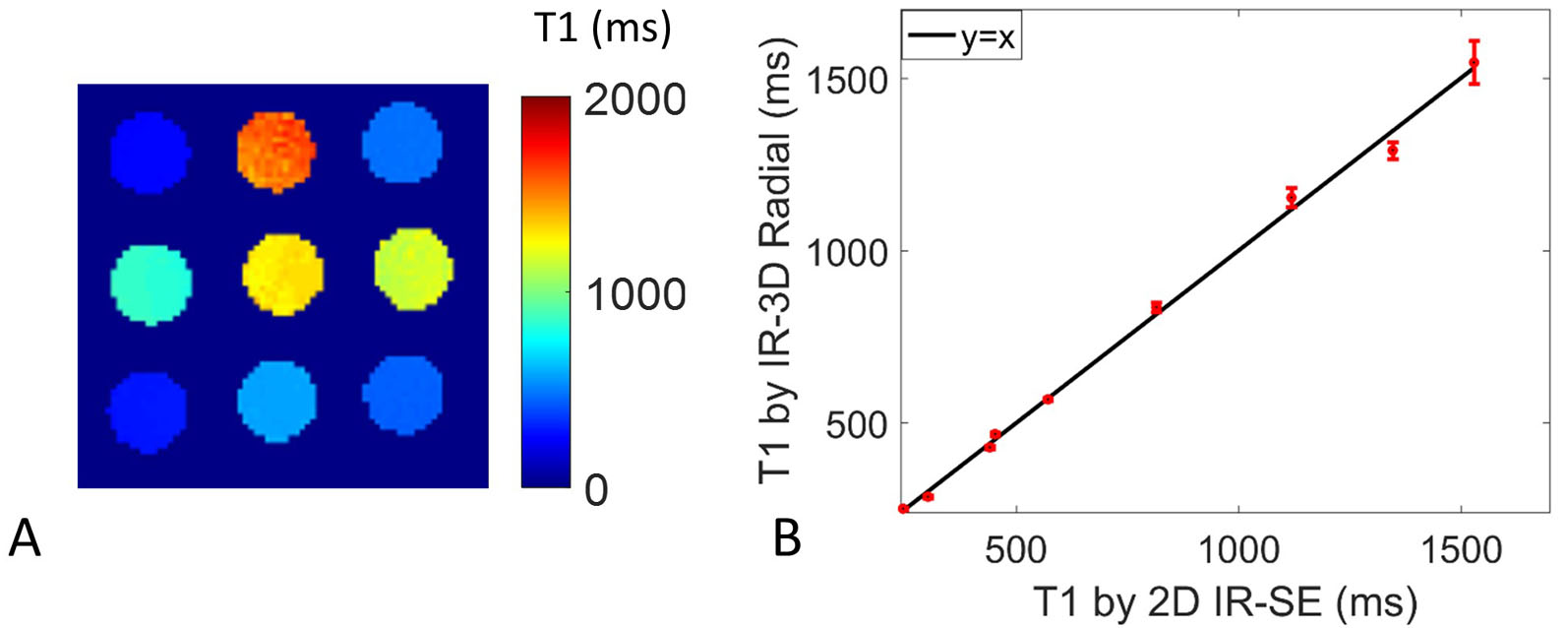
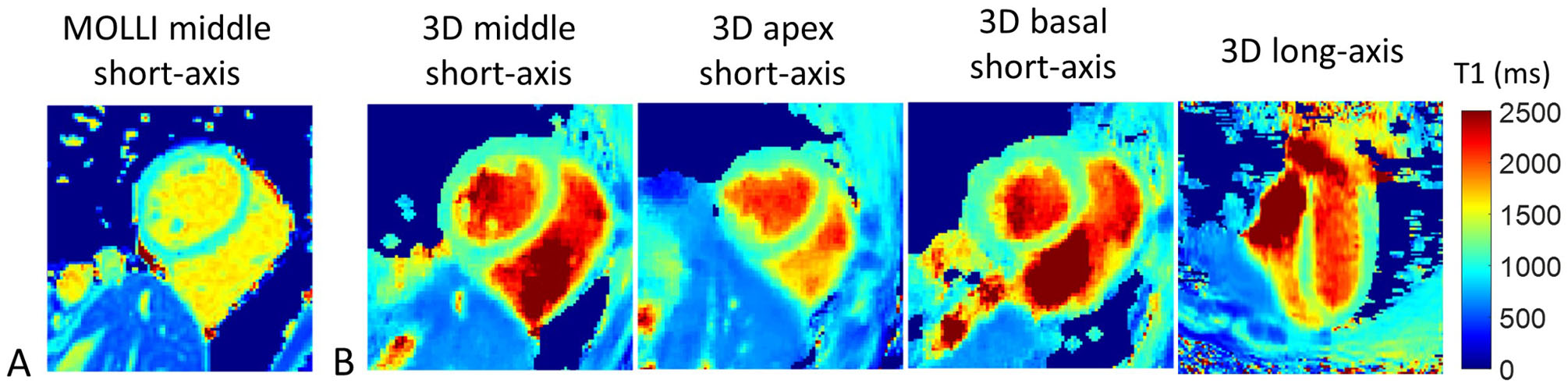
MR Imaging: Phantom experiments were performed to test the accuracy of the proposed sequence using the 2D IR spin echo (IR-SE) sequence as gold standard. For the in vivo study, five healthy subjects (2 females, 29.2±3.3 years) were scanned with the proposed free-running 3D T1 mapping and a conventional 2D breath-hold, ECG-gated MOLLI sequence (7). Imaging was performed in the short axis orientation, with MOLLI imaging slice positioned at mid-ventricle, whereas the proposed sequence covered the whole heart.
Results
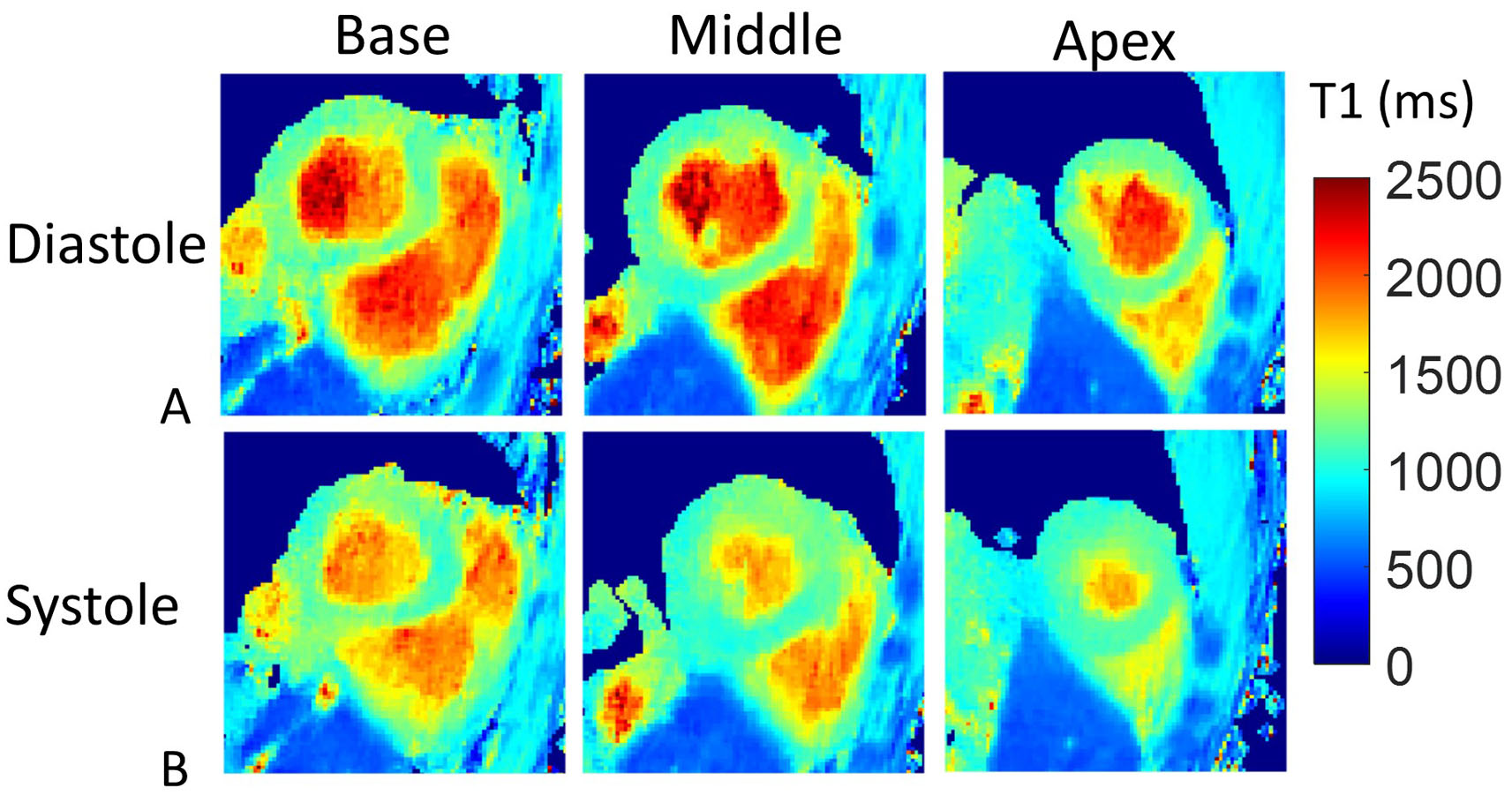
Phantom T1 mapping results are shown in Fig. 3, where good accuracy and precision can be observed for the proposed method. T1 mapping results at diastole are shown in Fig. 4 for one representative subject, including three short-axis slices and a long-axis slice from the 3D T1 mapping approach and a middle short-axis slice by 2D MOLLI. T1 mapping results from another subject are shown in Fig. 5, where three short-axis slices at both diastole and systole are demonstrated. T1 of the septum using the 3D T1 mapping method (1175.8±17.3ms) is slightly higher than MOLLI (1040.4±22.3ms) as expected, as 2D MOLLI has been reported to underestimate T1 (2).Discussion
Free-running 3D whole heart myocardial T1 mapping with 1.5mm isotropic spatial resolution has been successfully achieved with 100% respiratory efficiency. This sequence allows for reconstruction of high resolution 3D T1 maps at arbitrary cardiac phase, potentially enabling simultaneous cardiac function assessment and T1 tissue characterization. The sequence was investigated at 1.5T but further benefits of signal-to-noise ratio, and thus shortened scan time or improved resolution, are expected at 3T. Future work will also investigate the simultaneous reconstruction of different cardiac phases, exploiting redundancy in the cardiac phase dimension.Acknowledgements
This work was supported by the following grants: EPSRC EP/P032311/1, EP/P001009/1 and EP/P007619/1.References
1. Perea RJ, Ortiz-Perez JT, Sole M, Cibeira MT, de Caralt TM, Prat-Gonzalez S, Bosch X, Berruezo A, Sanchez M, Blade J. T1 mapping: characterisation of myocardial interstitial space. Insights Imaging 2015;6(2):189-202.
2. Kellman P, Hansen MS. T1-mapping in the heart: accuracy and precision. J Cardiovasc Magn Reson 2014;16:2.
3. Messroghli DR, Moon JC, Ferreira VM, Grosse-Wortmann L, He T, Kellman P, Mascherbauer J, Nezafat R, Salerno M, Schelbert EB, Taylor AJ, Thompson R, Ugander M, van Heeswijk RB, Friedrich MG. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: A consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI). J Cardiovasc Magn Reson 2017;19(1):75.
4. Asslander J, Cloos MA, Knoll F, Sodickson DK, Hennig J, Lattanzi R. Low rank alternating direction method of multipliers reconstruction for MR fingerprinting. Magn Reson Med 2018;79(1):83-96.
5. Bustin A, Ginami G, Cruz G, Correia T, Ismail TF, Rashid I, Neji R, Botnar RM, Prieto C. Five-minute whole-heart coronary MRA with sub-millimeter isotropic resolution, 100% respiratory scan efficiency, and 3D-PROST reconstruction. Magn Reson Med 2018.
6. Chan RW, Ramsay EA, Cunningham CH, Plewes DB. Temporal Stability of Adaptive 3D Radial MRI Using Multidimensional Golden Means. Magnetic Resonance in Medicine 2009;61(2):354-363.
7. Ugander M, Oki AJ, Hsu LY, Kellman P, Greiser A, Chen MY, Bandettini WP, Aletras AH, Arai AE. Myocardial Extracellular Volume Imaging by MRI Quantitatively Characterizes Myocardial Infarction and Subclinical Myocardial Fibrosis. Circulation 2010;122(21).
Figures