0404
Diffusion tensor cardiovascular magnetic resonance in a Langendorff perfused beating porcine heart1Cardiovascular Magnetic Resonance Unit, The Royal Brompton Hospital and Imperial College London, London, United Kingdom, 2Department of Perfusion, The Royal Brompton Hospital, London, United Kingdom, 3Translational Biomedical Research Centre, University of Bristol, Bristol, United Kingdom, 4National Heart and Lung Institute, Imperial College London, London, United Kingdom, 5Magdi Yacoub Institute, Imperial College London, London, United Kingdom, 6Aeronautics, Imperial College London, London, United Kingdom
Synopsis
We have developed an MRI compatible Langendorff perfused beating isolated porcine heart model. Hearts are harvested and transported to a remote imaging centre, avoiding the need for onsite pre-clinical facilities. The model allows comparison of beating and arrested data in equivalent cardiac states. We performed cine imaging, parametric mapping and diffusion tensor cardiovascular magnetic resonance in the beating and arrested hearts. After MRI, co-localised 3D histology is performed.
Background
Previous studies have used large animal models for validation of diffusion tensor cardiovascular magnetic resonance (DT-CMR) [1,2] and small animal isolated perfused hearts have been used to evaluate cardiac microstructure in relaxed and contracted states [3]. In this work, we present initial DT-CMR results from a large animal isolated perfused beating heart model [4] providing microstructure in arrested and beating hearts in contracted and relaxed states.Methods
Hearts were harvested from large white pigs (~60-80kg) by a specialist surgical team at a clinical standard facility based on a heart transplant protocol, with a long section of intact aorta. Hearts were arrested and protected using cardioplegia and topical cooling for transport to the remote imaging site, with a cold ischemic time of ~2.5-3hours.
The aorta was attached to a custom 3D printed cannula in the magnet room and Langendorff perfused (retrograde through the aorta, feeding the coronary arteries) with a modified Tyrode’s solution at room temperature (figure 1). A standard bypass pump system and heater cooler with a custom perfusion tubing set was used to oxygenate at 100% O2. An initial heat-exchanger/membrane oxygenator was located in the control room and a secondary heat exchanger was located on the scanner bed to account for heat loss along the perfusion tubing. A flexible tube inserted through a pulmonary vein, left atrium and the mitral valve was used to relieve excess intracavity left ventricular pressure. Perfusion flow and temperature were increased gradually (38°C, ~350ml/min). Defibrillation with 10-30J was performed when hearts entered ventricular fibrillation. Once the hearts began to contract, autologous washed blood (0.5-1L whole) was added to the perfusate and the mixture was recirculated. Hearts were electrically paced above the intrinsic rate (70-100bpm).
The beating heart was transferred to a custom 3D printed chamber holding the heart at the magnet isocentre and allowing a small surface coil to be wrapped around. A 3T Skyra (Siemens) was used to acquire cine, DT-CMR and parametric mapping in the beating heart, triggered from the pacing system. Pacing was then stopped and high potassium Tyrode’s perfusate (blood free) was used to arrest hearts in a relaxed state. Next, sodium-free high-lithium perfusion (again, blood free) induced contracture. DT-CMR and parametric mapping were repeated in both arrested states after sufficient settling time.
DT-CMR was performed using a monopolar STEAM EPI sequence in a single mid-ventricular short-axis slice with b=150 and 500smm-2 [5].
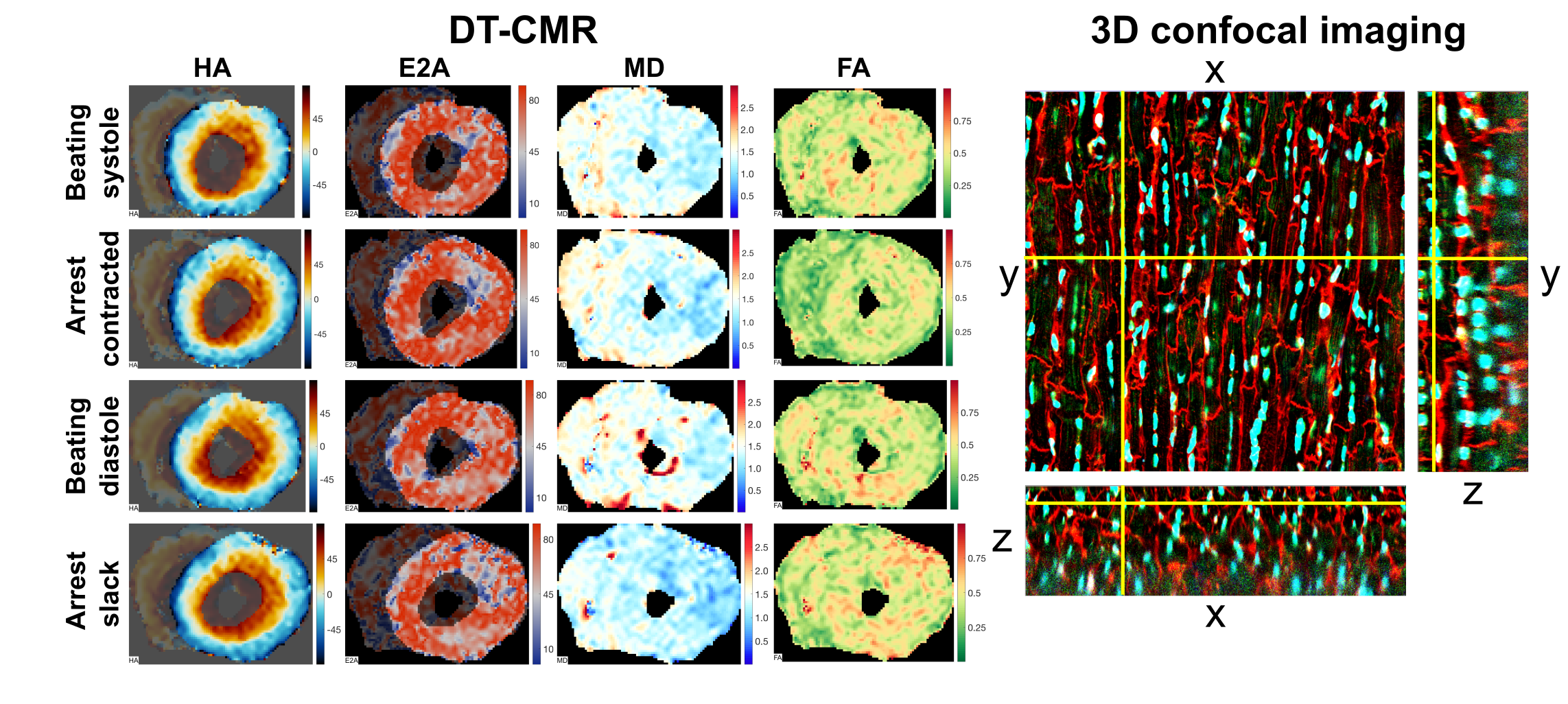
Oil filled tubes within the bed of the imaging chamber provided fiducial markers, allowing blocks of tissue to be cut in the plane of the DT-CMR data after imaging was complete. Histological sections were cut from these blocks (100µm for 3D confocal imaging – DAPI and WGA, 10µm for widefield, Masson staining).
Results
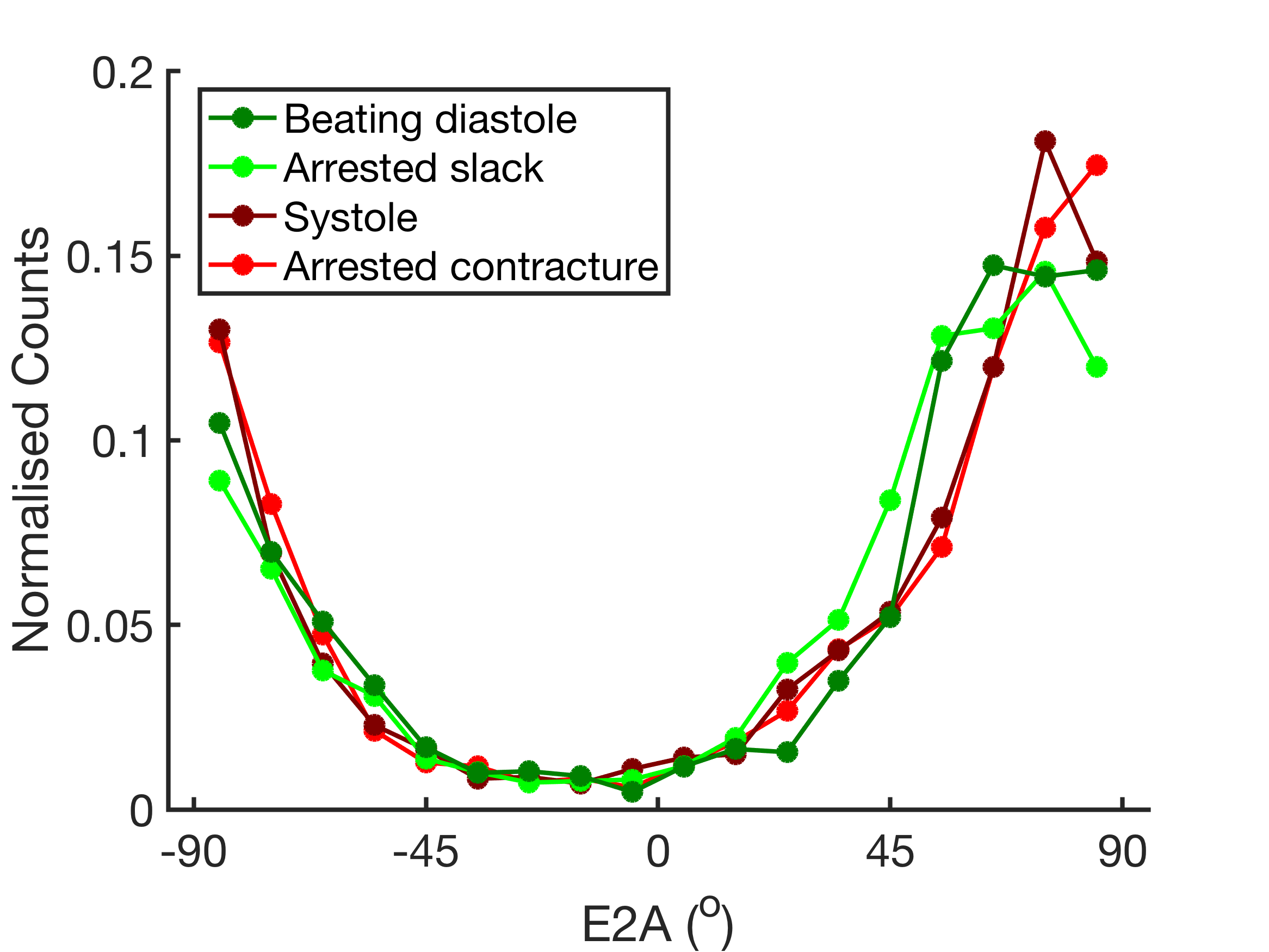
Hearts were harvested from 10 pigs and 6 were successfully established in beating heart mode (S=success, F=failure: FFSFFSSSSS). Here we show results from heart 10, where data was acquired in beating and arrested, contracted and relaxed states. Example video of the beating heart is shown in figure 2, with cine CMR data in figure 3. Example DT-CMR result images and corresponding 3D histology are shown figure 4. For beating diastole, systole, arrested relaxed and arrested contracted states T2 values were 68ms, 78ms, 101ms and 105ms; mean left ventricular (LV) mean diffusivity (MD) was 1.47, 1.38, 1.18 and 1.35 x10-3 mm2s-1, mean LV FA was 0.45, 0.46, 0.49 and 0.41 and median LV E2A, a measure of sheetlet orientation [1], was 68˚, 71˚, 66 ˚ and 72 ˚ respectively. Figure 5 shows histograms of second eigenvector angle (E2A), demonstrating a good similarity between equivalent arrested and beating states, but minimal change between contracture and slack states.Discussion
We have developed an MRI compatible Langendorff perfused isolated beating porcine heart model and obtained microstructural information via DT-CMR in relaxed and contracted beating and arrested hearts in a centre without pre-clinical facilities. Despite the use of a dextran colloid and autologous blood in the perfusate, the hearts were edematous, demonstrated by the elevated T2 and MD. The sheetlet angles (E2A) in the edematous heart appeared systolic like in all states with a severely reduced range of sheetlet mobility. This has implications for the effects of edema on sheetlet function. Future work will optimise perfusate constituents and the perfusion protocol to address the edema in this powerful model for pre-clinical microstructural imaging.Acknowledgements
Support from BHF grants RE/13/4/30184, PG/14/68/30798, Institute of Physics and Engineering Research and Innovation Award. We acknowledge further support from the Royal Brompton Clinical Engineering Department, Alex Berry (3D printing and design) and the Facility for Imaging Light Microscopy Imperial College London.References
1. Nielles-Vallespin et al. Myocardial microstructural dynamics by in-vivo diffusion tensor CMR: preclinical validation and clinical translation in DCM and HCM. J Am Coll Cardiol. 2017. 69: 661. DOI:10.1016/j.jacc.2016.11.051.
2. Stoeck et al. Direct comparison of in vivo versus postmortem second‐order motion‐compensated cardiac diffusion tensor imaging. Magn Reson Med 2017. 79:2265. DOI:10.1002/mrm.26871
3. Hales et al. Histo-anatomical structure of the living isolated rat heart in two contraction states assessed by diffusion tensor MRI. Prog Biophys Mol Biol 2012. 110: 319. DOI:10.1016/j.pbiomolbio.2012.07.014
4. Schuster et al. An isolated perfused pig heart model for the development, validation and translation of novel cardiovascular magnetic resonance techniques. J Cardiovasc Magn Reson 2010. 12:52. DOI:10.1186/1532-429X-12-53
5. Scott AD et al. Optimal diffusion weighting for in vivo cardiac diffusion tensor imaging. Magnetic Resonance in Medicine 2014; 74(2). DOI:10.1002/mrm.25418
Figures