0402
Motion-corrected 3D high-resolution fat-water imaging of the heart1Physikalisch-Technische Bundesanstalt (PTB), Braunschweig and Berlin, Germany, 2Department of Cardiac, Thoracic and Vascular Sciences, University of Padua, Padua, Italy, 3Charité Medical Faculty University Medicine, Berlin, Germany, 4Working Group on Cardiovascular Magnetic Resonance, Experimental and Clinical Research Center (ECRC), DZHK partner site Berlin, Berlin, Germany, 5Department of Cardiology and Nephrology, HELIOS Klinikum Berlin Buch, Berlin, Germany
Synopsis
Fat infiltration in the myocardium is of great clinical interest as potential predictor of poor prognosis in patients with either ischemic or non-ischemic cardiac diseases. Commonly, 2D chemical shift encoded MR methods are used to obtain fat-water separated images. Nevertheless, fat infiltrations are often small and hence could be missed due to poor slice resolution. Here we propose a free-breathing 3D whole-heart fat-water imaging approach with an isotropic resolution of 1.5mm3, which uses respiratory motion correction and retrospective cardiac gating. The approach was evaluated in five patients demonstrating accurate visualisation of the heart and small fat infiltrations in the myocardium.
Introduction
The identification of fat in the myocardium is of great clinical interest, because of the high prognostic significance in patients with ischemic or non-ischemic disorders and the potential role as a substrate for arrhythmia1–4. Due to the short T1 time, fat is difficult to distinguish from myocardial fibrosis in late gadolinium enhancement (LGE)-MRI in these patients. Chemical shift encoded MRI (i.e. fat-water imaging) using, for example, a Dixon approach, has been shown to provide accurate fat visualisation and quantification in the heart5. However, the commonly used 2D technique could fail to identify myocardial fat infiltrations, because they can be sometimes very small6. The main challenge of 3D high-resolution fat-water imaging is long scan times because multiple images at different echo times need to be acquired. Several 3D fat-water imaging techniques have been proposed for the heart, but they often do not provide high isotropic resolution. In particular, the necessary respiratory gating can lead to even longer scan times, depending on the breathing pattern of the patient7,8.
Here we propose to use a continuous free-breathing 3D whole-heart fat-water imaging approach with an isotropic resolution of 1.5mm3, which uses respiratory motion correction and retrospective cardiac gating to minimize motion artefacts and ensure accurate fat visualisation.
Methods
Data acquisition: Figure 1 gives an overview of the proposed data acquisition and image reconstruction. A triple-echo spoiled gradient echo acquisition with a Golden Radial Phase Encoding (GRPE) trajectory was used to obtain 3D data continuously during free-breathing, covering a FOV of 288mm3 with an isotropic resolution of 1.5mm3 (TE1/TE2/TE3/TR: 2.9/4.5/6.1/8.2ms, FA: 15°) on 1.5T MR Scanner (Avanto Fit, Siemens Healtineers)9. Total acquisition time was 13:30min.
Image reconstruction: In a first step, respiratory resolved 3D images of the first echo are reconstructed based on a self-navigator signal using spatial and temporal total variation regularization to minimize undersampling artefacs10. A non-rigid image registration approach is used to obtain 3D motion vector fields describing how each pixel moved relative to a reference image in end-expiration11. In a second step, the same raw data is split into different cardiac phases based on a recorded ECG-signal. Each phase corresponded to an acquisition window of ~200ms in each cardiac cycle depending on the heart rate. The motion vector fields are then utilized in a motion-corrected image reconstruction (MCIR) to obtain respiratory motion-corrected images at three echo times for multiple cardiac phases. A total-variation-based regularization is applied along the cardiac phase dimension to utilize temporal similarities and minimize undersampling artefacts. This two-step approach ensures minimization of both respiratory and cardiac motion artefacts.
Fat-water separation: An iterative fat-water separation approach was used to obtain fat and water images from the mid-diastolic cardiac phase12.
Patient experiments: The proposed approach was applied in 5 patients after the injection of a Gadolinium-based contrast agent (Gadoteridol, 0.4ml/kg). For comparison, standard 2D dark-blood fat-water (spoiled GRE, resolution: 1.4x1.9x8mm3, TE1/TE2/TE3/TR: 1.6/3.9/6.3/10.4ms, FA: 12°) and 2D LGE (balanced SSFP, resolution: 1.8x1.8x6 mm3, TE/TR: 1.2/3.4ms, FA: 56°) images were also obtained in 2-, 3- and 4-chamber view during breathhold.
Results
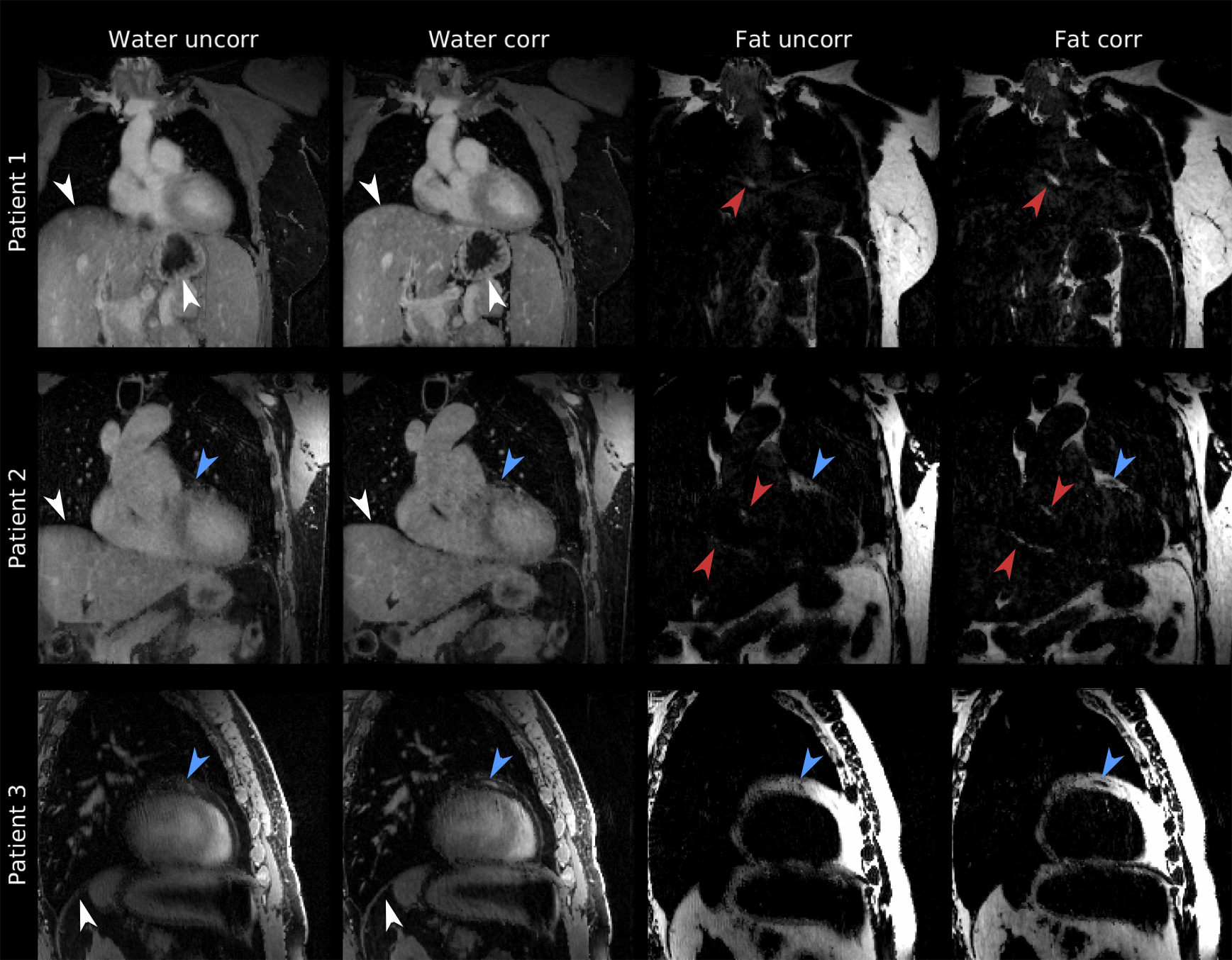
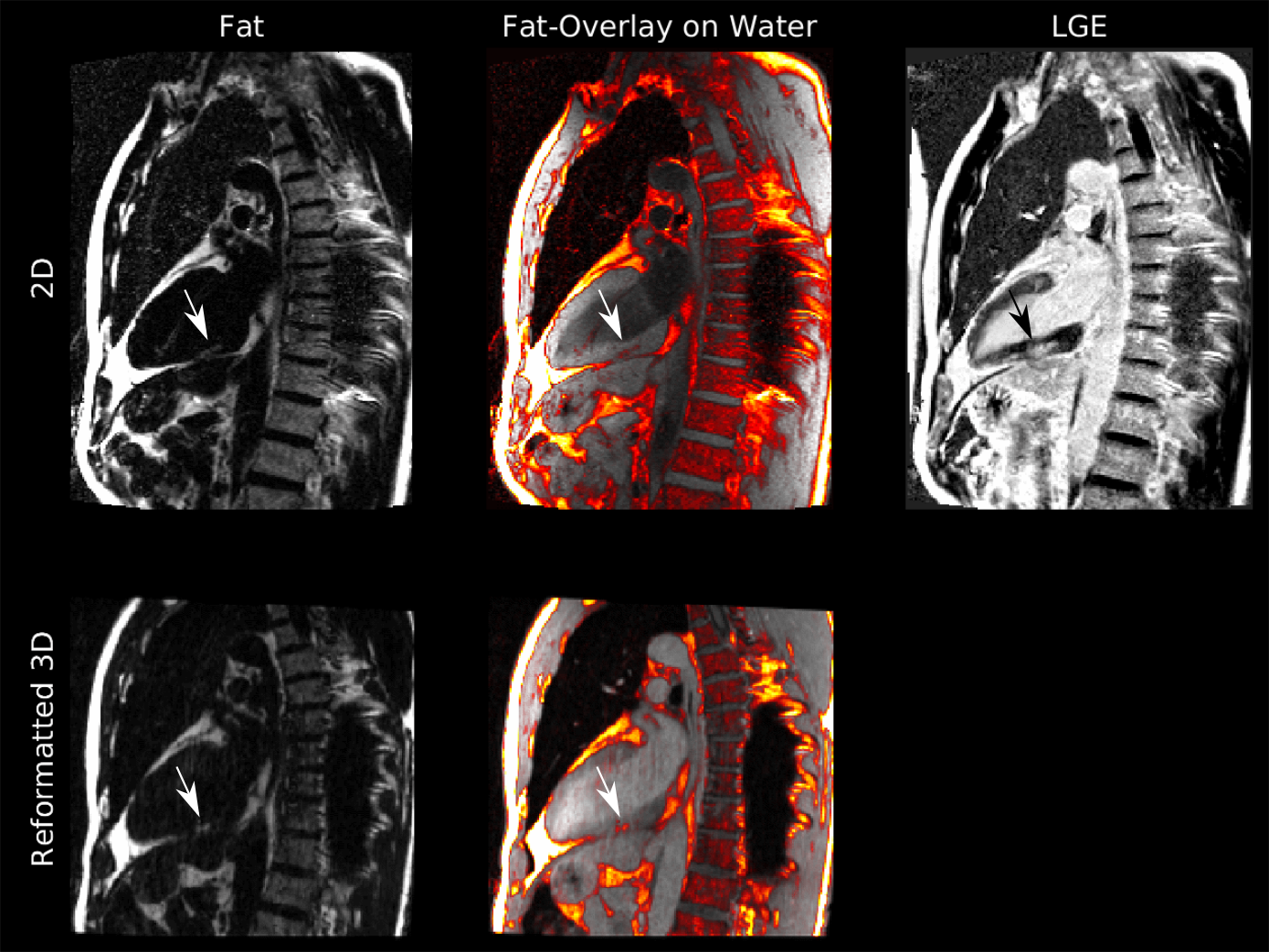
Figure 2 compares water and fat images without motion correction and with the proposed technique. Motion blurring of the anatomy of the heart and the surrounding organs is strongly reduced. Small features such as the coronary artery and thin fat layers around the heart can be clearly seen. The 3D data allows for reformatting in 2-, 3- and 4-chamber view. The reformatted images are compared to standard 2D fat-water images in Figure 3. Both approaches provide an accurate depiction of fat structure around the heart. Figure 4 shows a patient with myocardial fat infiltration in the inferior wall of the left ventricle, readily appreciable in the 2D and reformatted 3D images.Acknowledgements
No acknowledgement found.References
1. Goldfarb JW, Roth M, Han J. Myocardial Fat Deposition after Left Ventricular Myocardial Infarction: Assessment by Using MR Water-Fat Separation Imaging. Radiology. 2009;253(1):65-73.
2. Mordi I, Radjenovic A, Stanton T, et al. Prevalence and Prognostic Significance of Lipomatous Metaplasia in Patients With Prior Myocardial Infarction. JACC Cardiovasc Imaging. 2015;8(9):1111-1112.
3. Homsi R, Sprinkart AM, Gieseke J, et al. 3D-Dixon cardiac magnetic resonance detects an increased epicardial fat volume in hypertensive men with myocardial infarction. Eur J Radiol. 2016;85(5):936-942.
4. Samanta R, Pouliopoulos J, Thiagalingam A, Kovoor P. Role of adipose tissue in the pathogenesis of cardiac arrhythmias. Hear Rhythm. 2016;13(1):311-320.
5. Kellman P, Hernando D, Arai AE. Myocardial Fat Imaging. Curr Cardiovasc Imaging Rep. 2010;3(2):83-91.
6. Schmacht L, Traber J, Grieben U, et al. Cardiac involvement in myotonic dystrophy type 2 patients with preserved ejection fraction: Detection by cardiovascular magnetic resonance. Circ Cardiovasc Imaging. 2016;9(7):1-10.
7. Börnert P, Koken P, Nehrke K, Eggers H, Ostendorf P. Water/fat-resolved whole-heart Dixon coronary MRA: An initial comparison. Magn Reson Med. 2014;71(1):156-163.
8. Taviani V, Hernando D, Francois CJ, et al. Whole-heart chemical shift encoded water-fat MRI. Magn Reson Med. 2014;72(3):718-725.
9. Kolbitsch C, Neji R, Fenchel M, Mallia A, Marsden P, Schaeffter T. Fully integrated 3D high-resolution multicontrast abdominal PET-MR with high scan efficiency. Magn Reson Med. 2018;79(2):900-911.
10. Cruz G, Atkinson D, Buerger C, Schaeffter T, Prieto C. Accelerated motion corrected three-dimensional abdominal MRI using total variation regularized SENSE reconstruction. Magn Reson Med. 2016;75(4):1484-1498.
11. Rueckert D, Sonoda LI, Hayes C, Hill DLG, Leach MO, Hawkes DJ. Nonrigid registration using free-form deformations: application to breast MR images. IEEE Trans Med Imaging. 1999;18(8):712-721.
12. Berglund J, Kullberg J. Three-dimensional water/fat separation and T2* estimation based on whole-image optimization-Application in breathhold liver imaging at 1.5 T. Magn Reson Med. 2012;67:1684-1693.
Figures

Figure 1: Overview. 3D MR data is acquired using a Golden Radial Phase Encoding (GRPE) trajectory. A self-navigator signal is obtained from a central k-space line. Based on this navigator signal, raw data is split into 8 respiratory phases and 3D images are reconstruction. Non-rigid motion fields are obtained using spline-based image registration. Based on an external ECG signal, MR raw data is split into different cardiac phases. Non-rigid motion fields are utilized to reconstruct respiratory motion-corrected (MCIR) images for each cardiac phase for each echo. Finally, images of the three echoes of the mid-diastolic cardiac phase are used to obtain fat and water images.