0401
Fast and Accurate Free-Breathing Whole-Heart 3D T2 Mapping1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Frimley, United Kingdom
Synopsis
T2 mapping is a promising quantitative imaging technique for the detection of myocardial edema. Conventionally, T2 mapping is performed using T2-prepared single-shot 2D acquisitions, acquiring multiple slices in several breath-holds. While showing high accuracy and reproducibility, breath-holding limits achievable spatial resolution and heart coverage and can be challenging in very sick patients. Here we propose a free-breathing whole-heart 3D T2 mapping technique with high isotropic spatial resolution in a clinically feasible scan time. This is achieved by combining an accelerated T2-prepared acquisition with patch-based reconstruction and dictionary-based signal matching. Feasibility of the proposed method was investigated in a standardized T1/T2 phantom and healthy subjects.
Purpose
T2 mapping is a promising quantitative technique for the detection of myocardial edema and has shown excellent diagnostic accuracy in patients with clinically suspected myocarditis [1]. Nowadays, T2 mapping is conventionally performed using T2-prepared single-shot 2D acquisitions, acquiring multiple slices in several breath-holds. While showing high accuracy and reproducibility, breath-holding limits achievable spatial resolution and heart coverage and can be challenging in very sick patients. Here we propose a free-breathing whole-heart 3D T2 mapping with high isotropic spatial resolution in a clinically feasible and predictable scan time. This Motion corrected Undersampled Signal maTched (MUST) T2 map is achieved by combining an accelerated T2-prepared acquisition with patch-based reconstruction and dictionary-based signal matching. The feasibility of MUST-T2 map was investigated in a standardized T1/T2 phantom and five healthy subjects and was compared against reference standard techniques.Methods
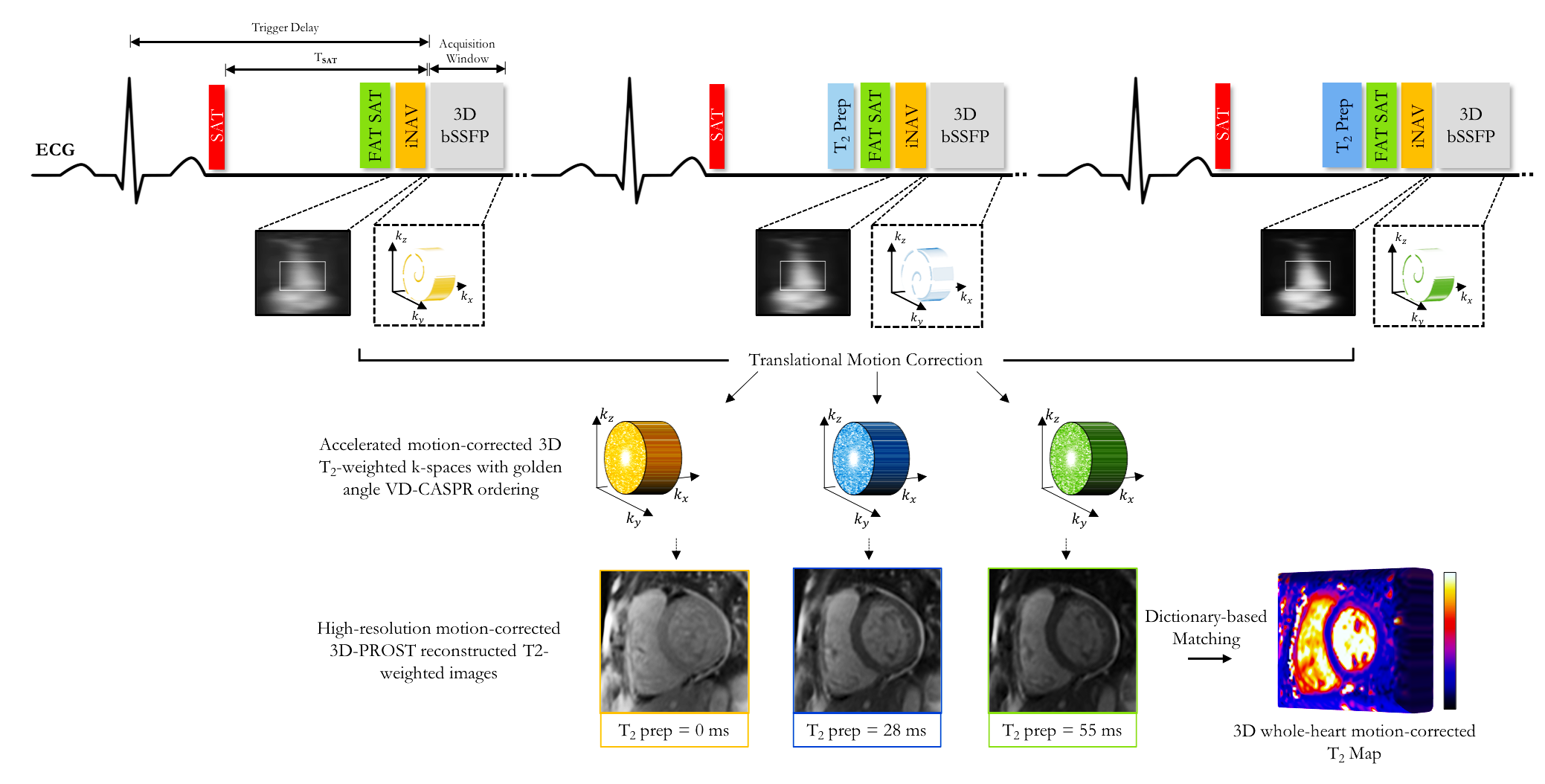
Acquisition: The proposed 3D whole-heart MUST-T2 mapping acquisition (Fig.1) consists of an ECG-triggered, T2-prepared, balanced steady-state free precession (bSSFP) sequence with nonselective saturation pulses. A saturation pulse is applied at each heartbeat to null magnetization history [2], ensuring insensitivity to heart rate. Three successive volumes are acquired with increasing T2 preparation times ([0,28,55]ms). An undersampled 3D Cartesian sampling with spiral order and variable density (VD-CASPR) is employed to accelerate the scan [3-4]. Spiral-like arms are rotated with the golden-angle within and between the three T2-prepared volumes to achieve incoherent aliasing. A 2D image-based navigator preceded each spiral acquisition to achieve 100% respiratory scan efficiency (no data rejection), predictable scan time and 2D translational motion estimation/correction of the heart [5]. A SPIR saturation pulse is also applied to ensure adequate fat suppression.
Reconstruction: The three motion-corrected T2-prepared k-spaces are individually reconstructed using a 3D patch-based low-rank reconstruction (3D-PROST [3]) that exploits local and non-local redundancies within the images. Extended phase graph simulations [6], matching the acquisition parameters, are carried out to generate a subject-specific dictionary. The dictionary was calculated for a T2 in the range of ([4:2:100,105:5:200,210:10:450]ms) and a fixed T1 of 1100ms. 3D quantitative T2 maps are generated by matching each measured signal evolution to the closest dictionary entry using dot product.
Imaging: Acquisitions were performed in a standardized T1/T2 phantom [7] and five healthy subjects (3 males, range 28-31years) on a 1.5T scanner (Magnetom Aera, Siemens Healthcare). Phantom – Relevant scan parameters included: TR/TE=3.2/1.42ms, FA=90°, bandwidth=910Hz/pixel, $$$T_{SAT}$$$=630ms, FOV=187x187x156mm3, and 1.5mm3 isotropic resolution. Scans were performed with a simulated heart rate of 60 beats per minute with different acceleration factors (up to 5-fold). In vivo – Scan parameters were similar to the phantom experiments except: FOV=320x320x80-90mm3, bandwidth=830Hz/pixel, subject specific mid-diastolic trigger delay, acquisition window (range ~85-109ms) and $$$T_{SAT}$$$ (range ~470-900ms), average acquisition time 7min54s. Data were acquired in free-breathing using the proposed 3D MUST-T2 map with a 5-fold acceleration.
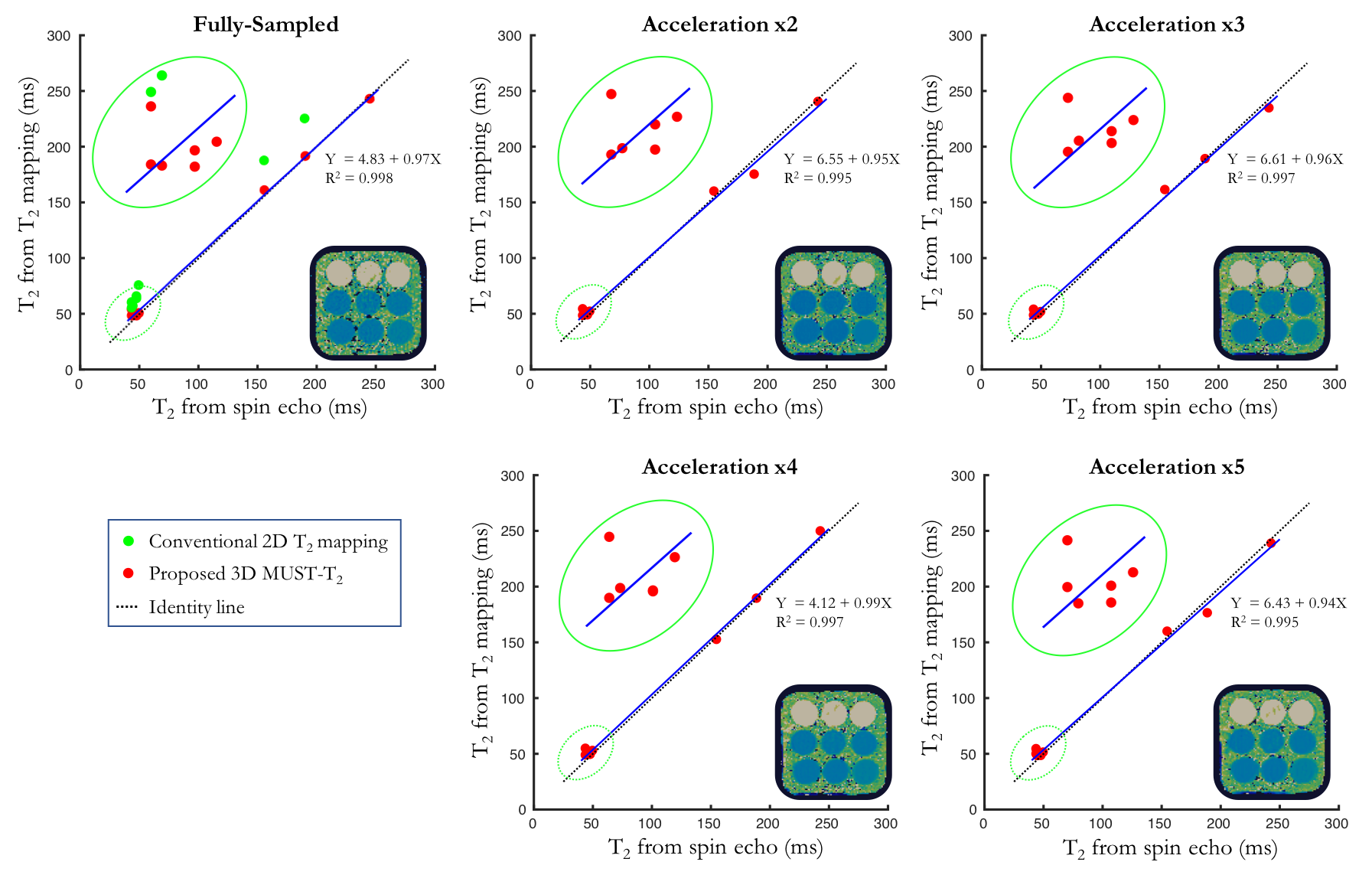
In both phantom and in vivo experiments, conventional 2D T2 mapping (T2-prepared single-shot 2D bSSFP, TE=[0,25,55]ms, three heart-beats recovery, resolution 1.9x1.9x8mm3, mono-exponential fitting) was performed for comparison purposes. Three slices were acquired in basal, midventricular and apical short-axis in three breath-holds of ~10s each. Mean and standard deviation of T2 values were extracted by drawing regions of interest across each of the nine vials (phantom) and in the myocardial septum (in vivo).
Results
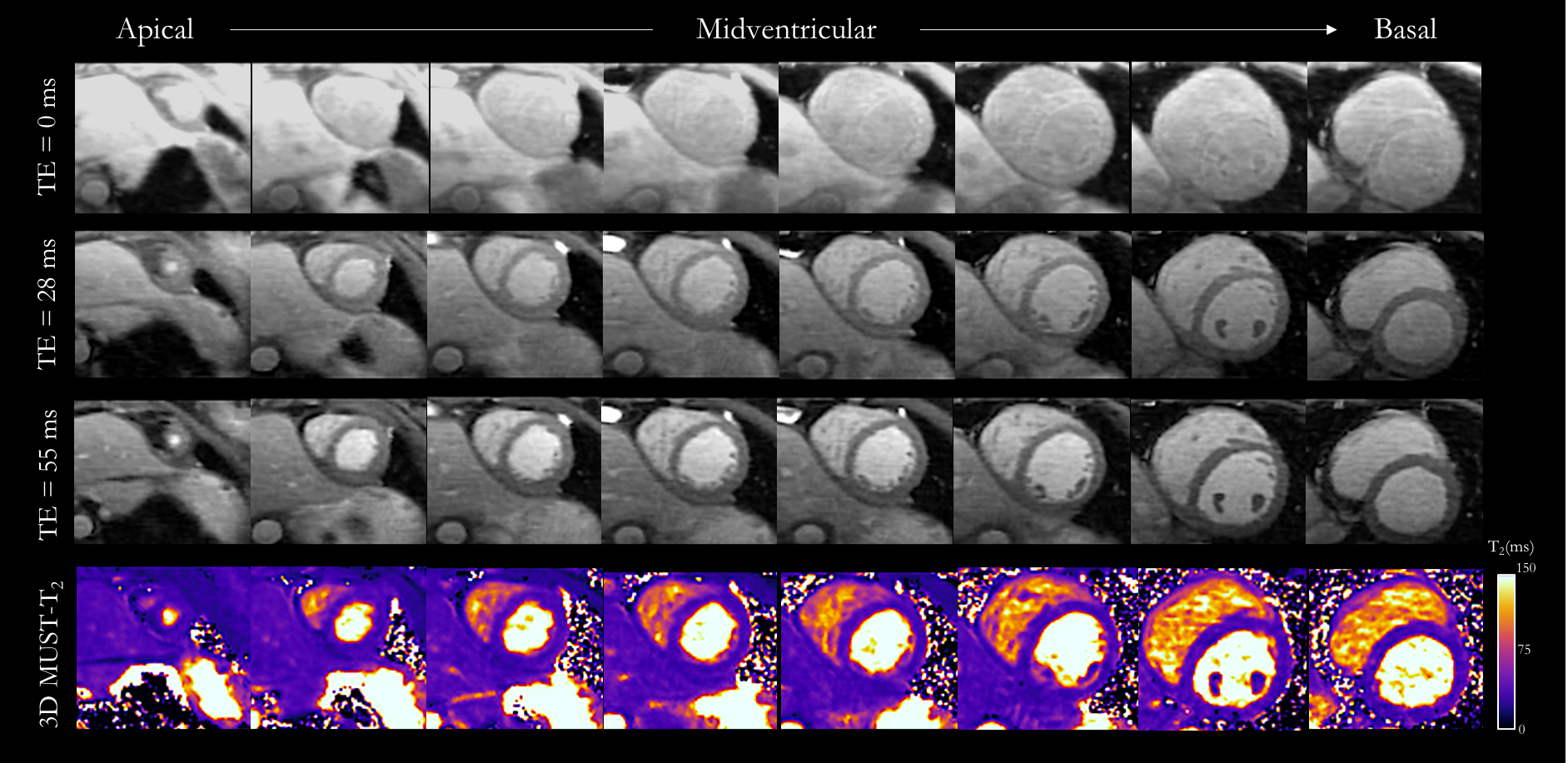
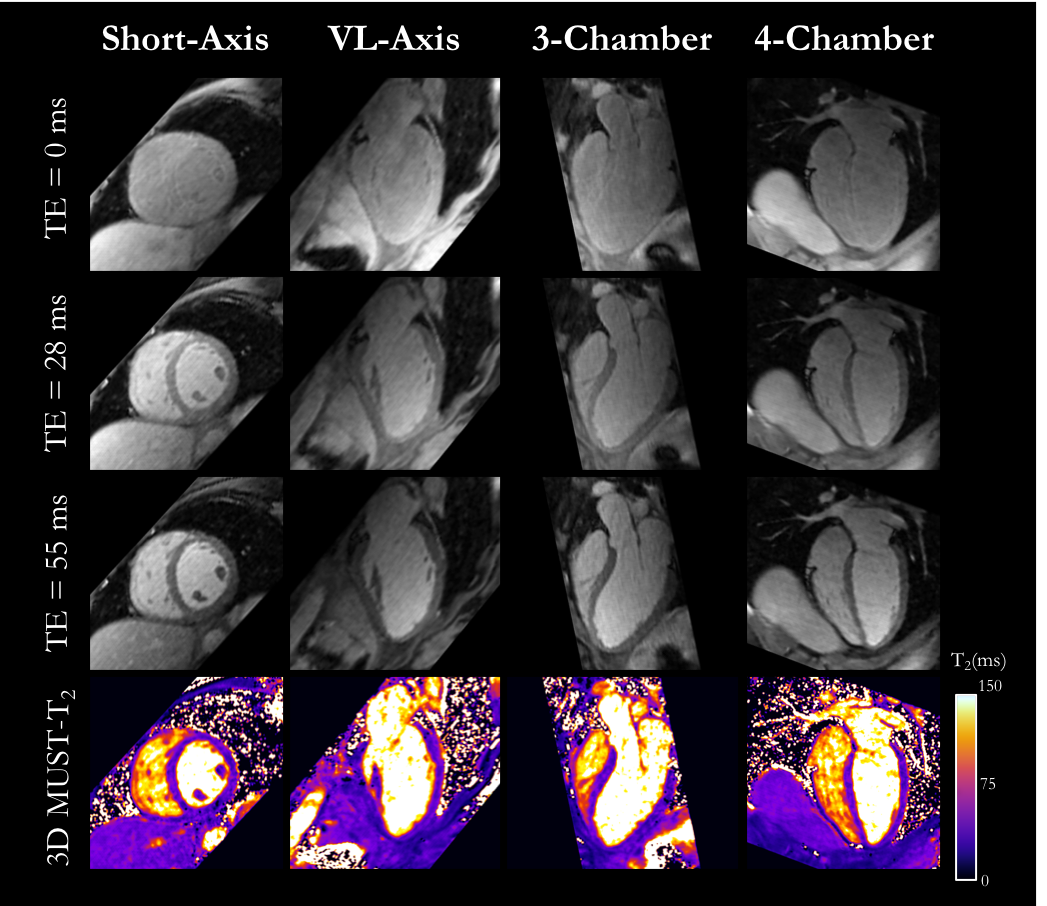
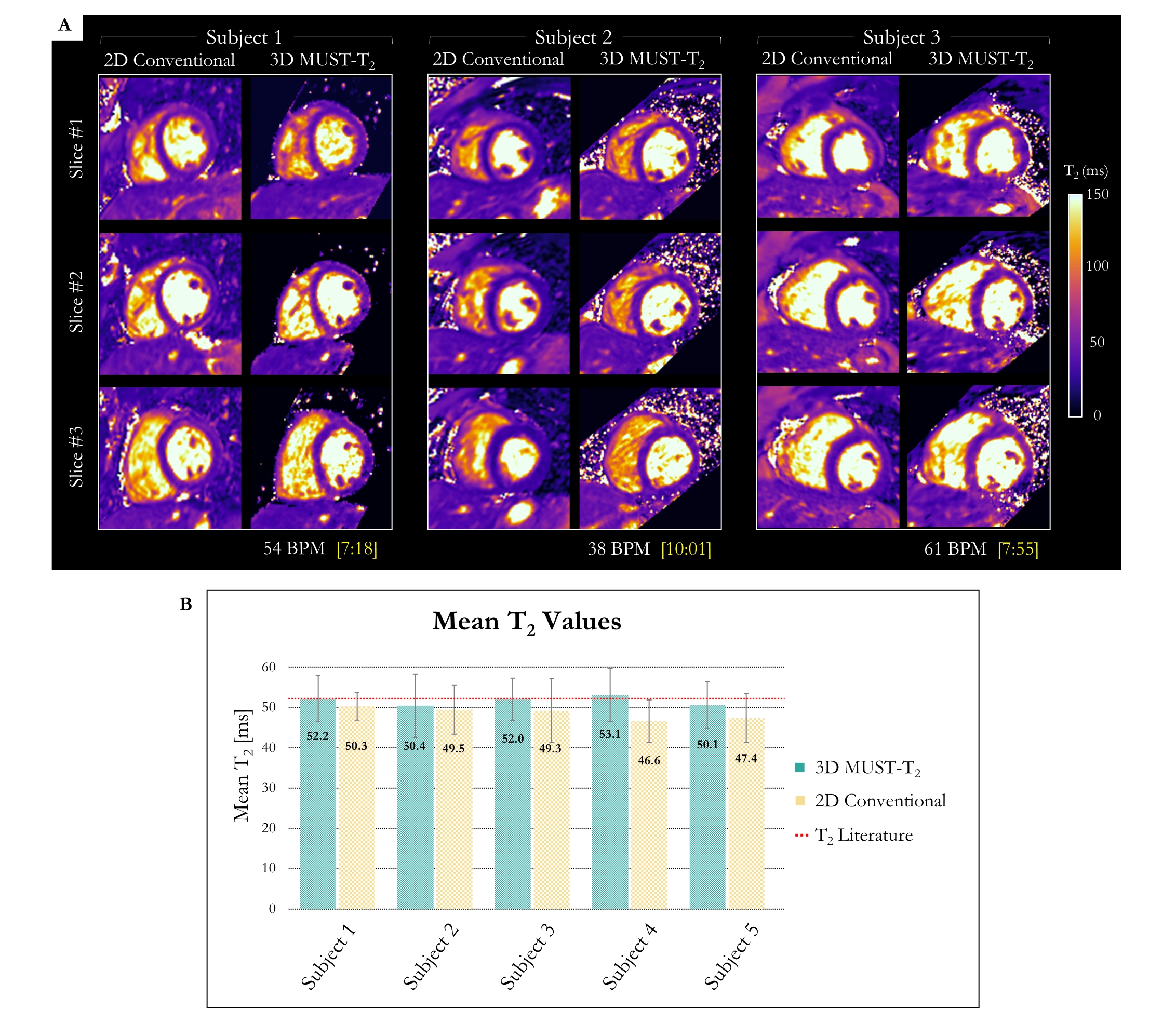
Phantom T2 values estimated with the proposed 3D MUST-T2 map were in excellent agreement with the ground truth T2 values (R2>0.995) even for high acceleration (5-fold), showing superior performance over the conventional 2D acquisition for high T2 values (Fig.2). 3D MUST-T2 short axis images and maps are shown in Fig.3 for a representative subject, showing homogenous T2 values over all slices. The isotropic nature of the proposed approach allows for reformatting in different orientations over the whole myocardium as shown in Fig. 4. 3D MUST-T2 maps of three other healthy subjects are shown in Figure 5a, showing excellent image quality. Mean T2 values are in good agreement with those obtained with conventional 2D T2 mapping (Figure 5b).Discussion
A novel approach was developed to enable free-breathing whole-heart 3D T2 mapping with high isotropic spatial resolution (1.5mm3) in a clinically feasible scan time (<8min with 100% respiratory scan efficiency). The proposed accelerated sequence combined with 3D-PROST reconstruction and dictionary matching achieved fast and accurate T2 quantification of myocardial tissue with excellent image quality in phantom and healthy subjects. Future studies will assess the clinical utility of MUST-T2 mapping in patients with myocardial inflammation.Acknowledgements
This work was supported by EPSRC (EP/L015226/1, EP/P001009, EP/P007619, EP/P032311/1) and Welcome EPSRC Centre for Medical Engineering (NS/ A000049/1).References
[1] Kim PK, Hong YJ, Im DJ, et al. Myocardial T1 and T2 mapping: techniques and clinical applications. Korean J Radiol. 2017;18(1):113-131.
[2] Ding H, Fernandez-de-Manuel L, Schar M, et al. Three-dimensional whole-heart T2 mapping at 3T. Magn Reson Med 2015;74:803-816.
[3] Bustin A, Ginami G, Cruz G, et al. Five-minute whole-heart coronary MRA with sub-millimeter isotropic resolution, 100% respiratory scan efficiency, and 3D-PROST reconstruction. Magn Reson Med 2018;1-14.
[4] Prieto C, Doneva M, Usman M, et al. Highly efficient respiratory motion compensated free-breathing coronary mra using golden-step Cartesian acquisition. J Magn Reson Imaging. 2015;41:738-746.
[5] Henningsson M, Koken P, Stehning C, et al. Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magn Reson Med. 2012;67:437-445
[6] Weigel M. Extended phase graphs: dephasing, RF pulses, and echoes – pure and simple. J. Magn. Reson. Imaging 2015;41:266-295.
[7] Captur G, Gatehouse P, Keenan KE, et al. A medical device-grade T1 and ECV phantom for global T1 mapping quality assurance - the T1 mapping and ECV standardization in cardiovascular magnetic resonance (T1MES) program. J. Cardiovasc. Magn. Reson 2016;18:1-20.
Figures