0400
Free Breathing Isotropic Cardiac Diffusion Tensor MRI of the Left Ventricle Using M2-gSlider: Unfolding the Fiber Architecture of the Human Heart1Department of Medicine, Harvard Medical School, Charlestown, MA, United States, 2Cardiovascular Research Center, Massachusetts General Hospital, Charlestown, MA, United States, 3Martinos Center for Biomedical Imaging, Massachusetts General Hospital, Charlestown, MA, United States, 4Department of Radiology, Harvard Medical School, Charlestown, MA, United States, 5Cardiovascular Institute, Rutgers Robert Wood Johnson Medical School, New Brunswick, NJ, United States, 6Department of Computer Science, University of São Paulo, São Paulo, Brazil
Synopsis
Free breathing isotropic cardiac diffusion tensor MRI (DT-MRI) of the entire left ventricle was achieved by combining two recently-developed technologies: second moment (M2) motion compensated spin echo encoding and generalized slice dithered enhanced resolution (gSlider). M2-gSlider can address cardiac motion-induced signal loss under free breathing and can achieve isotropic spatial resolution of 2.5 mm. With spatial resolution three times that of conventional cardiac DT-MRI, the precision of tractography-based indices can be improved. Furthermore, isotropic acquisition eases the interpretation of myocardial fiber architecture including in an “unfolded” representation, depicting both circumferential and longitudinal microstructure in a planar format.
INTRODUCTION
Despite inherent sensitivity to motion, in vivo cardiac diffusion Tensor MRI (DT-MRI) has now advanced to address motion-induced signal loss using second moment (M2) motion compensated spin echo diffusion encoding1-4. This M2 compensation permits the acquisition of cardiac DT-MRI while using an efficient 2D single shot EPI readout that allows for a free-breathing acquisition and subsequent retrospective motion correction (MOCO)3,5. Conventional 2D in vivo cardiac DT-MRI suffers from poor slice-axis resolution (~8 mm) relative to in-plane resolution (~2.5 mm), reducing the precision of quantitative tractography6,7 and potentially limiting the ability to capture longitudinal structure. To address this limitation, we propose the combination of M2 compensation with a recently developed RF encoded super-resolution framework using generalized slice dithered enhanced resolution (gSlider), which has demonstrated a significant increase in slice spatial resolution allowing for isotropic sub-millimeter imaging of the brain8. M2-gSlider achieves free breathing isotropic (~2.5 mm) DT-MRI acquisition of the entire left ventricle (LV), demonstrating a total increase of spatial resolution by a factor of 3. Isotropic resolution also improves analysis and visualization of fiber architecture in an “unfolded” representation, depicting both circumferential and longitudinal tissue microstructure.METHODS
Pulse Sequence Design:
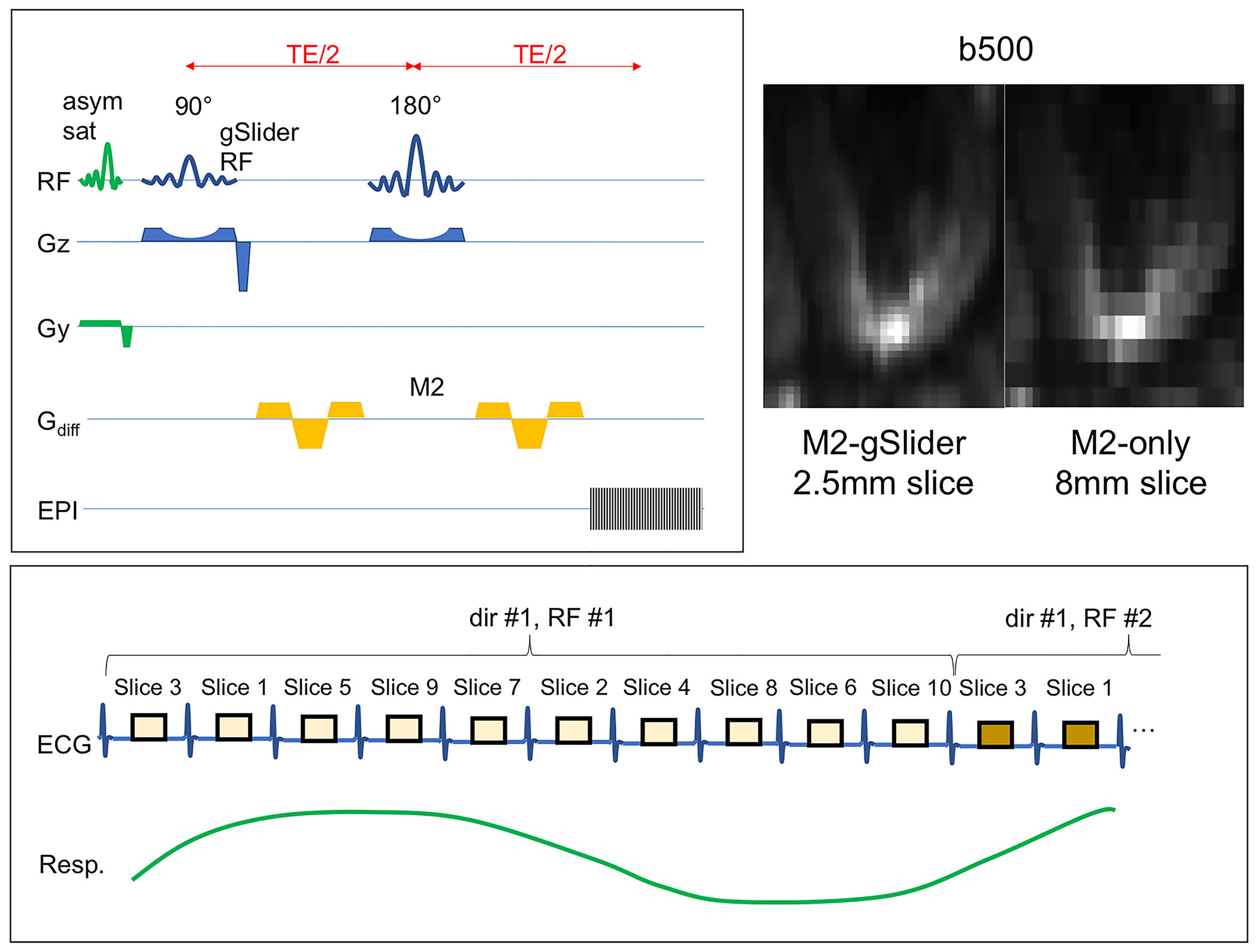
M2 compensation was achieved using a symmetric gradient encoding design optimized to reduce B1 sensitivity (Fig. 1). The gSlider RF and slice selective pulses were further optimized to significantly reduce RF duration, improve slice dither profile, and reduce SAR using a VERSE design9 for cardiac applications. Optimized slice interleaving was performed to ensure sufficient recovery (4 RR) occurred before adjacent slices were acquired. Asymmetric saturation bands were applied to mitigate any aliasing due to a zoomed single shot EPI acquisition. Zoomed EPI acquisition minimized readout duration (20 ms), reducing susceptibility distortion and echo time.
In Vivo Study:
Five healthy volunteers were scanned on a 3T scanner (Siemens Prisma) for 1.5 hours using M2-gSlider DT-MRI (TR = 10 RR, TE = 81 ms, in-plane resolution = 2.5 mm x 2.5 mm, slice thickness = 2.5 mm [RF slab thickness = 12.5 mm, gSlider factor = 5], outer volume suppression with asymmetric saturation bands, 1 b = 0 and 10 b = 500 s/mm2 diffusion directions, 10 averages) under free breathing conditions covering the entire LV. A purpose-built 64-channel cardiac phased-array coil was used for all acquisitions.
Image Analysis:
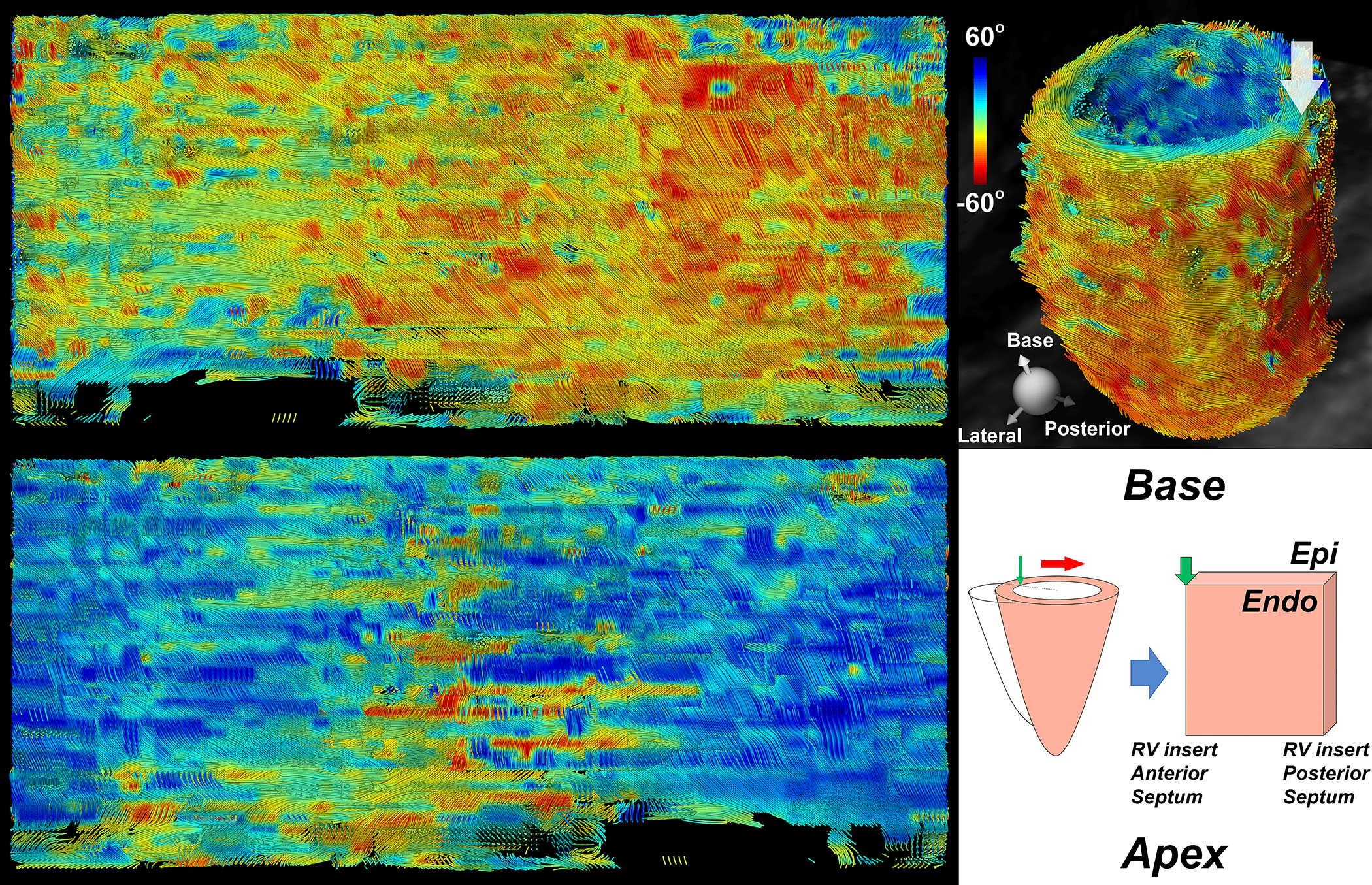
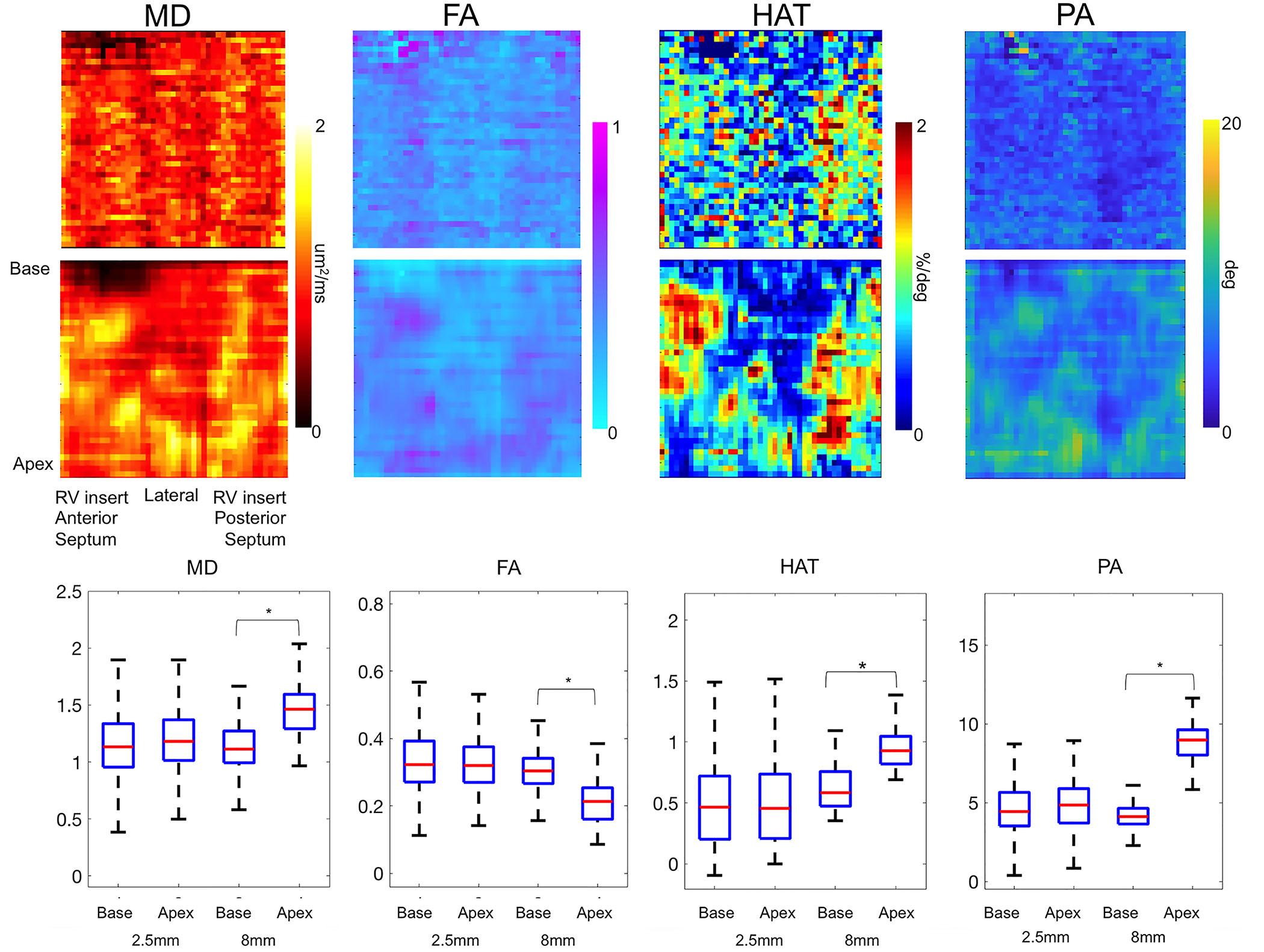
Diffusion-based indices including mean diffusivity (MD), fractional anisotropy (FA), helix angle (HA), helix angle transmurality (HAT), and tractographic propagation angle (PA) were computed at both isotropic and resampled conventional resolution (2.5 x 2.5 x 8 mm). An unfolded representation of the LV wall was generated by projecting 90 radial scanlines10 4 degrees apart, from the center at the LV cavity, at each level from apex to base, using the anterior LV-RV junction as the starting point of unfolding. The unfolded tensor field within the resulting slab was then corrected for the geometrical transformation. The diffusion-based indices were mapped onto this unfolded representation and averaged across transmural depth. Values of MD, FA, HAT, and PA derived from conventional and isotropic resolutions in all subjects were compared using the Wilcoxon-signed rank test. A comparison of tractography using a 4th order Runge-Kutta approach11 based on conventional and isotropic data was performed to assess the effect of artifact due to partial volume averaging.
RESULTS
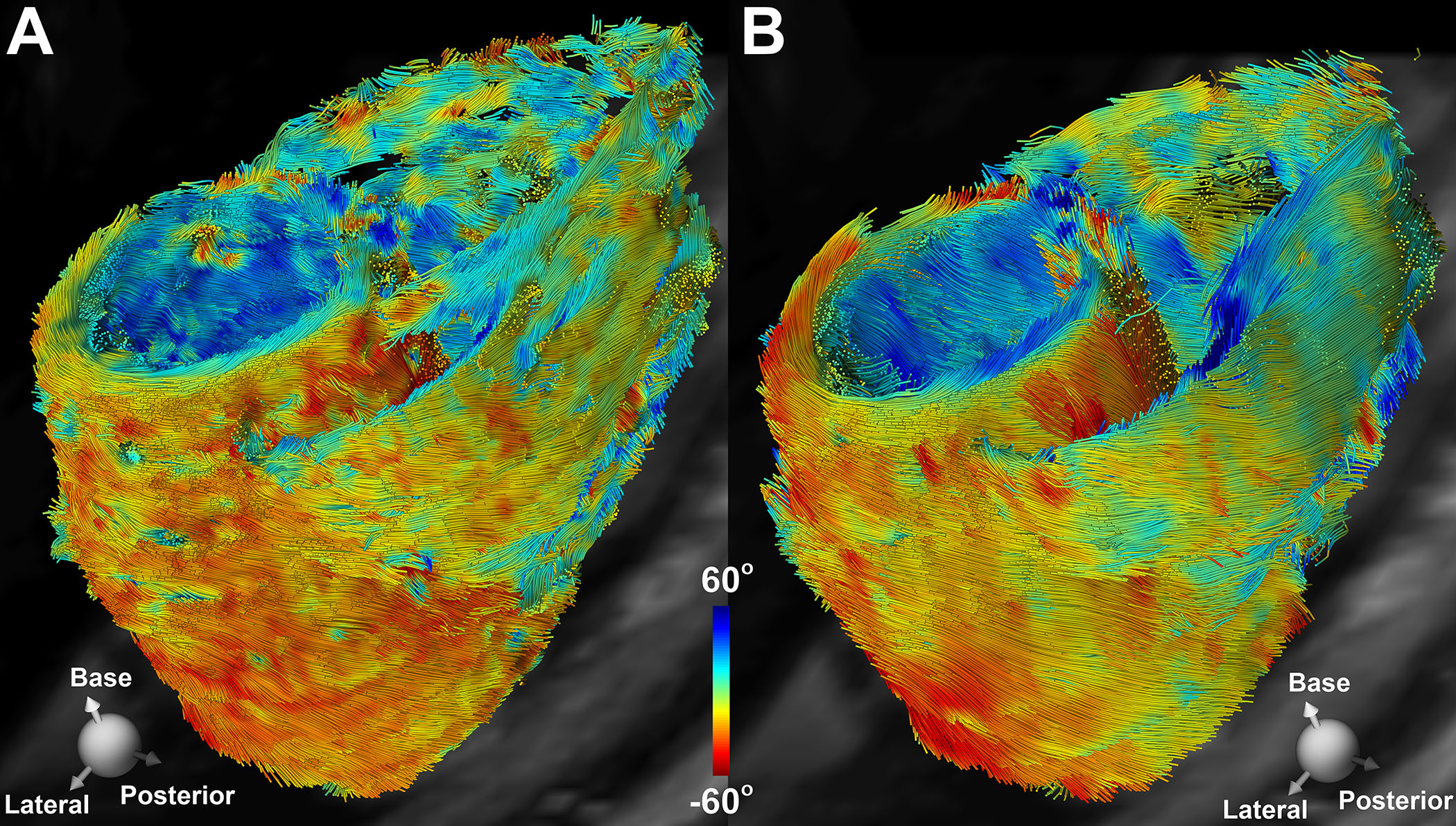
As compared to conventional anisotropic acquisition, tractography derived from M2-gSlider DT-MRI isotropically-acquired data was able to capture more of the local variability in the 3D myofiber continuum (e.g. as seen in the anterolateral wall in Fig. 2). Using M2-gSlider (2.5 mm isotropic resolution), there were no significant differences between basal (MD=1.1±0.3 μm2/ms, FA=0.34±0.1, HAT=0.48±0.4 deg/%, and PA=4.7±2 deg) and apical (MD=1.2±0.3 μm2/ms, FA = 0.33±0.08, HAT=0.49±0.4 deg/%, and PA=4.8±2 deg) left ventricular regions (Figs. 3 and 4). In contrast, there were significant differences in all cardiac DT-MRI indices derived from conventional DT-MRI (2.5 x 2.5 x 8.0 mm) between basal (MD=1.1±0.2 μm2/ms, FA=0.31±0.06, HAT=0.62±0.2 deg/%, and PA=4.2± 0.8 deg) and apical (MD=1.4±0.3 μm2/ms, FA=0.20±0.1, HAT=0.94±0.2 deg/%, and PA=8.7±2 deg) LV regions.CONCLUSION
Acquisition of the entire left ventricle with isotropic resolution was accomplished using M2-gSlider cardiac DT-MRI. This method increases spatial resolution by a factor of 3 over conventional cardiac DT-MRI techniques. The ability to acquire truly isotropic data improves analysis and visualization of myofiber architecture by reducing diffusion index spatial variability from base to apex, as demonstrated in this study. Future work will include improvement and acceleration of the M2-gSlider cardiac DT-MRI method and will extend its use to the study of patients with variety of cardiomyopathies.Acknowledgements
NIH R01HL131635
NIH R21EB024701
References
1. Stoeck, C. T., Deuster, von, C., Genet, M., Atkinson, D. & Kozerke, S. Second-order motion-compensated spin echo diffusion tensor imaging of the human heart. Magn. Reson. Med. 75, 1669–1676 (2016).
2. Nguyen, C. et al. In vivo three-dimensional high resolution cardiac diffusion-weighted MRI: a motion compensated diffusion-prepared balanced steady-state free precession approach. Magn. Reson. Med. 72, 1257–1267 (2014).
3. Nguyen, C. et al. In vivo diffusion‐tensor MRI of the human heart on a 3 tesla clinical scanner: An optimized second order (M2) motion compensated diffusion‐preparation approach. Magn. Reson. Med. (2016). doi:10.1002/mrm.26380
4. Aliotta, E., Wu, H. H. & Ennis, D. B. Convex optimized diffusion encoding (CODE) gradient waveforms for minimum echo time and bulk motion-compensated diffusion-weighted MRI. Magn. Reson. Med. 77, n/a–n/a (2016).
5. Moulin, K. et al. In vivo free-breathing DTI and IVIM of the whole human heart using a real-time slice-followed SE-EPI navigator-based sequence: A reproducibility study in healthy volunteers. Magn. Reson. Med. 76, 70–82 (2015).
6. Mekkaoui, C., Reese, T. G., Jackowski, M. P., Bhat, H. & Sosnovik, D. E. Diffusion MRI in the heart. NMR Biomed. n/a–n/a (2015). doi:10.1002/nbm.3426
7. Mekkaoui, C. et al. Diffusion Tractography of the Entire Left Ventricle by Using Free-breathing Accelerated Simultaneous Multisection Imaging. Radiology 282, 850–856 (2017).
8. Setsompop, K. et al. High‐resolution in vivo diffusion imaging of the human brain with generalized slice dithered enhanced resolution: Simultaneous multislice (gSlider‐SMS). Magn. Reson. Med. 57, 167 (2017).
9. Hargreaves, B. A., Nishimura, D. G. & Conolly, S. M. Time-optimal multidimensional gradient waveform design for rapid imaging. Magn. Reson. Med. 51, 81–92 (2003).
10. Mekkaoui, C., et al. J Cardiovasc Magn Reson. 2013;15(Suppl 1):O81. Published 2013 Jan 30. doi:10.1186/1532-429X-15-S1-O81
11. Mekkaoui, C. et al. Fiber architecture in remodeled myocardium revealed with a quantitative diffusion CMR tractography framework and histological validation. Journal of Cardiovascular Magnetic Resonance 14, 70 (2012).
Figures