0395
Evaluation of Fractional Tumor Burden (FTB) fidelity using a no-preload, low-flip angle dynamic susceptibility contrast MRI acquisition scheme1Biophysics, Medical College of Wisconsin, Milwaukee, WI, United States, 2Radiology, Mayo Clinic Arizona, Phoenix, AZ, United States, 3Diagnostic Imaging, Rhode Island Hospital, Providence, RI, United States, 4Imaging Research, Barrow Neurological Institute, Phoenix, AZ, United States, 5Neurology, Medical College of Wisconsin, Milwaukee, WI, United States, 6Radiology, Medical College of Wisconsin, Milwaukee, WI, United States
Synopsis
This study examines the fidelity of a no pre-load, low flip-angle (LFA) dynamic susceptibility contrast MRI acquisition approach in the calculation of Fractional Tumor Burden (FTB) maps, which have shown promise as a predictive biomarker in glioblastoma patients. The LFA approach was recently identified as providing similar accuracy to the standard mid-range flip-angle approach with preload. FTB was found to have robust quantitative and spatial agreement between LFA and MFA approaches. The results of this study bode well for increased adoption of FTB as a biomarker amenable to both the standard and newer LFA approach.
Introduction
Fractional tumor burden (FTB), a recent biomarker derived from DSC-MRI relative cerebral blood volume (rCBV), allows spatial and quantifiable distinction of tumor from treatment effect.1,2 FTB correlates with both progression free and overall survival in patients with GBM following treatment with either upfront chemo-radiation or bevacizumab at recurrence.3,4 However, it is unknown if FTB will perform similarly for various DSC-MRI acquisition and contrast agent dosing schemes. Recently, using a digital reference object of DSC-MRI in GBM,5 it was shown that in addition to post-processing leakage correction,6,7 the best approach for collecting DSC uses both a single-dose contrast agent (CA) preload and single-dose CA bolus with a mid-range flip angle (MFA) (Preload+Bolus, FA=60°, TE=30ms) to be the most accurate for rCBV map generation.5,8 This is the approach used for the original validation of FTB.1-4 Interestingly, similar accuracy was also identified for data collected without a preload of CA when using a low flip-angle (LFA) approach (Bolus, FA=30°, TE=30ms) as long as leakage correction was also used.8,9 The goal of this study was to evaluate the fidelity of FTB when DSC is acquired with a LFA and single-dose of CA.Methods
Informed, written consent was obtained for all participants in this multi-center HIPAA-compliant and IRB-approved study. All 38 participants had a glial tumor and two DSC-MRI exams acquired during the same scanning session. The first LFA DSC-MRI was collected during the first loading bolus of CA. The second MFA DSC-MRI was acquired during a second single-dose bolus of CA. The CA injected during the first DSC exam served as the pre-load for the second exam. Both normalized (to NAWM) (nRCBV) and standardized10, 11 (using FDA-approved software) (sRCBV) rCBV maps were created for each DSC-MRI acquisition. All images were co-registered to T1+C. Lesion ROIs were delineated with quantitative deltaT1 maps,12, 13 where standardized T1 is subtracted from standardized T1+C. FTB maps were created by thresholding the rCBV maps within the lesion ROI. FTB was quantified as the fraction of tumor voxels relative to the entire lesion. Sørensen–Dice coefficients were calculated for each subject to assess spatial agreement. Lin’s concordance correlation coefficient and linear regression were performed to assess quantitative agreement between FTB maps for the two DSC acquisition schemes.Results
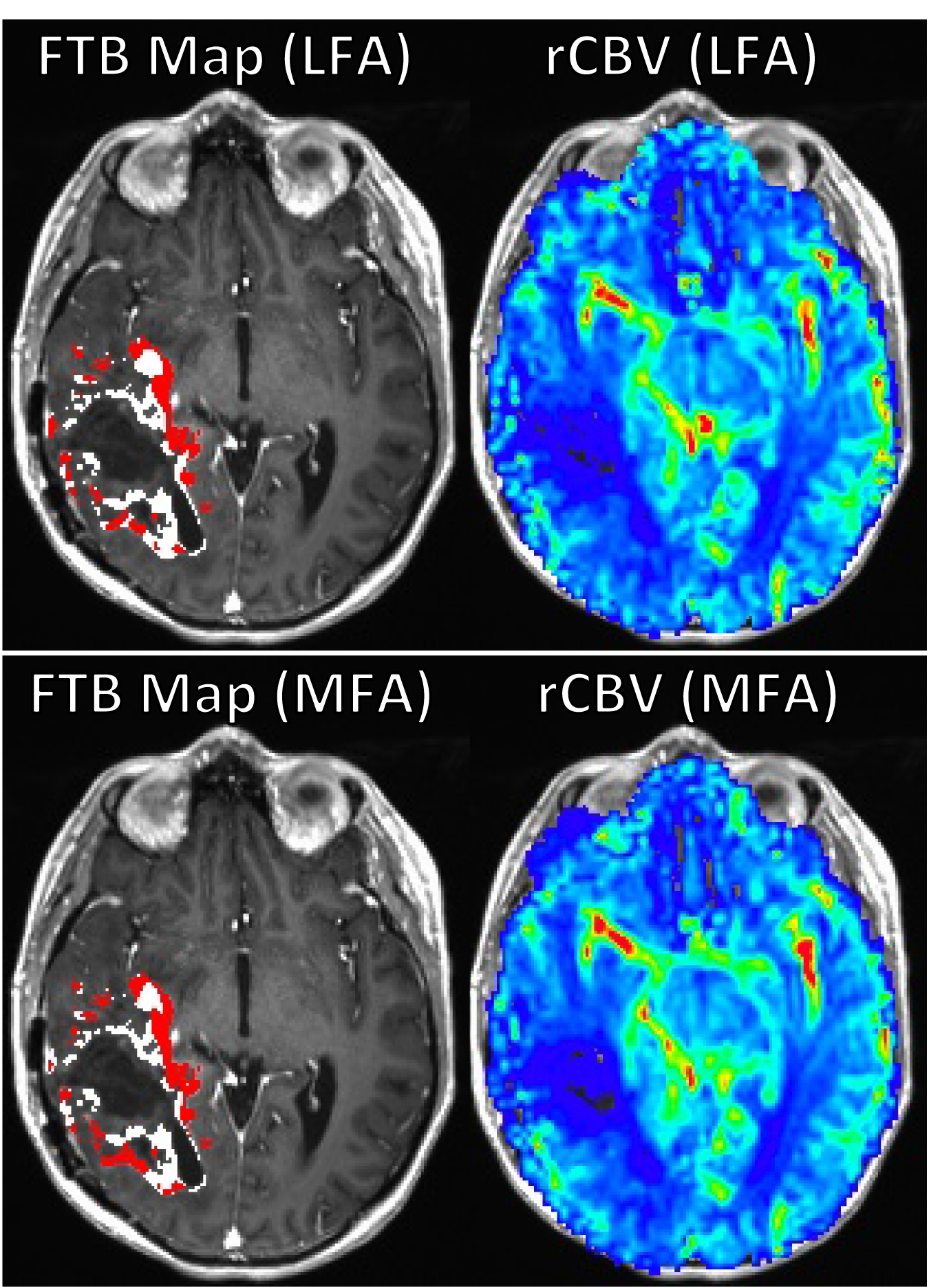
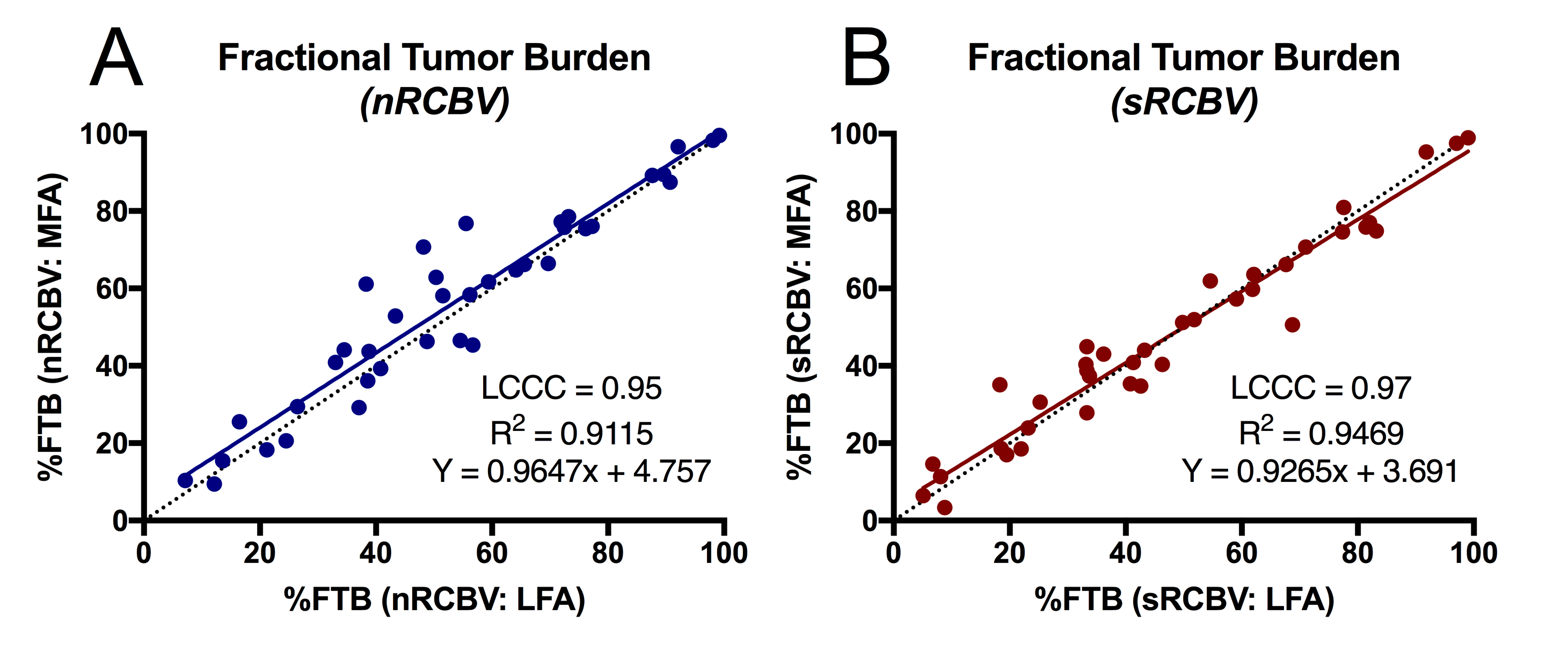
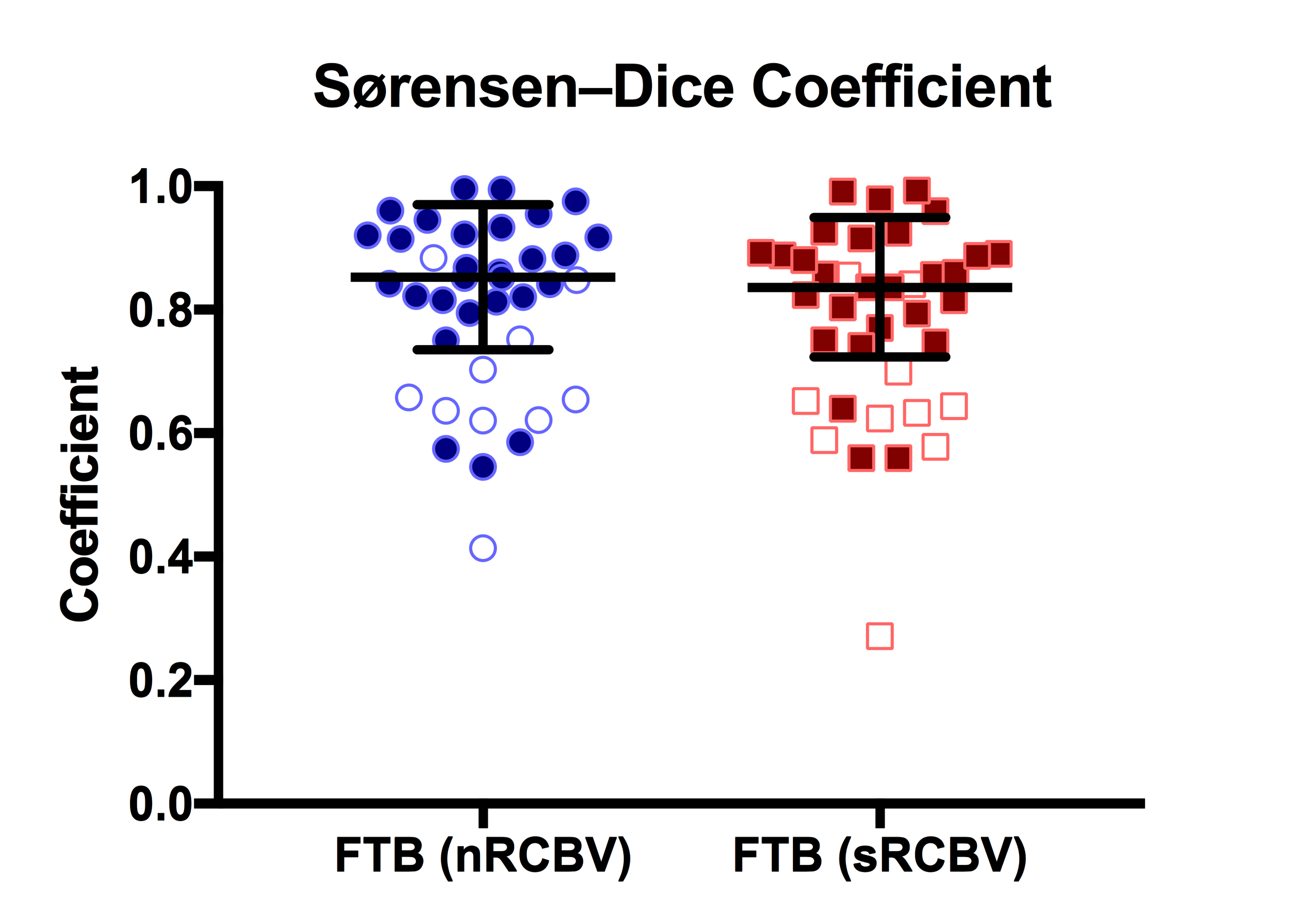
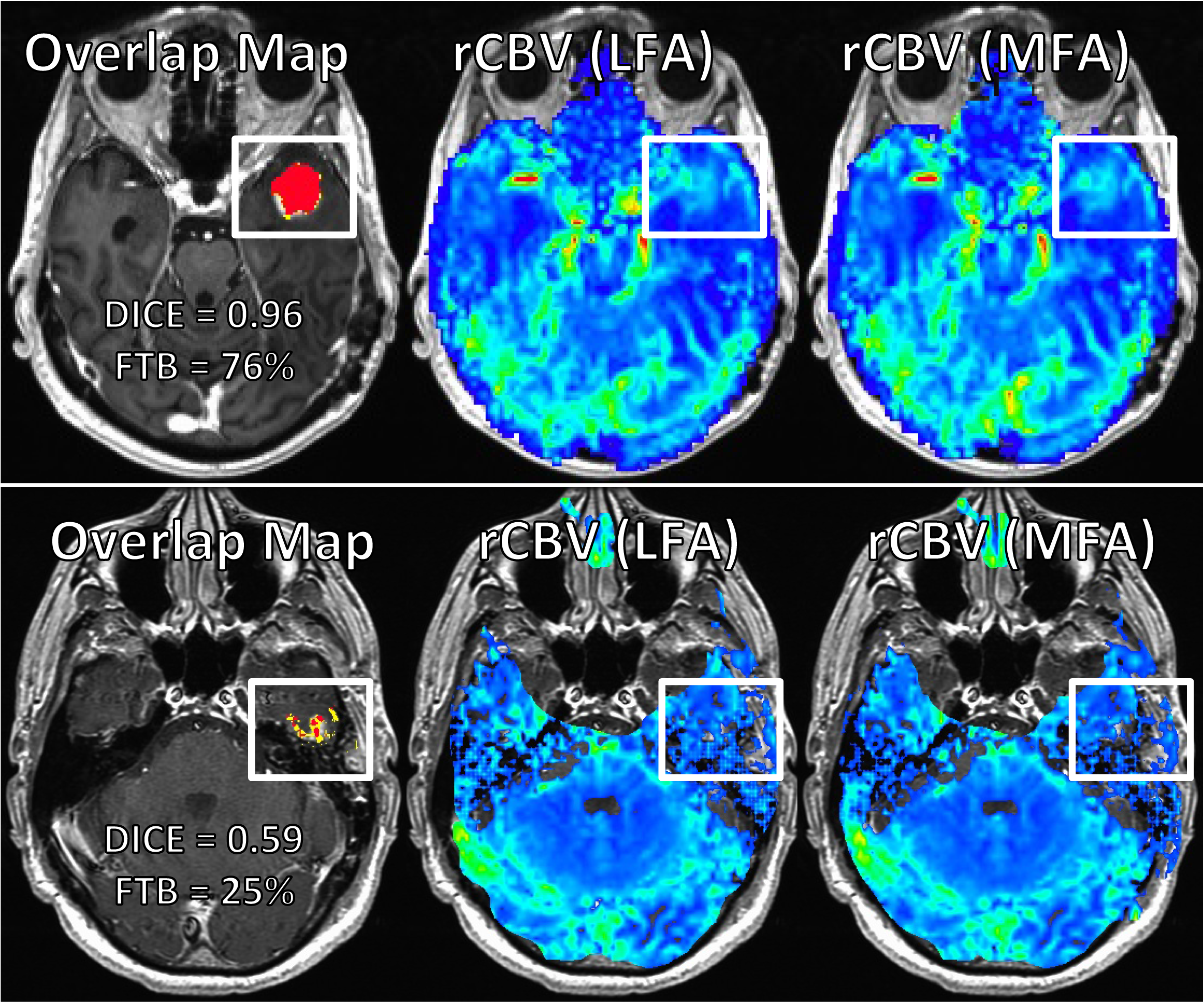
Example FTB and rCBV maps are shown in Figure 1 for both LFA and MFA DSC acquisitions. Regression analysis and LCCC showed excellent agreement (Figure 2) between LFA and MFA methods for both nRCBV (LCCC=0.95; R2=0.91) and sRCBV (LCCC=0.97; R2=0.95). Dice coefficients showed good agreement for nRCBV (mean=0.852, range=0.546-0.996) and sRCBV (mean=0.836, range=0.560-0.994) among FTB regions when FTB volume was of measureable disease (>1cc) (Figure 3). In subjects where the volume of tumor burden was <1cc, Dice coefficients were noticeably worse for both nRCBV (mean=0.680, range=0.414-0.885) and sRCBV (mean=0.640, range=0.272-0.856). Example overlap and corresponding rCBV maps are displayed in Figure 4 for a subject with good agreement and a subject with poor agreement.Discussion
FTB appears to be a robust biomarker that is translatable for use with a LFA acquisition scheme, as results show excellent agreement quantitatively and good agreement spatially. Poor agreement was observed in areas where the DSC-MRI signal is poor as displayed in Figure 4, and when the volume of tumor burden was <1cc. Unlike the MFA approach, a limitation to the LFA approach is that it might also be more prone to diminished areas of CNR, such as can occur near the edge of active tumor.Conclusion
The results of this study show that a single-dose LFA DSC-MRI acquisition provides comparable fidelity, which in turn may increase confidence in the adoption of FTB as a biomarker that is more accessible to institutions that prefer to limit CA dosing. Furthermore, this study may increase confidence in the use of the lower dose LFA approach as an acceptable alternative to the MFA approach, which requires delivery of additional CA.Acknowledgements
Funding support was provided by NIH/NCI R01 CA082500 and NIH/NCI U01 CA176110.References
1. Hu, L.S., et al., Reevaluating the imaging definition of tumor progression: perfusion MRI quantifies recurrent glioblastoma tumor fraction, pseudoprogression, and radiation necrosis to predict survival. Neuro Oncol, 2012. 14(7): p. 919-30.
2. Prah, M.A., et al., Spatial discrimination of glioblastoma and treatment effect with histologically-validated perfusion and diffusion magnetic resonance imaging metrics. J Neurooncol, 2018. 136(1): p. 13-21.
3. Prah M.A., et al., “MRI-perfusion derived Fractional Tumor Burden (FTB) stratifies survival in recurrent glioblastoma following treatment with bevacizumab.” 25th Annual Meeting of the International Society of Magnetic Resonance in Medicine (ISMRM), Honolulu, HI (2017) p 707.
4. Prah M.A., Connelly J.M., and Schmainda K.M. “MRI-perfusion derived Fractional Tumor Burden (FTB) is predictive of overall and progression free s survival in newly diagnosed glioblastoma following concomitant chemoradiotherapy.” 25th Annual Meeting of the International Society of Magnetic Resonance in Medicine (ISMRM), Honolulu, HI (2017) p 708.
5. Semmineh, N.B., et al., A Population-Based Digital Reference Object (DRO) for Optimizing Dynamic Susceptibility Contrast (DSC)-MRI Methods for Clinical Trials. Tomography, 2017. 3(1): p. 41-49.
6. Paulson, E.S. and K.M. Schmainda, Comparison of dynamic susceptibility-weighted contrast-enhanced MR methods: recommendations for measuring relative cerebral blood volume in brain tumors. Radiology, 2008. 249(2): p. 601-13.
7. Boxerman, J.L., et al., The Role of preload and leakage correction in gadolinium-based cerebral blood volume estimation determined by comparison with MION as a criterion standard. AJNR Am J Neuroradiol, 2012. 33(6): p. 1081-7.
8. Schmainda, K.M., et al., Moving Towards A DSC-MRI Consensus: A new single dose option for standardized rCBV. 26th
Annual Meeting of the International Society of Magnetic Resonance in Medicine
(ISMRM), Paris, France (2018).
9. Boxerman J, et al., A comparison of low flip-angle, no-preload DSC-MRI to intermediate flip-angle, preload-based DSC-MRI as a reference standard. In: Proceedings of the ASNR 56th Annual Meeting, June 2-7, 2018, Vancouver, BC, CAN.
10. Bedekar, D., T. Jensen, and K.M. Schmainda, Standardization of relative cerebral blood volume (rCBV) image maps for ease of both inter- and intrapatient comparisons. Magn Reson Med, 2010. 64(3): p. 907-13.
11. Prah, M.A., et al., Repeatability of Standardized and Normalized Relative CBV in Patients with Newly Diagnosed Glioblastoma. AJNR Am J Neuroradiol, 2015. 36(9): p. 1654-61.
12. Schmainda, K.M., et al., Dynamic susceptibility contrast MRI measures of relative cerebral blood volume as a prognostic marker for overall survival in recurrent glioblastoma: results from the ACRIN 6677/RTOG 0625 multicenter trial. Neuro Oncol, 2015. 17(8): p. 1148-56.
13. Bedekar, D., et al. Delta T1 Method: An Automatic Post-Contrast ROI Selection Technique for Brain Tumors. in In: Proceedings of the Eighteenth Meeting of the International Society for Magnetic Resonance in Medicine #2175. 2010. Stockholm, Sweden: Curran Associates, Inc.
Figures