0389
A 24-channel head and spine array for 3T pediatric MRI under 3-year-old1Lauterbur Imaging Research Center,Shenzhen Institutes of Advanced Technology, Chinese Academy of Sciences, Shenzhen, China, 2Shenzhen Key Laboratory for MRI, Shenzhen, China, 3Shanghai United Imaging, Shanghai, China, 4Department of Radiology, Xinhua Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China, 5Department of Radiology and Biomedical Imaging, University of California San Francisco, San Francisco, CA, United States, 6UCSF/UC Berkeley Joint Graduate Group in Bioengineering, San Francisco, CA, United States
Synopsis
Pediatric MRI is an important tool for clinical diagnosis and research. It demands high spatial resolution and short scan time to increase success rates. To obtain high resolution images within resonable scan time, a dedicated 24-channel head and spine coil array was designed and fabricated for patient under 3-year-old in this work. Compared to a commercial 24-channel head and neck adult coil, the proposed coil offers higher resolution, image quality and shorter scan time in patient studies.
Introduction
Methods
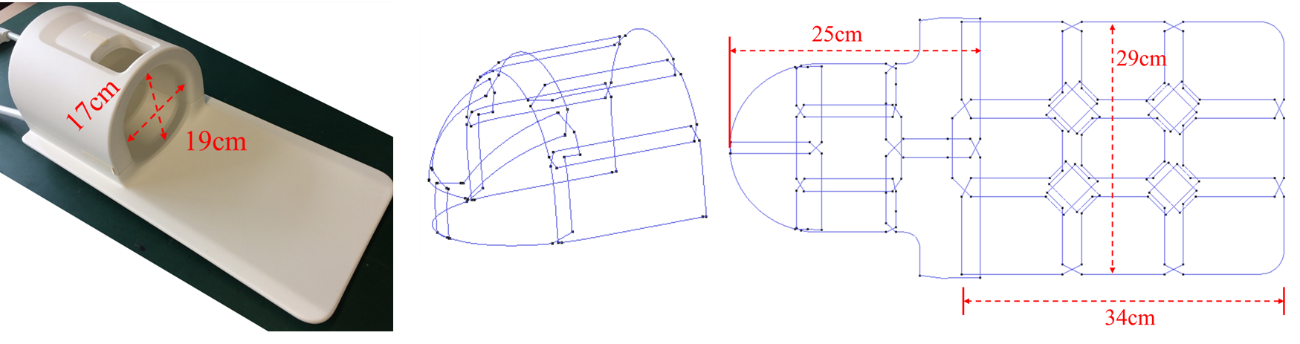
The dimensions of the proposed 24-channel pediactric coil were designed according to the measure of 3-year-old children [5]. The inner dimensions of the head part were 19 cm in the Antero-Posterior (AP) direction, 17 cm in the Left-Right (LR) direction, and 20 cm in the Inferior-Superior (IS) direction. The spine part was of 29 cm in width and 34 cm in length. The coil consisted of 13 elements for brain imaging, 2 elements for neck imaging and 9 elements for body imaging as shown in Figure 1. All the elements was tuned to 128.23 MHz and matched to 50 Ohm. The adjacent elements were decoupled by overlapping and low impedance preamplifiers were employed for non-adjacent element decoupling. Phantom and in-vivo studies were carried out on a 3T MRI system (uMR 770, Shanghai United Imaging Healthcare, Shanghai, China). The phantom consisted of saline with 2.6 g/L NaCl and 1.234 g/L NiSO4﹒6H2O. The coronal and sagittal images were acquired with a 2D GRE sequence (TR/TE=300 ms/15 ms, flip angle=90o, FOV= 200 x 200 mm2, slice thickness=5 mm, Matrix size=256 x 256), Noise scan was performed by setting the transmit power to zero. The SNR was computed and compared with the commercial 24-channel adult head-neck coil. For in-vivo pediatric imaging, more than 20 patients from 4-month to 3-year-old have been scanned using the proposed coil. High spatial resolution brain images of two patients were acquired by using a 3D T1-weighted fat-saturation contrast-enhancement gradient echo sequence with the parameters as following: TR/TE= 7.6/3.34 ms, flip angle=10o, FOV= 180 × 180 mm, acceleration rate = 2, bandwidth= 250 Hz/pixel. The acquisition matrix and image resolution of the proposed coil were 544 × 544 and 0.33 × 0. 33 × 0.4 mm respectively, while those of the adult coil were 480 × 480 and 0.375 × 0.375 × 0.4 mm respectively. The numbers of average of the proposed coil and adult coil are 3 and 4 respectively. Therefore, total acquisition time of proposed coil is 3 minutes and 32 seconds while that of the adult coil is 5 minutes.Results
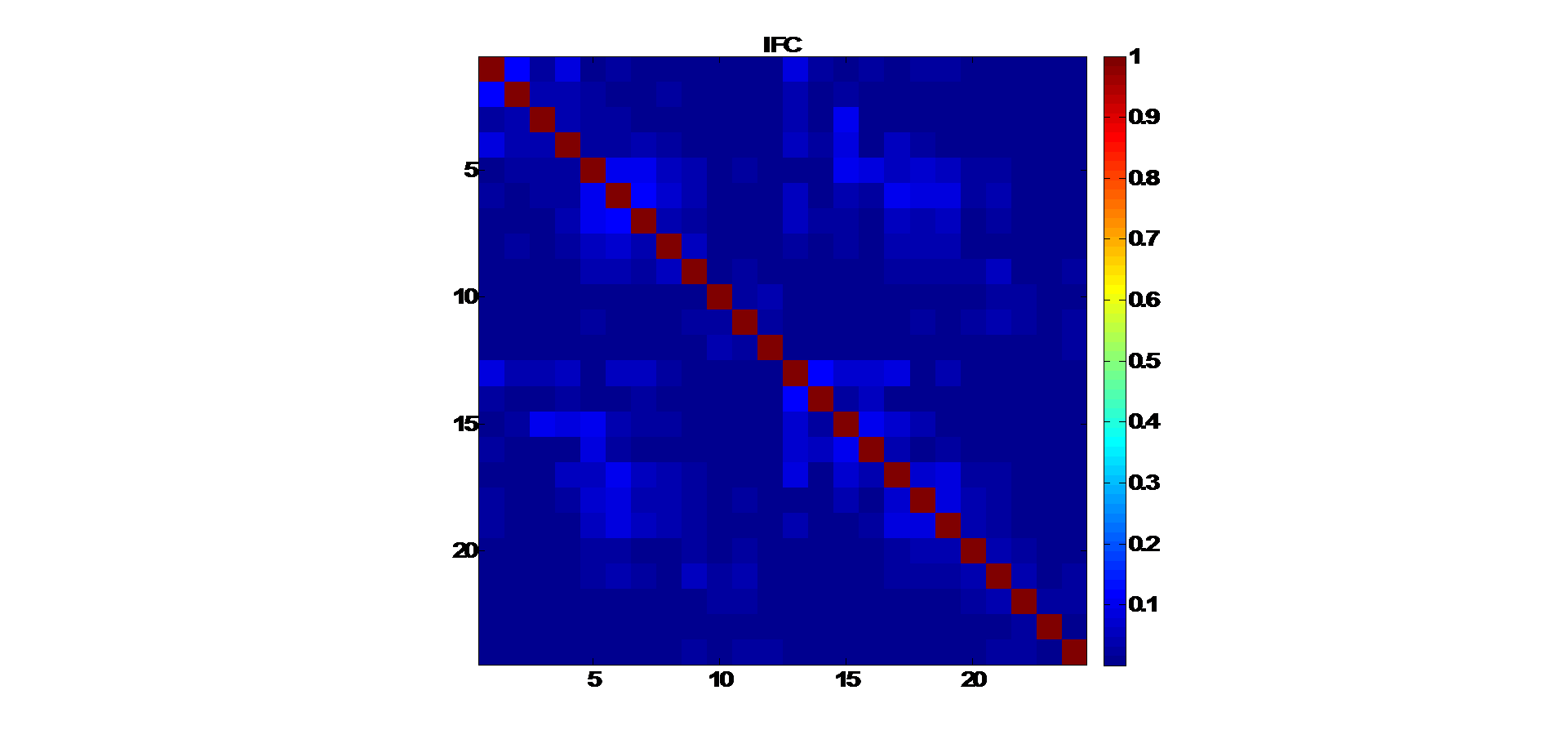
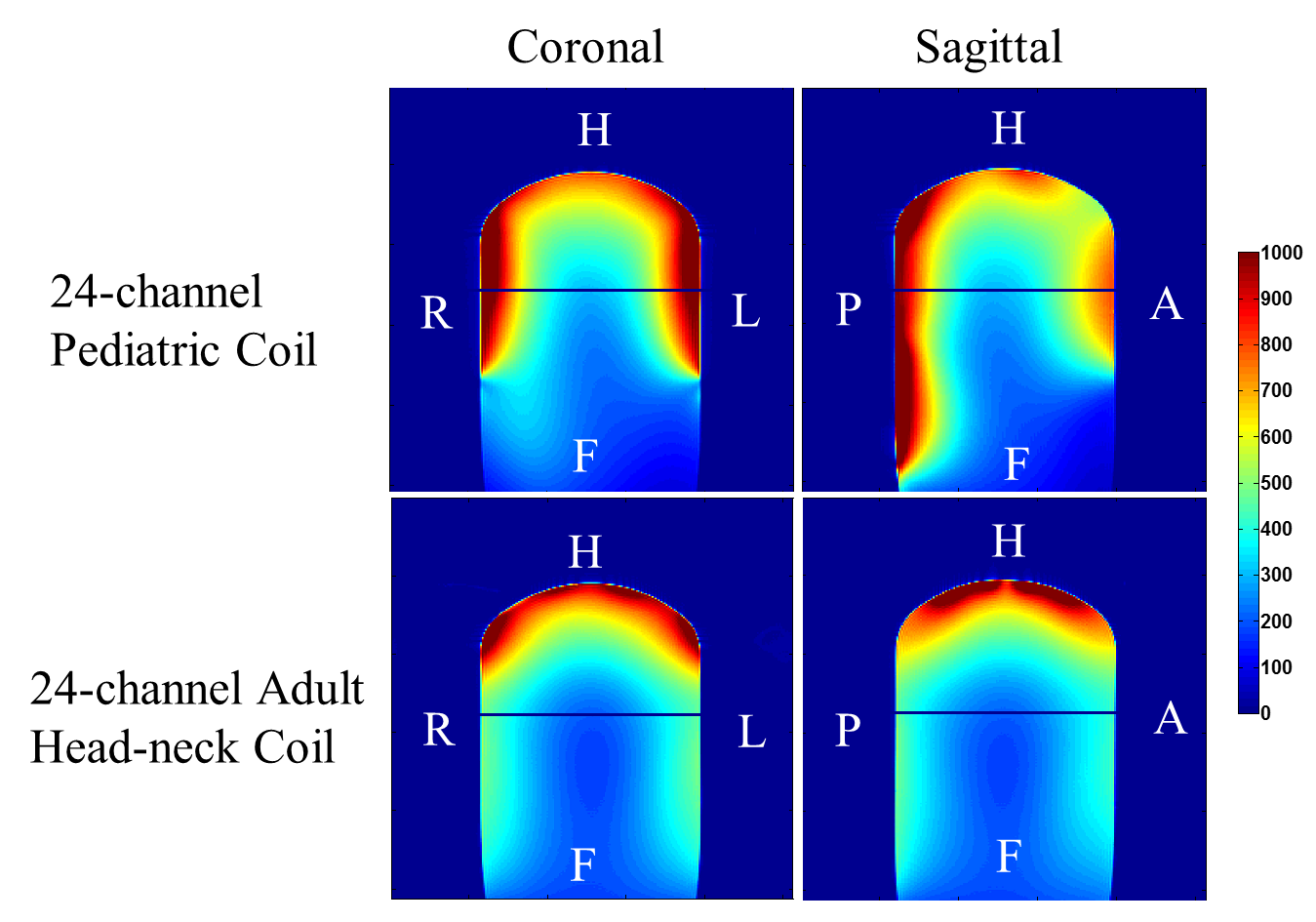
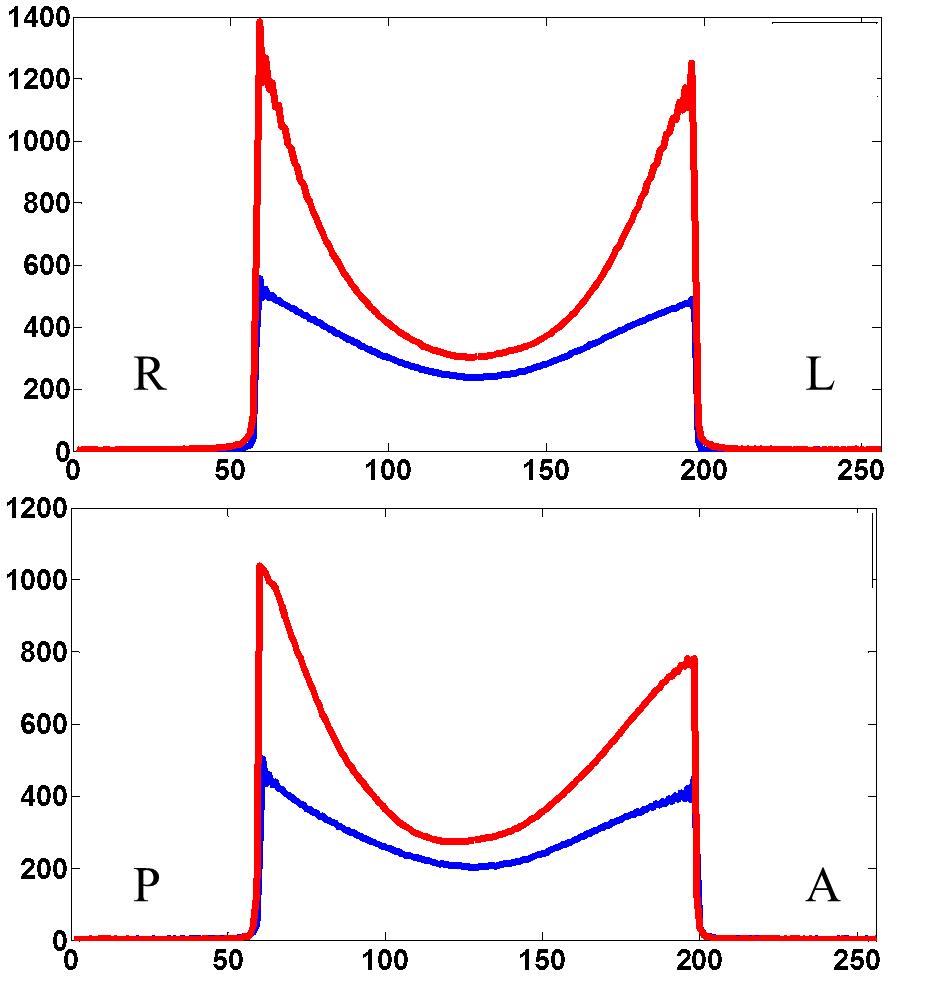
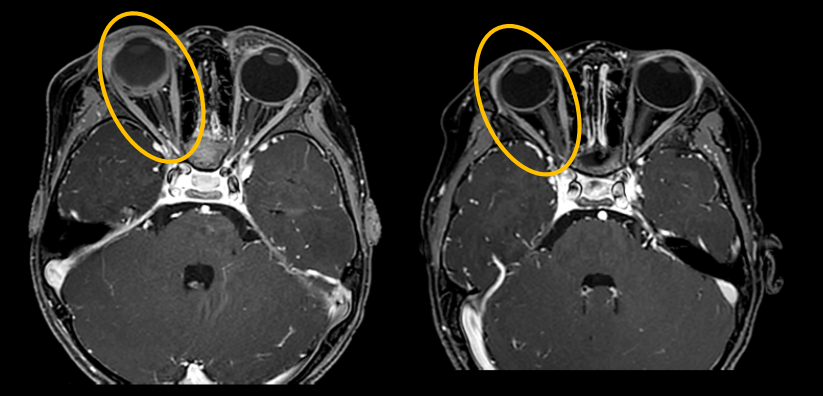
Fig. 2 shows the noise covariance matrix of the proposed 24-channel array. The mean and maximum of non-diagonal elements are 0.02 and 0.14 respectively, which demonstrates good decoupling condition among each coil element. SNR improvement was obvious in the brain regions, which was at least 42 %. The SNR maps of the two coils in the coronal and sagittal planes are shown in figure 3. The SNR of the 24-channel pediatric coil provides higher SNR compared with the adult head-neck coil. Fig. 4 depicts the 1D profiles in the Right/Left (R/L) and Anterior/Posterior (A/P) directions. The red and blue lines denote the proposed pediatric coil and adult coil respectively. The SNR gain is more than 2-fold in the surface region and 20% in the center of the phantom by using the proposed coil. Fig. 5 shows the contrast-enhancement brain images of two patients acquired by 3D T1-weighted gradient echo sequence with fat-saturation. The proposed coil offers higher resolution and imaging speed. The images demonstrate the shapes of the tumor and the optic nerve as well as whether the optic nerve is enhanced. These information is critical for the follow-up treatment plan.Conclusion
A 24-channel head and spine pediatric coil was designed, constructed and evaluated by phantom and in-vivo experiments. Compared with a commercially available 24-channel head and neck adult coil, the proposed coil provides higher resolution in shorter scan time in pediatric brain studies, which will benefit clinical diagnosis and success rates. The proposed coil could be potentially used together with a flexible torso array for body imaging.
Acknowledgements
This work was supported in part by NSFC under Grant No. 61571433, 61801466, 81627901, 81527901; Grant No. 2016YFC0100301; Guangdong Province grants 2014A030312006, and 2014B030301013; Youth Innovation Promotion Association of CAS No. 2017415; city grants JCYJ20170413161314734; NIH U01EB023829, and a Pengcheng Scholar Award.References
1. A. E. Finnemore, A. N. Price, et al. “Impact of neonatal cardiac receive-array coil on SNR and CNR in newborn infants,” Journal of Cardiovascular Magnetic Resonance, vol.13, pp.215, 2011.
2. M. Helle, M. Jerosch-Herold, et al. “Improved MRI of the neonatal heart: feasibility study using a knee coil,” Pediatr Radiol, vol.41, pp.1429-1432, 2011.
3. E. J. Hughes, T. Winchman, et al. “A Dedicated Neonatal Brain Imaging System,” Magnetic resonance in medicine, vol.78, no.2, pp.794-804, 2017.
4. B. Keil, V. Alagappan, et al. “Size-optimized 32-Channel Brain Arrays for 3T Pediatric Imaging,” Magnetic resonance in medicine, vol.66, pp. 1777-1787, 2011.
5. Alvin R. Tilley, and Henry Dreyfuss Associates. The Measure of Man and Woman: Human Factors in Design (Revised Edition), John Wiley and Son Inc., 2001.
Figures