0386
Long half-life of propylene glycol in neonatal brain: an MRS study1Radiology and Nuclear Medicine, Amsterdam UMC, Location VUMC, Amsterdam, Netherlands, 2Pediatrics / Neonatology, Amsterdam UMC, Location VUMC, Amsterdam, Netherlands, 3Child Neurology, Amsterdam UMC, Location VUMC, Amsterdam, Netherlands, 4Pharmacy, Erasmus MC - Sophia Children's Hospital, Rotterdam, Netherlands
Synopsis
Neonatal convulsions are preferably treated with intravenous phenobarbital that contains propylene glycol (PG) as solvent. Very high concentrations of brain PG have been observed with quantitative MRS, especially when low-concentrated phenobarbital medication was used. PG can have serious adverse effects, and the half-life is longer in neonates than in adults. Based on given medication and the interval until MRS examination we estimated a PG half-life in neonatal brain that is at least 30 hours and maybe up to 43 hours. This shows that extremely high and potentially toxic PG concentrations will persist longer than expected in the neonatal brain.
Introduction
Neonatal convulsions are preferably treated with intravenous phenobarbital. This medication contains propylene glycol (PG) as solvent. Typical clinical doses exceed recommended safety thresholds, although serious short-term adverse effects of PG have been described.1,2 Depending on the pharmaceutical formulation of phenobarbital, and on the interval between administration and MRS examination, very high concentrations of PG in neonatal brain have been detected.3 PG is eliminated through the kidneys or metabolized in the liver, but due to lower metabolic hepatic capacity and immature renal function, the half-life is longer in neonates than in adults. In a small group of neonates, mostly preterm-born and with very low birth weight, receiving a multivitamin preparation with high doses of PG, a mean plasma PG half-life of 19.3 h was estimated (range 10.8-30.5 h).4 The aim of the current study was to use MRS observations to estimate PG half-life in neonatal brain.Methods
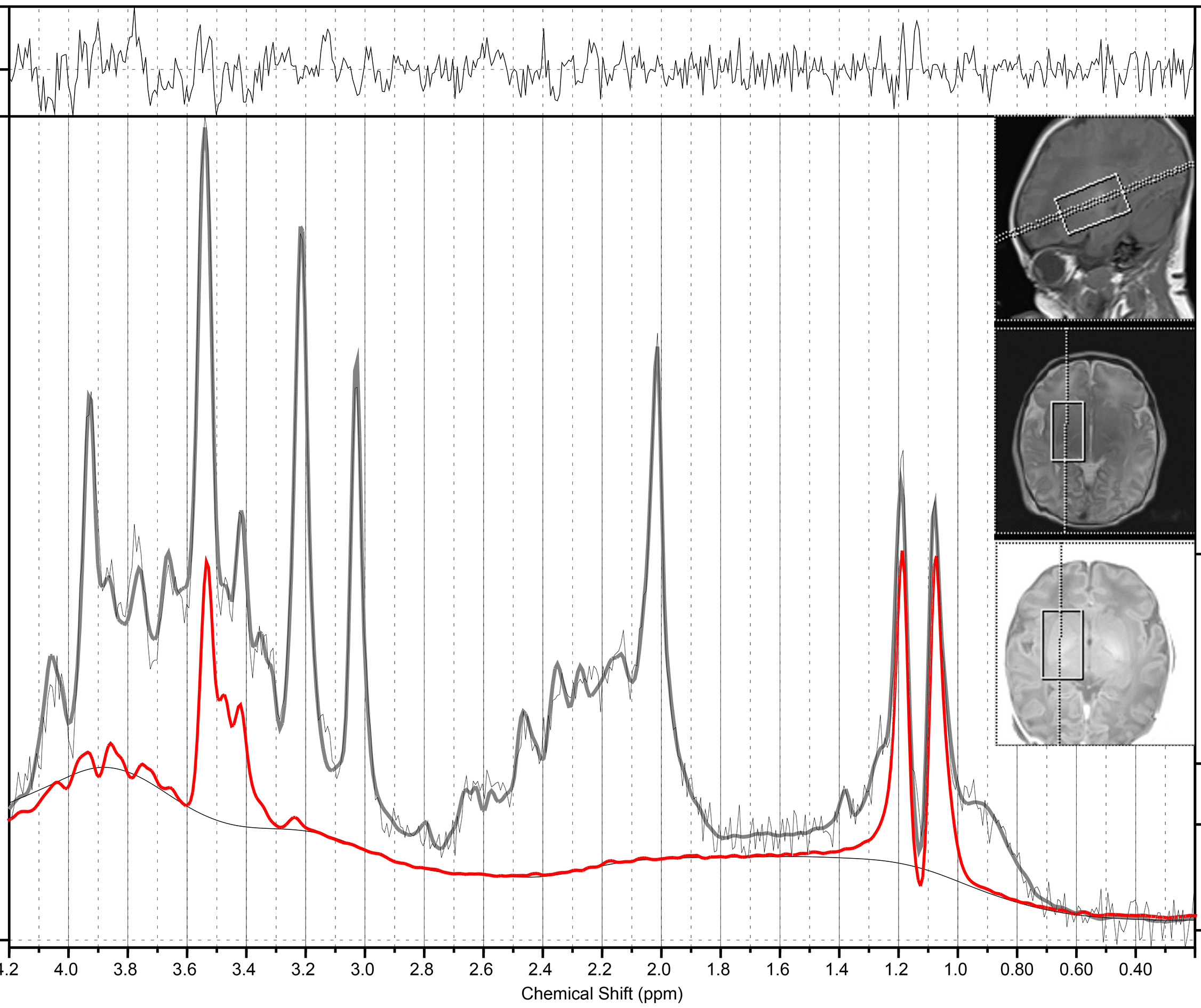
Between January 2016 and September 2018, 44 neonates were included that received one or more doses of phenobarbital and were examined with single voxel MRS at 1.5T (Siemens Avanto). Volume-of-interest was 14 mL, covering right basal ganglia and thalamus, PRESS localization, 32 averages, TR/TE 3000/30 ms. Spectra were quantified with LCModel, using a basis set of model spectra measured locally, and simulating macromolecules and lipids. Reference measurements without water suppression using both head and body coil as receiving coil were obtained for quantification, using the transmitter reference amplitude of the body coil.5
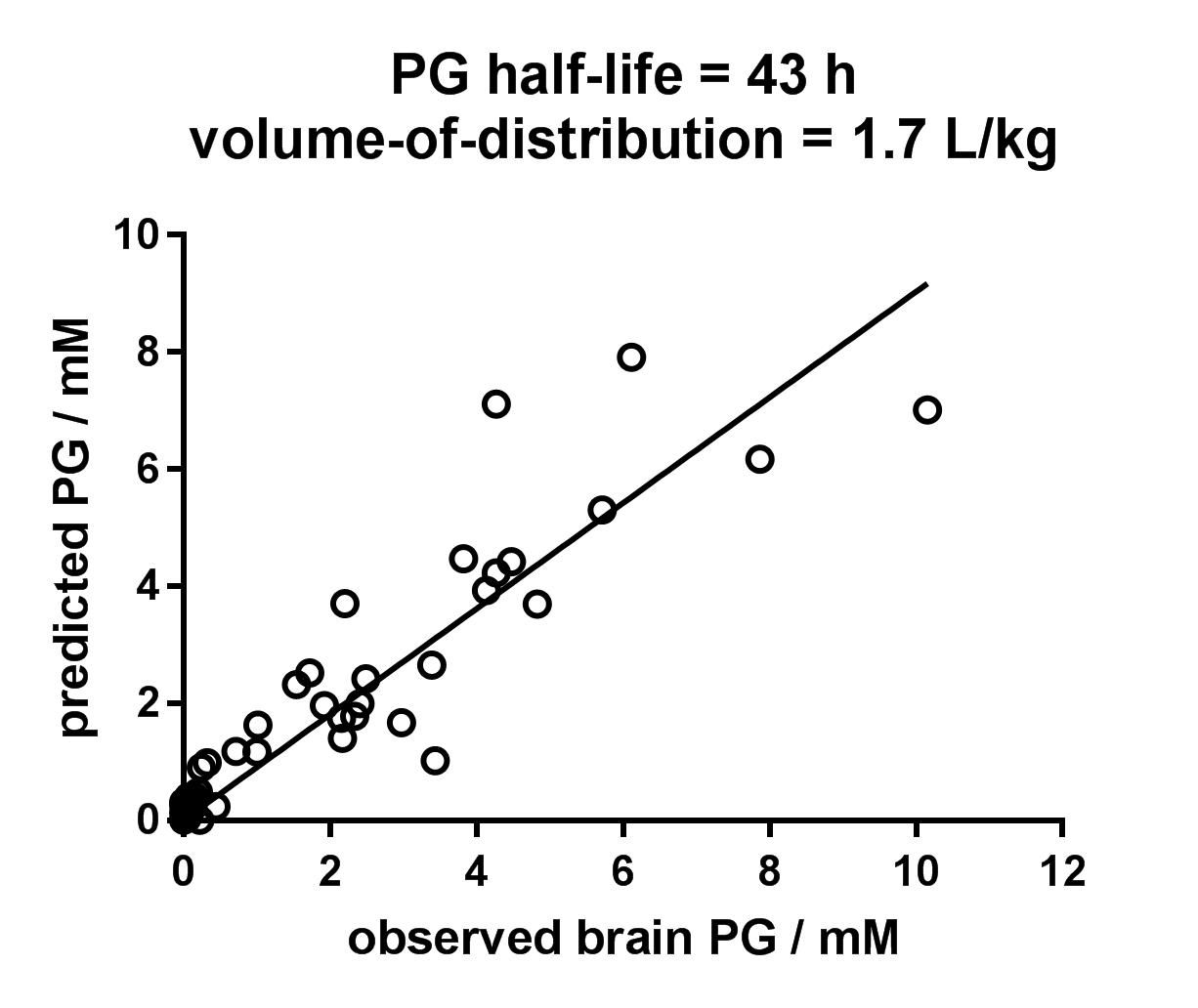
Predicted concentrations of PG were expressed as one or multiple administrations of a given dosage PGi, interval between time of administration and MRS examination, and assuming a population-based volume-of-distribution in brain tissue: PGpredicted = $$$\sum_{i}^{ }$$$PGi exp(-intervali/half-life)/volume-of-distribution. PG half-life and volume-of-distribution were estimated by least squares optimization between predicted and observed PG.
Results
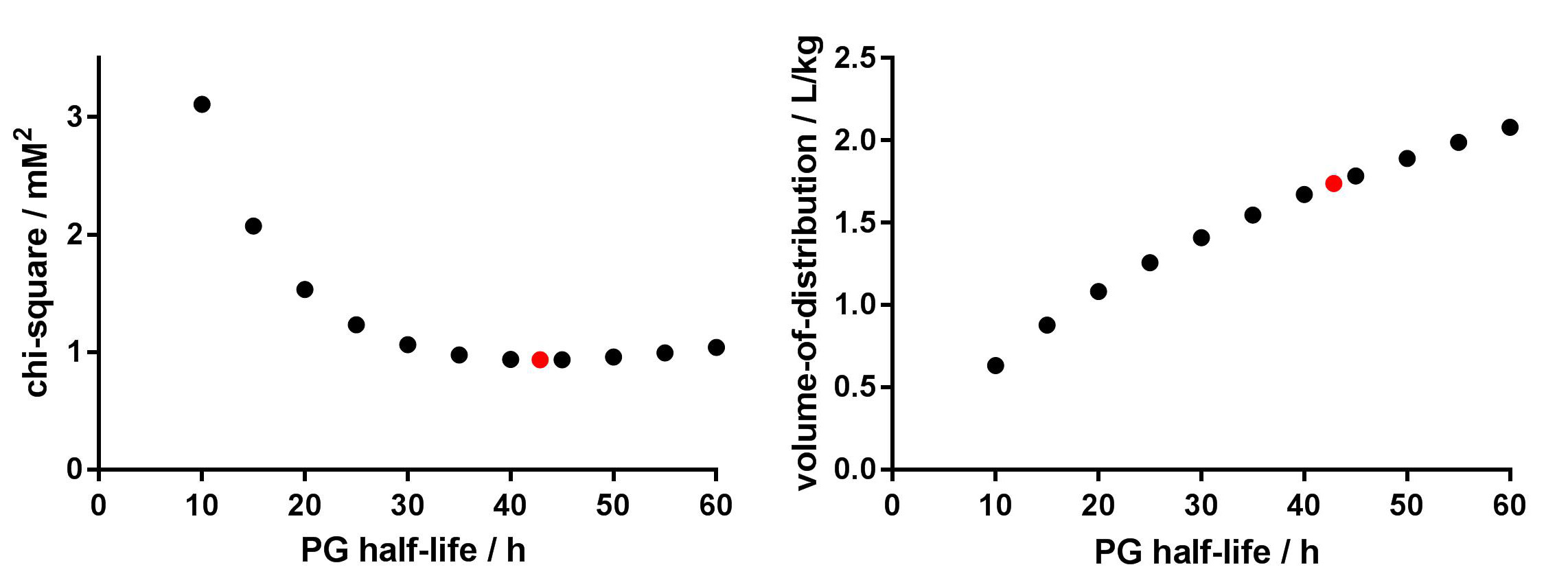
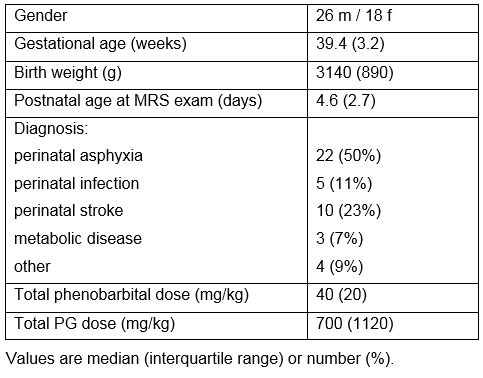
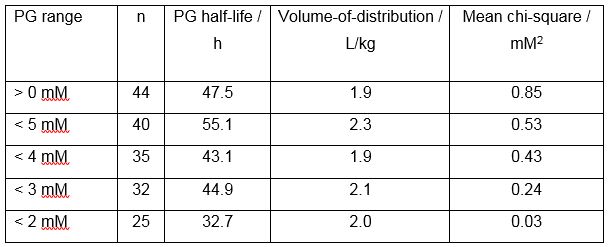
Demographics and clinical data are shown in Table 1. Most infants were term-born, had appropriate birth weight, and were examined within the first post-natal week. Median cumulative dose of PG was 700 (IQR 1120) mg/kg. The large range reflects the use of different phenobarbital solutions, containing either 10, 25 or 50 mg phenobarbital per mL, all containing 350 mg (4.6 mmol) PG per mL. VOI localization and a representative spectrum are shown in Figure 1, illustrating the high spectral quality in neonates, with median FWHM 1.0 (0.6) Hz, and SNR 16 (6) as estimated by LCModel. For spectra with PG concentration above 1 mM (n=24), median PG Cramer-Rao-lower-bound was 8%. Least-squares optimization resulted in PG half-life of 43 h and volume-of-distribution in brain tissue of 1.7 L/kg, with good correspondence between predicted and observed PG (Figure 2). Since much lower plasma half-lives were reported for the small group of neonates with low body weight,4 we investigated how well the data would also correspond to shorter half-lives. Figure 3 shows that chi-square hardly changed for half-lives between 30 and 60 h, but increased for shorter half-lives. In addition, because pharmacokinetics may change at higher concentrations of PG, we repeated the analysis for subjects with observed PG below 5, 4, 3 and 2 mM, respectively. Some variability was observed, but PG half-life remained above 30 h in all subsets of spectra (Table 2).Discussion
We determined a half-life of PG in neonatal brain of 43 h, although 30 h is also consistent with the data. This is well above or at the high end of plasma half-lives determined in neonates with low body weight (10.8 – 30.5 h).4 In our cohort, most neonates were born at term with appropriate birth weight: therefore, we had expected a shorter half-life. However, our data suggest that PG half-life in neonatal brain is even longer than assumed until now.
Ideally, the half-life of PG is examined with multiple examinations in each neonate. Our analysis was based on the assumption that the half-life of PG was similar in all neonates, although we expect inter-individual variation, especially considering the variation in clinical symptoms. Furthermore, because there was relatively small variation in body weights, we used a population-based volume-of-distribution in this analysis. Co-administration with other medication (e.g. paracetamol, phenobarbital) will prolong half-lives of each compound.6 In the current study, PG is co-administered with phenobarbital, but the ratio between PG and phenobarbital varies between infants, due to the variety in formulations. We anticipate that this may be investigated using more advanced pharmacokinetic modelling.6
Conclusion
PG has a half-life in neonatal brain of at least 30 h, but up to 43 h. When administering low-concentrated intravenous phenobarbital formulations, extremely high and potentially toxic PG concentrations will persist longer than expected in neonates.Acknowledgements
We thank Prof. Dr. M.S. van der Knaap, Dr. N.I. Wolf, and Dr. D.P. Bakker, pediatric neurologists at Amsterdam UMC, location VUMC, for their expert evaluation of MRI/MRS of all included subjects.References
1. Lim TY, Poole RL, Pageler NM. Propylene glycol toxicity in children. J Pediatr Pharmacol Ther. 2014;19(4):277-82.
2. European Medicine Agency. Questions and answers on propylene glycol used as an excipient in medicinal products for human use. In: Committee for Human Medicinal Products, editor. 2017.
3. Pouwels PJW, van de Lagemaat M, van de Pol LA, et al. Spectroscopic detection of brain propylene glycol in neonates: Effects of different pharmaceutical formulations of phenobarbital. J Magn Reson Imaging. 2018; Oct 22. doi: 10.1002/jmri.26344.
4. Glasgow AM, Boeckx RL, Miller MK, et al. Hyperosmolality in small infants due to propylene glycol. Pediatrics. 1983;72(3):353-5.
5. Natt O, Bezkorovaynyy V, Michaelis T, et al. Use of phased array coils for a determination of absolute metabolite concentrations. Magn Reson Med. 2005;53(1):3-8.
6. De Cock RF, Knibbe CA, Kulo A, et al. Developmental pharmacokinetics of propylene glycol in preterm and term neonates. Br J Clin Pharmacol. 2013;75(1):162-71.
Figures