0385
Early identification of neonatal mild hypoxic-ischemic encephalopathy by Amide Proton Transfer magnetic resonance imaging: A Pilot Study1Medical Image Center, Nanfang Hospital, Southern Medical University, Guangzhou, China, 2Philips Healthcare, Guangzhou, China
Synopsis
Neonatal hypoxic-ischemic encephalopathy (HIE) is a major complication of perinatal asphyxia, with high morbidity and morbidity. APT imaging is a potential technique for detecting in vivo characterization of the internal environment during hypoxic-ischemic brain injury. We investigated the feasibility of APT in differentiating neonatal mild HIE from normal age-matched infants, and to explore the changes in the internal environment in neonatal mild HIE. The results indicate that APT imaging for neonatal mild HIE is a useful and feasible technique with diagnostic capability.
Introduction
Neonatal hypoxic-ischemic encephalopathy (HIE) is a major complication of perinatal asphyxia, with high morbidity and morbidity, occurs in 1 to 6 per 1,000 live births1,2. The underlying pathophysiological mechanisms in HIE is inadequate blood flow and oxygen supply to the brain resulting in focal or diffuse brain injury. Conventional magnetic resonance imaging (MRI) has been more widely used in neonatal HIE. It is well known that the internal environment and brain metabolism is altered during hypoxic-ischemia. Amide proton transfer (APT) imaging is a new MRI technique that permits the non-invasive in vivo detection of endogenous mobile proteins and pH at the cellular and molecular level3. Therefore APT imaging is a potential technique for detecting in vivo characterization of the internal environment during hypoxic-ischemic brain injury. The purpose of this study was to investigate whether APT can differentiate neonatal mild HIE from normal age-matched infants, and to explore the changes in the internal environment in neonatal mild HIE.Methods
30 full-term neonates with mild HIE (16 males and 14 females; mean postnatal age 4.2 days, age rang 2–7 days) and 12 normal neonates (6 males and 6 females; mean postnatal age 3.3 days, age rang 2-5 days) underwent conventional MR imaging and APT imaging with a 3.0T clinical scanner (Achieva TX, Philips). The main imaging parameters of 3D_TSE_Dixon_APT sequence were as follows: Saturation pulse duration/power = 2s/2µT; frequency offsets = ±3.5, ±3.42, ±3.58, -1540 ppm; TR/TE =6835/6,8 ms ; FOV, 140×119×68 mm3; voxel size, 1.2×1.2×4 mm3; matrix, 116×99; SENSE factor, 2.25; scan duration, 5 min 20s.
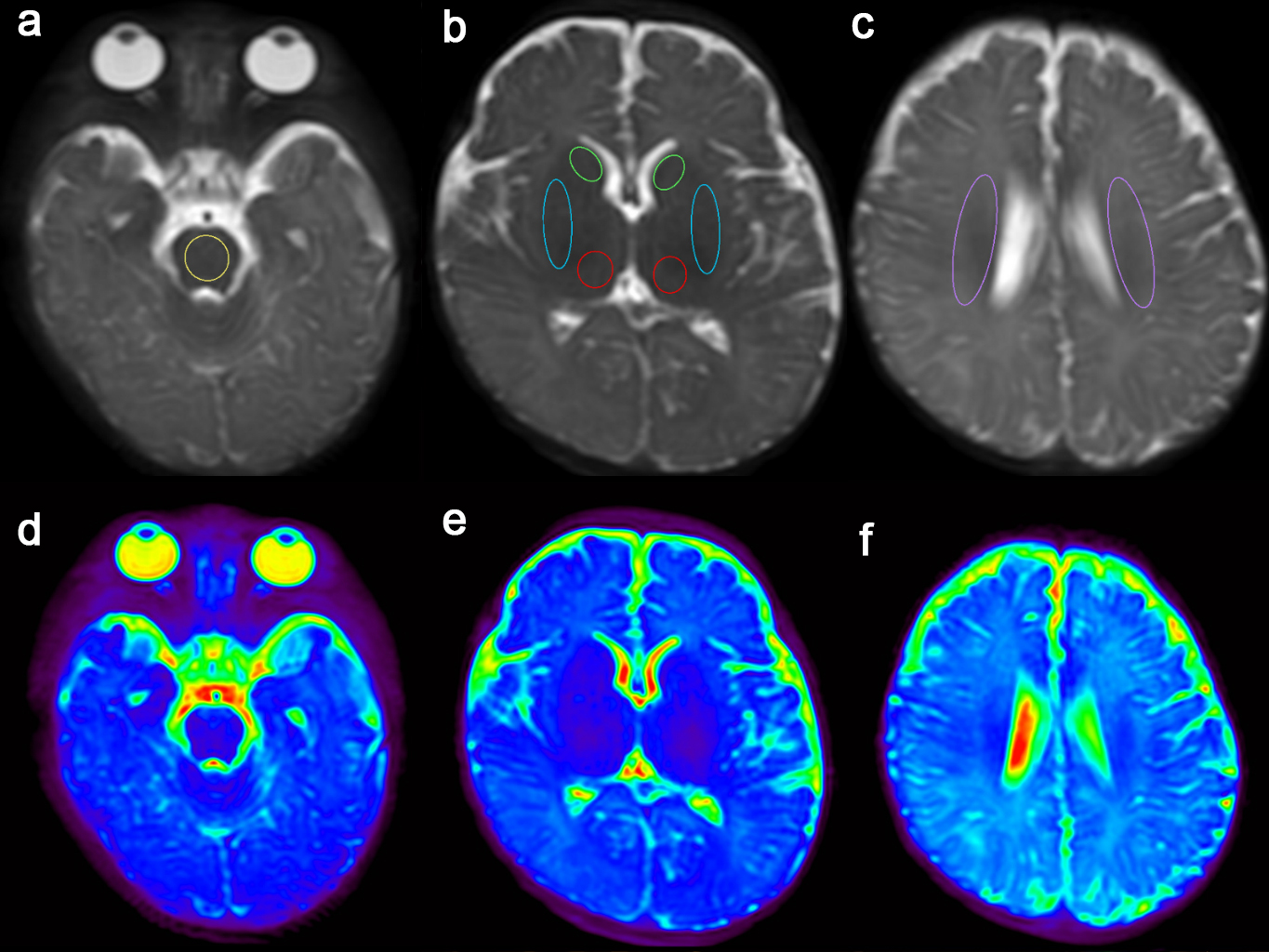
APT measurements were performed in bilateral caudate, bilateral globus pallidus/putamen, bilateral thalamus, bilateral centrum semiovale, and brainstem (Figure 1). APT values were statistically analyzed in order to assess for significant differences between the mild HIE and normal neonates in different regions of the brain, and correlation with neonate gestational age.
Results and Discussion
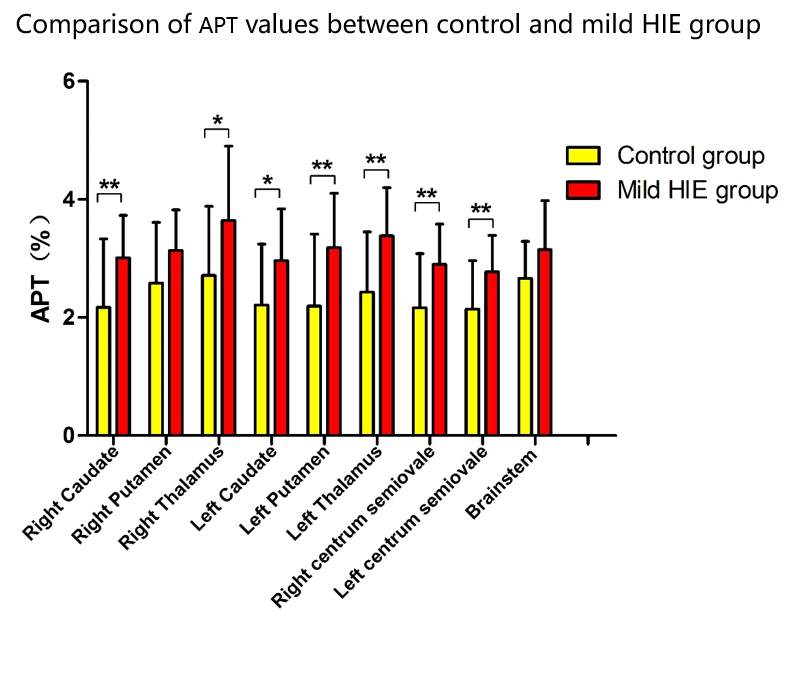
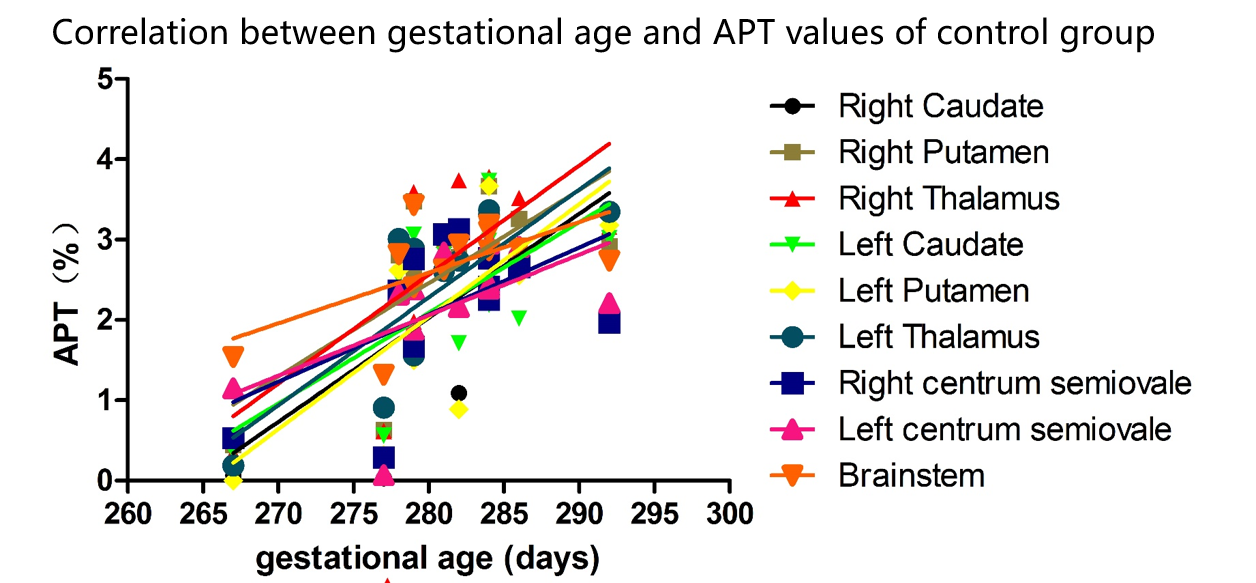
In 30 neonates with mild HIE, 10% (3/30) of the HIE patients had a normal conventional MRI. The mean MRI scores were 5.67±3.76 in HIE group. The APT values of the control group and the HIE group differed significantly in right caudate, right thalamus, left caudate, left globus pallidus/putamen, left thalamus, right centrum semiovale, and left centrum semiovale (p<0.05). No statistical difference in APT values was observed in right globus pallidus/putamen (p=0.051) and brainstem (p=0.073) between the two groups (Figure 2). Furthermore, APT in bilateral caudate, bilateral globus pallidus/putamen, bilateral thalamus, and brainstem regions (p<0.05) exhibited positive linear correlations with gestational age in control group, excepted for bilateral centrum semiovale (right: Pearson’s r=0.554, p=0.062; left: Pearson’s r=0.561, p=0.058). In mild HIE groups, APT values has no significant correlation with gestational age at all regions (Figure 3).Conclusion
In our study, APT imaging was applied to neonatal brain. The results indicate that APT imaging offers effective new tools for the characterization of brain internal environment that could enhance our understanding of the pathogenesis of neonatal HIE.Acknowledgements
NoReferences
[1] Trivedi SB, et al. A validated clinical MRI injury scoring system in neonatal hypoxic-ischemic encephalopathy. Pediatric radiology. 2017;47:1491-9.
[2] Chau V, et al. Magnetic resonance imaging in the encephalopathic term newborn. Current pediatric reviews. 2014;10:28-36.
[3] Zheng Y, ,et al. The Applicability of Amide Proton Transfer Imaging in the Nervous System: Focus on Hypoxic-Ischemic Encephalopathy in the Neonate. Cellular and molecular neurobiology. 2018;38:797-807.
Figures