0384
Electrocorticography-combined diffusion tract quantification model to improve benefit-risk assessment in pediatric epilepsy surgeryMin-Hee Lee1, Nolan Baird O'Hara2, Csaba Juhasz3, Eishi Asano4, and Jeong-Won Jeong3
1Pediatrics and Translational Imaging Laboratory, Wayne State University School of Medicine, Detroit, MI, United States, 2Translational Neuroscience Program, Wayne State University School of Medicine, Detroit, MI, United States, 3Pediatrics, Neurology and Translational Imaging Laboratory, Wayne State University School of Medicine, Detroit, MI, United States, 4Pediatrics and Neurology, Wayne State University School of Medicine, Detroit, MI, United States
Synopsis
The present study proposes a novel diffusion weighted imaging (DWI) tract classification methodology which integrates DWI-maximum a posteriori probability (DWI-MAP) analysis with Kalman filter in order to predict an optimal margin of cortical resection balancing postoperative benefit (seizure freedom) and risk (motor deficit in face, hand and leg) in pediatric epilepsy surgery. The predicted margins provided high Fisher’s exact test probability, 0.92 (0.94) of successful avoidance of motor deficits with (or without) seizure freedom. This finding demonstrates the translational value of a DWI tract classification approach in quantitative benefit-risk assessment to achieve ultimate goal of pediatric epilepsy surgery.
Introduction
Clinical management of children with drug-resistant epilepsy includes surgical resection of the epileptogenic zone following invasive electrocorticography (ECoG) recording.1,2 Thereby, clinicians intend to maximize the chance of postoperative seizure freedom (benefit) while minimizing postoperative neurological deficits such as motor function (risk). In the current ECoG practice for young children, the benefit-risk prediction is inevitably limited by poor spatial resolution and suboptimal sensitivity to localize eloquent areas at an individual patient level.3 Thus, a more structured and quantitative tool is required to provide an optimal resection margin taking into account the balance between benefit and risk of epilepsy surgery. The present study proposes a novel DWI tract classification model which integrates DWI-maximum a posteriori probability (DWI-MAP)4 analysis with Kalman filter5 in order to model “ECoG data-driven knowledge of benefit and risk” as a hidden state function of DWI-MAP-defined tract loss determined by a given surgical margin.Methods
We studied 40 children with drug-resistant epilepsy (age: 8.7±4.8 years) who underwent resection of the presumed epileptogenic zone following extraoperative ECoG recording. Newly developed postoperative motor deficits were determined during a six-month follow-up. DWI scans were acquired using a 3T scanner with 55 isotropic gradient directions and b = 1000 s/mm2. Pre- and postoperative tractography evaluations were performed by our previously described DWI-MAP analysis,4,5 where whole brain tractography of the operated hemisphere was obtained by independent component analysis with ball and stick model6 and then sorted into 3 eloquent white matter pathways using stereotaxic white matter probability maps of age-gender matched controls: "C1-3: face/hand/leg motor area-internal capsule pathway". Also, we adopted an additional streamline clustering procedure to Ci=1,2,3 where average direct-flip distance, β*i (i.e., mean distance of equally sampled bidirectional fibers to their exemplar fiber)7 was optimized to reclassify true streamlines in Ci so that their postoperative volume change (ri = 100×(volume of preoperative Ci ∩ volume of resected tissue)/volume of preoperative Ci) should maximize the prediction of postoperative deficit in binary logistic regression model. Resection margin, di, was determined by minimal Euclidean distance between voxels of Ci and resection boundary on co-registering the postoperative to preoperative b0 images. In case Ci was resected, di was assumed as -1 × maximum Euclidean distance between every paired voxel inside the resected Ci. For Kalman filter analysis to approximate the hidden relationship between the preoperatively measurable di and unmeasurable ri, it was assumed that ri is a dynamic variable to control the unknown state vector, x(ri), affecting the surgical margin, di, where Kalman filter directly models a stochastic system with dynamics: x(ri), and observation: di(ri).5 To obtain a better estimate of di(ri) in a small sample size, Rauch-Tung-Striebel algorithm7 was used to smooth the estimated di(ri) at fixed interval. An optimal margin, d*i, balancing seizure freedom with the occurrence of deficit after surgery, was found at di satisfying P(deficit|di(ri)) = P(seizure freedom|di(ri)) where P(deficit|di(ri)) and P(seizure freedom|di(ri)) represent cumulative probability density functions of seizure freedom and deficit at d ≤ di(ri), respectively. Finally, Fisher’s exact probability test8 was applied to investigate statistical significance of d*i for prediction of successful avoidance of postoperative deficit with (or without) seizure freedom.Results
Binary logistic regression analysis revealed that postoperative fiber loss, r1,2,3 of DWI-MAP-determined C1,2,3 achieved clinically relevant accuracy of 0.93, 1.00 and 0.98 for prediction of postoperative deficits in face (β*1 = 13 mm), hand (β*2 = 9 mm), and leg (β*3 = 8 mm), respectively. The subsequent Kalman filter analysis also revealed hidden nonlinear state relationships between r1,2,3 and d1,2,3 (Figure 1), yielding d*1,2,3 = -1.93, 2.29, -4.84 mm, which ultimately balanced the values of P(deficit|di(ri)) and P(seizure freedom|d(ri)) as plotted in Figure 2. The surgical margin, d, greater than the estimated d* achieved high accuracy for prediction of successful functional and seizure outcomes. Namely, Fisher’s probability of successful avoidance of motor deficits with (or without) seizure freedom was 0.83 (0.88), 0.96 (1.00), and 0.96 (0.94). Figure 3 presents safe boundaries of Ci (i.e., outmost boundaries of Ci + d*i), which is associated with preserved motor function and seizure freedom.Discussion
We have established a clinically effective DWI tractography method to allow objective prediction of surgical outcomes including postoperative functional deficits and seizure freedom. This method may help in achieving the ultimate goal of epilepsy surgery. In contrast to other tractography approaches,9-12 the proposed method was systematically validated by empirical evidence including eloquent areas, postoperative functional outcome and clinical outcome.Conclusion
Our findings demonstrate the translational value of a DWI tract classification approach in quantitative benefit-risk assessment in pediatric epilepsy surgery.Acknowledgements
This study was funded by a grant from the National Institute of Health, (R01-NS089659 to J.J and R01 NS064033 to E.A.).References
- Hader WJ, Tellez-Zenteno J, Metcalfe A, et al. Complications of epilepsy surgery: a systematic review of focal surgical resections and invasive EEG monitoring. Epilepsia. 2013;54:840-847.
- Lesser RP, Crone NE, Webber WRS. Subdural electrodes. Clin Neurophysiol. 2010;121:1376-1392.
- Haseeb A, Asano E, Juhász C, et al. Young patients with focal seizures may have the primary motor area for the hand in the postcentral gyrus. Epilepsy Res. 2007;76:131-139.
- Jeong JW, Asano E, Brown EC, et al. Automatic detection of primary motor areas using diffusion MRI tractography: Comparison with functional MRI and electrical stimulation mapping. Epilepsia. 2013;54:1381-1390.
- Jeong JW, Asano E, Juhász C, et al. Quantification of primary motor pathways using diffusion MRI tractography and its application to predict postoperative motor deficits in children With focal epilepsy. Hum Brain Mapp. 2014;35:3216-3226.
- Jeong JW, Asano E, Yeh FC, et al. Independent component analysis tractography combined with a ball-stick model to isolate intra-voxel crossing fibers of the corticospinal tracts in clinical diffusion MRI. Magn Reson Med. 2013;70:441-453.
- Garyfallidis E, Brett M, Correia MM, et al. QuickBundles: a method for tractography simplification. Front Neurosci. 2012;6:175.
- Rauch HE, Tung F, Striebel CT. Maximum likelihood estimates of linear dynamic systems, AIAA J. 1965;3:1445-1450.
- Agresti A, A survey of exact inference for contingency tables. Stat Sci. 1992;7:131-153.
- Guevara P, Duclap D, Poupon C, et al. Automatic fiber bundle segmentation in massive tractography datasets using a multi-subject bundle atlas. Neuroimage. 2012;61:1083-1099.
- O'Donnell L J, Suter Y, Rigolo L, et al. Automated white matter fiber tract identification in patients with brain tumors. NeuroImage Clin. 2017;13:138-153.
- Garyfallidis E, Côté MA, Rheault F, et al. Recognition of white matter bundles using local and global streamline-based registrations and clustering. Neuroimage. 2018;170:283-295.
Figures
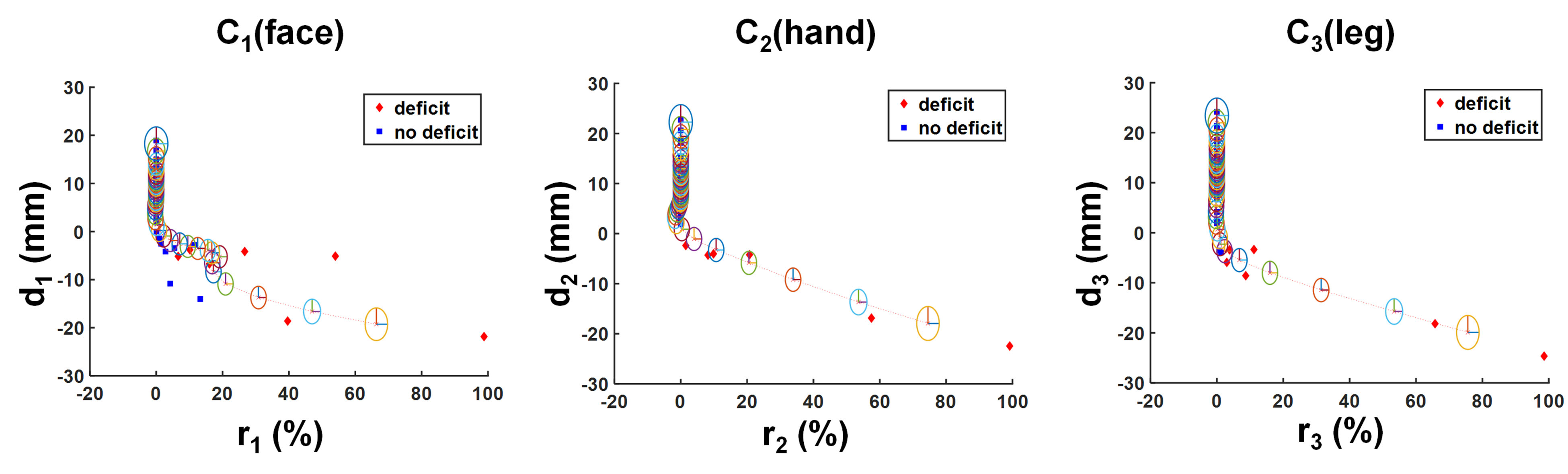
Surgical margin, di=1,2,3 predicted by
the proposed Kalman filter analysis using state dynamic state variable of ri=1,2,3,
which was determined by the DWI-MAP analysis class of Ci=1,2,3. Note
that the thresholds of average direct-flip distance, β*i=1,2,3 = 13, 9, 8 mm were applied to
reclassify streamlines in the original DWI-MAP-determined Ci=1,2,3.
Radius of each ellipsis indicates the covariance of state variable x(ri).
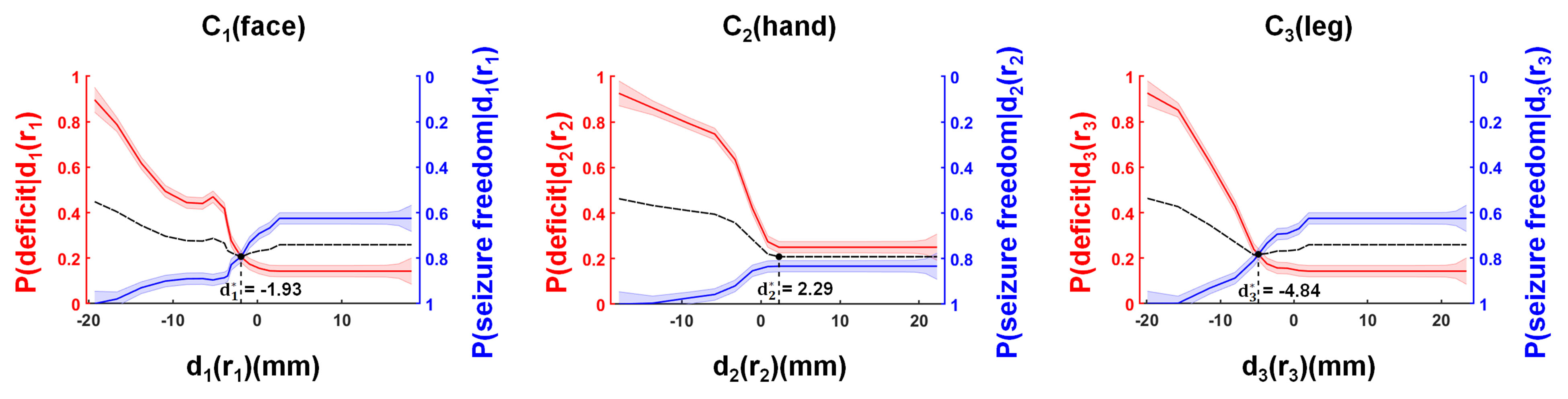
Identification of the surgical margin, d*i=1,2,3 = -1.93, 2.29, -4.84 mm, which were optimized to balance P(deficit|di=1,2,3(ri=1,2,3))
vs. P(seizure freedom|di=1,2,3(ri=1,2,3)) at DWI-MAP-determined
Ci=1,2,3. The width of the strips indicates ± 1×covariance of the predicted P(deficit|di(ri))
and P(seizure freedom|di(ri)). A solid dotted line
indicates the average value of P(deficit|di(ri)) and
P(seizure freedom|di(ri)).
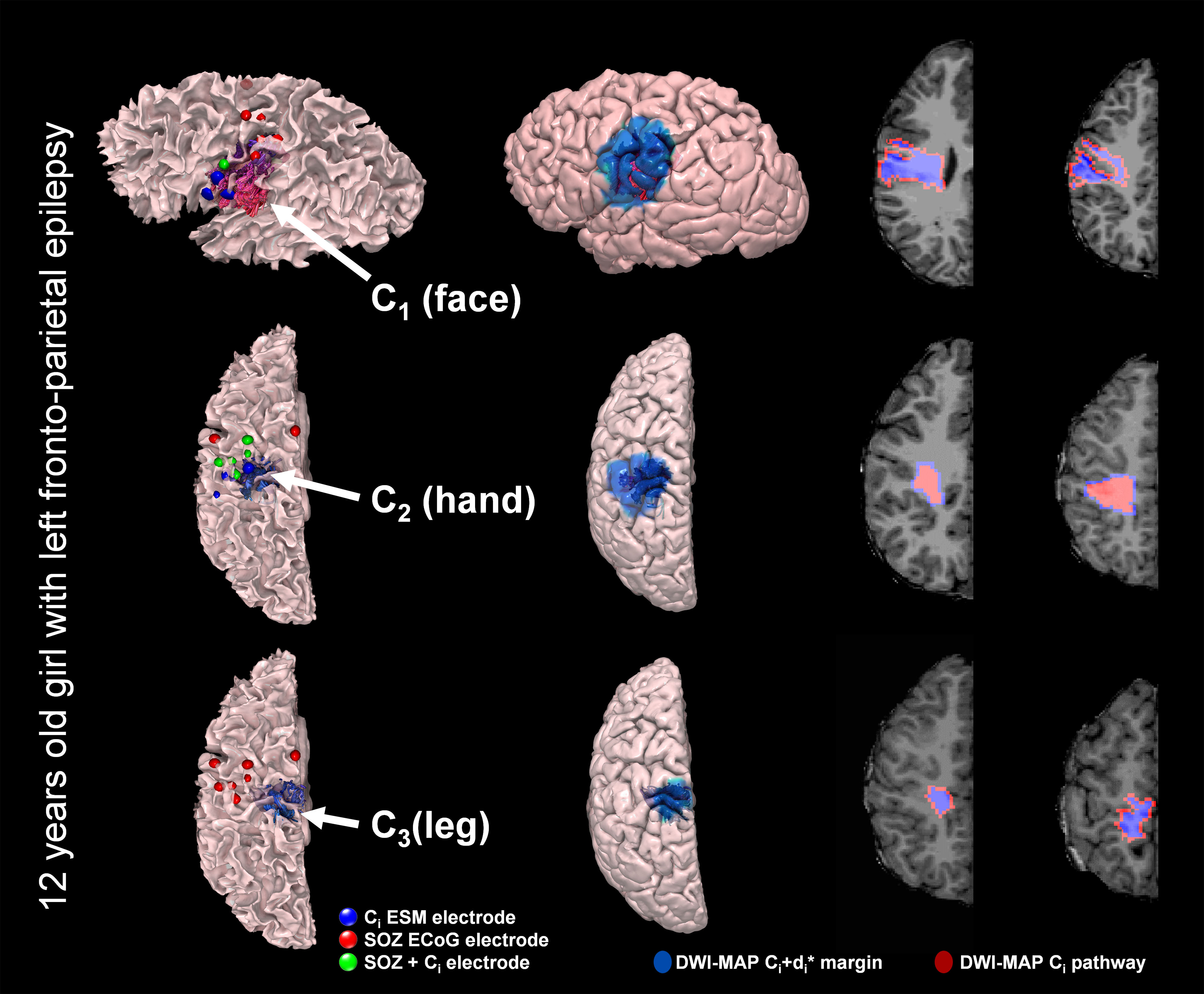
Representative examples of safe boundaries
estimated to preserve intact motor functions. For each of Ci=1,2,3,
the safe boundary was determined by adding the optimal margin, d*i
to outmost boundaries of DWI-MAP-determined Ci.