0379
Evaluation of an eight element AIR coil array for MRI in the prostate1Department of Radiology, Mayo Clinic, Rochester, MN, United States
Synopsis
Obtaining sufficient SNR in MRI of the prostate can be problematic without the use of an endorectal coil (ERC). We have constructed a lightweight, highly flexible receive-only surface coil array consisting of 8 recently developed AIR coil elements (GE Healthcare, Waukesha, WI, USA). This work compares the AIR coil array to commercial arrays commonly used for prostate imaging with and without the inclusion of an ERC. Initial phantom results show that the AIR coil array has approximately 2.5-3× higher SNR than the GE 32 channel anterior body/GEM posterior array when no ERC is used and approaches ERC SNR performance.
Introduction
Prostate cancer is the most common non-cutaneous malignancy found in males in the United States 1 and common worldwide. Early detection and staging greatly increase chances of successful treatment. While MRI is the modality of choice for the detection and characterization of prostate cancer, the anatomical position of the prostate in the lower pelvis presents challenges to obtaining sufficient image signal-to-noise ratio (SNR) and image uniformity. Additionally, the “optimal” MRI coil geometry for clinical prostate MR imaging has yet to be determined. Often the use of an endorectal coil (ERC) is necessary to achieve the desired SNR but is not ideal from the standpoint of patient acceptance, patient preparation, and positioning time. Also, the majority of MRI vendor coil arrays have limited mechanical flexibility which places limits on the ability to locate coil elements in close proximity to the prostate. We have constructed a prototype eight-element array using recently developed Adaptive Image Receive (AIR) coil technology (GE Healthcare, Waukesha, WI, USA) consisting of two four-element pads. The array is extremely flexible enabling the anterior and posterior pads to be folded in place around the prostate anatomy. The goal of this work is to compare SNR in the prostate between our custom AIR coil array and the 32 channel GE anterior body/GEM posterior array with and without an ERC.
Methods
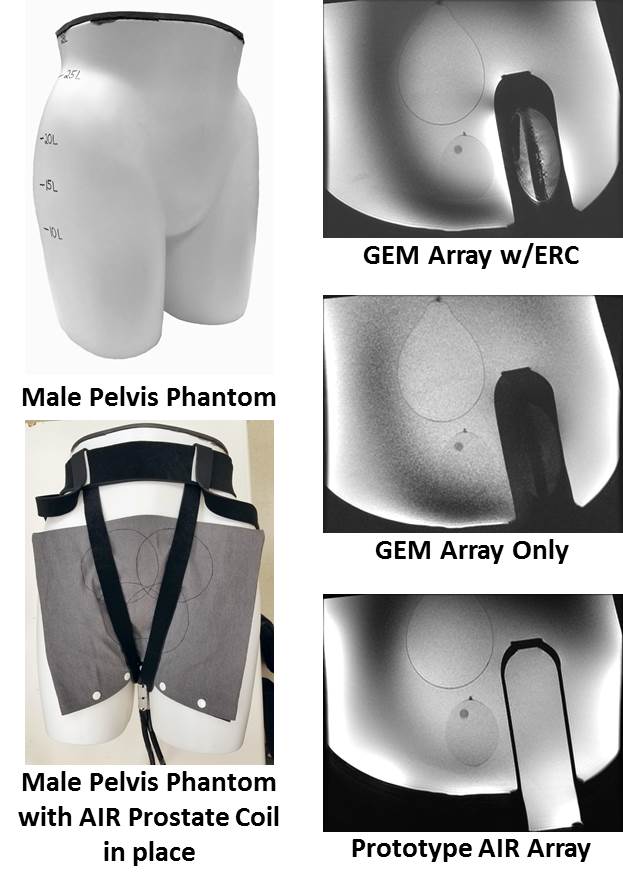
The prostate array consists of two separate pads each composed of four 11 cm diameter AIR coil elements. Elements within each pad are arranged in a semi-cloverleaf configuration with a superior-inferior overlap between elements of 3 cm, right-left overlap of 3 cm for the superior and 6 cm for the inferior elements resulting in in a slightly higher coil density near the prostate. This is possible using the AIR coil elements because they do not suffer from coil-to-coil inductive interference to the same degree as traditionally tuned coil array elements 2. Each AIR coil element is stitched on to a 2.25 mm thick neoprene fabric substrate and covered with an elastic polyester fabric. A flexible plastic cover is placed over the arrays during use to prevent the ingress of contaminants. The arrays are held in place by a flexible harness similar in design to those used in rock climbing. Imaging was performed in a phantom described and shown in Figure 1. Data was obtained in the phantom using Axial T2-weighted spin-echo (T2), Sagittal T2 and Axial Diffusion Weighted (DWI) pulse sequences commonly prescribed for prostate imaging at our institution and included in the PI-RADS protocol 3. Three coil arrangements were used: (i) AIR coil; (ii) the 32 channel GE anterior body/GEM posterior array with and (iii) without an ERC in a phantom. Mean SNR as well as SNR profiles in two directions (AP and RL) were determined for all sequences in the prostate-mimicking region of the phantom. In a separate experiment the performance of the new AIR coil array was assessed in a subject who was clinically indicated for prostate MRI who gave informed consent.Results
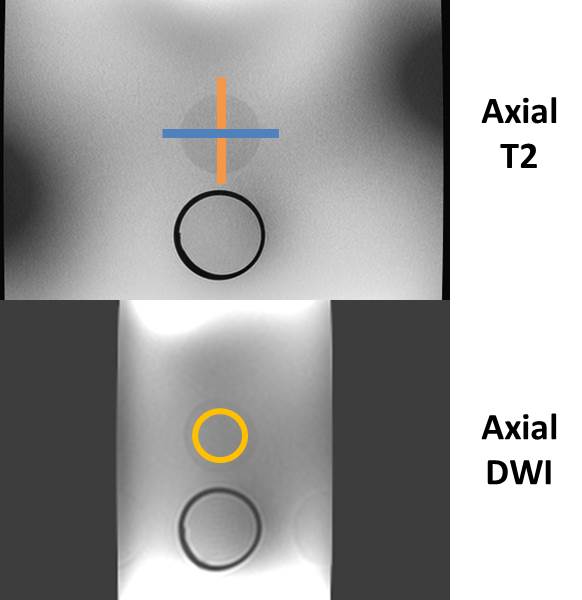
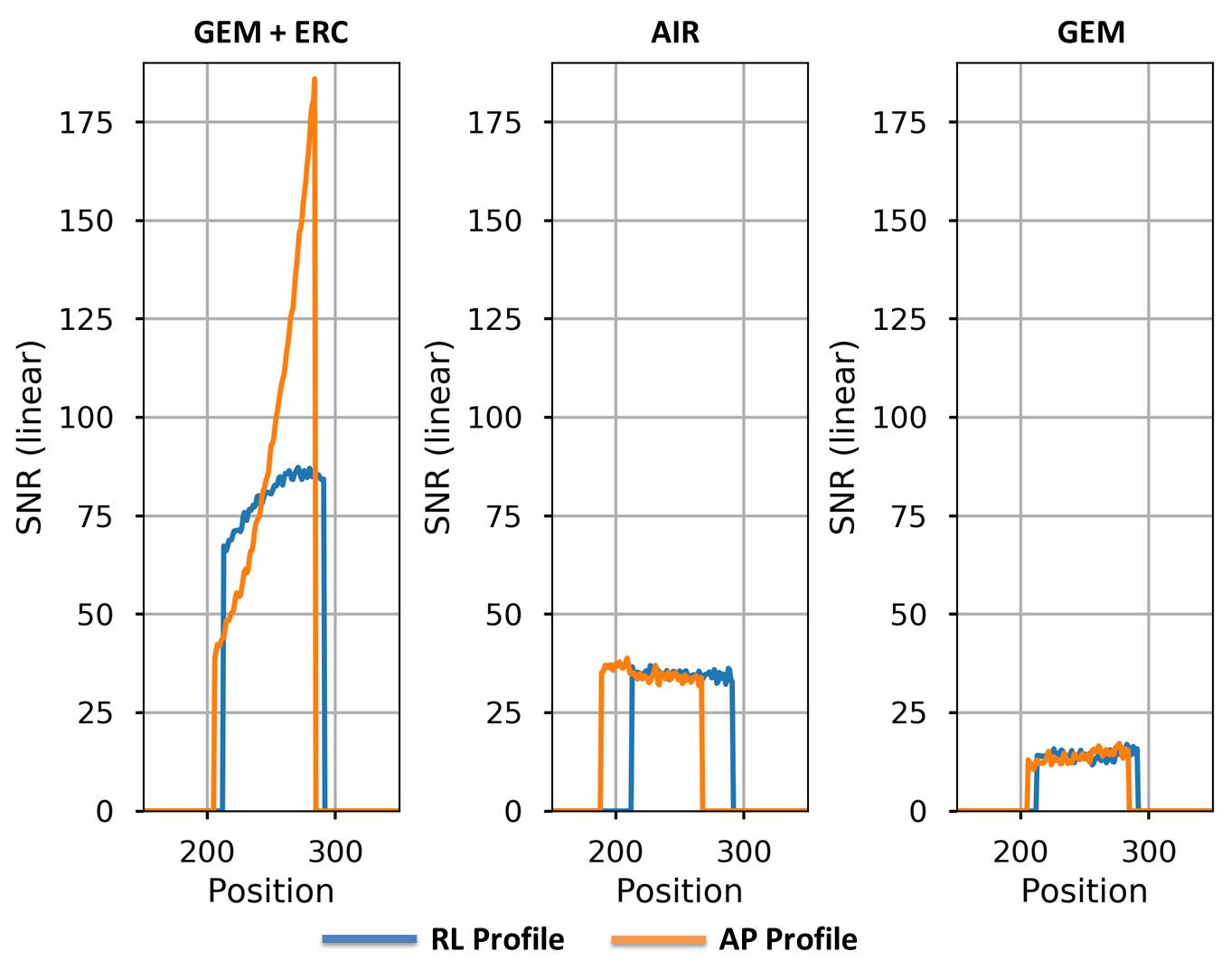
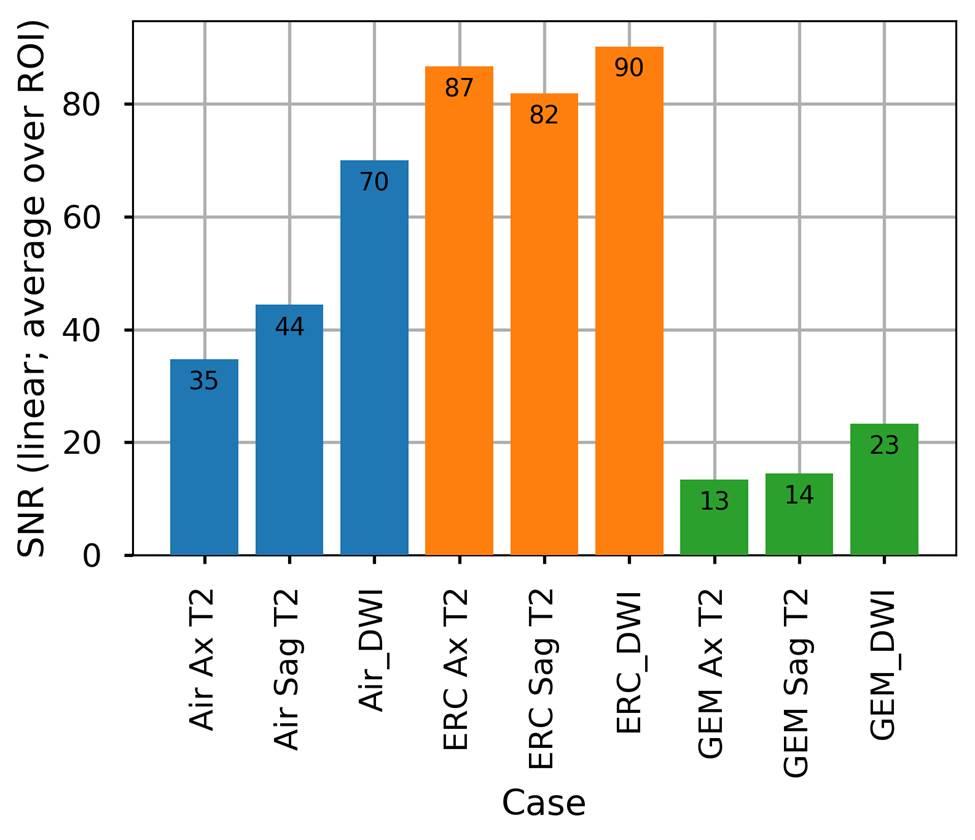
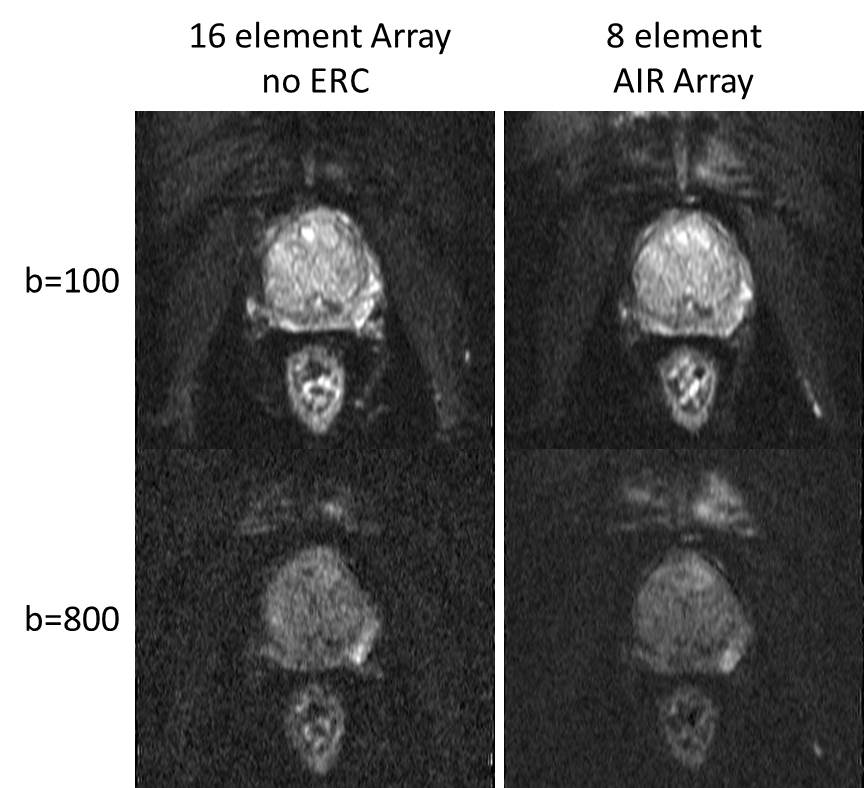
Figure 2 shows the profile and ROI locations from where the SNR data was obtained. Figure 3 shows the SNR results from the AP and RL profiles through the prostate inclusion. Figure 4 shows a comparison between the mean SNR values over all ROIs for each coil and imaging sequence. The GEM with ERC combination has the highest SNR over all three pulse sequences. However, note that the AIR coil array SNR significantly outperforms the standard surface coil array alone. Figure 5 shows DWI results from a volunteer with two b-values.Discussion
While the use of an endorectal coil in imaging of the prostate is considered standard of care, it has significant drawbacks including: additional time for coil placement and positioning, patient discomfort, and the need for post processing algorithms to correct for image inhomogeneity. The ability to obtain adequate SNR and signal uniformity solely using surface coils would be a major simplification. Our preliminary phantom results suggest that a significant increase in SNR in the prostate and lower pelvis can be obtained using highly flexible arrays consisting of AIR coil elements over more traditional surface coil arrays (without the inclusion of an ERC). It is also important to note that the prototype described included only eight coil elements, a factor of four less than the commercial phased array coil used for comparison. Future development will include more elements. This will allow for more pelvic coverage as well as enable higher coil densities which will in turn increase the SNR in the regions of interest.Acknowledgements
The authors would like to extend their appreciation to Robert Stormont, Scott Lindsay and Fraser Robb (GE Healthcare, Waukesha, WI, USA) for their technical support throughout this work.References
1) American Cancer Society. Cancer Facts and Figures. 2017.
2) McGee KP, et al “Characterization and evaluation of a flexible MRI receive coil array for radiation therapy MR treatment planning using highly decoupled RFcircuits” 2018 Phys. Med. Biol. 63 08NT02.
3) Weinreb JC, Barentsz JO, Choyke PL, Cornud F, Haider MA, Macura KJ, Margolis D, Schnall MD, Shtern F, Tempany CM, Thoehy HC, Verma S. PI-RADS Prostate imaging - Reporting and Data System: 2015, Version 2. Eur Urology 2016;69:16-40.
Figures