0377
Prospects of a Dedicated Nonlinear Gradient for Prostate DWI1Radiology and Biomedical Imaging, Yale University, New Haven, CT, United States
Synopsis
DWI is a crucial contrast for prostate cancer, not only for detection but also biopsy guidance and monitoring. Unfortunately, DWI of prostate is plagued by very low SNR, caused by the long TEs needed to encode diffusion with standard imaging gradients. Here we show that by abandoning typical requirements of an imaging gradient, especially nonlinearity, very strong diffusion weighting can be locally achieved using a single standard amplifier, greatly improving DWI image quality. Experiments verify the feasibility of DWI with nonlinear gradients. Though prostate is an ideal first target, this approach could find application in many other organs.
Introduction
Diffusion weighted imaging (DWI) gives the most sensitive and specific technique available to noninvasively detect lethal prostate cancer1-4. Improved DWI would impact not only diagnosis, but also surgical planning, treatment monitoring, and especially biopsies, which currently have low hit rates and are often inconclusive5-7. However, DWI is plagued by extremely low signal because the weak gradients designed for imaging require long echo times to achieve sufficient encoding.
This work studies the potential of an MR gradient specifically designed for DWI of prostate. By abandoning typical gradient requirements on linearity, directionality, active volume, and rapid switching, an initial design achieves >400mT/m in the region of interest. Moreover, this equipment has potential to be implemented as an accessory compatible with any scanner, encouraging rapid adoption in practice.
The presented simulations show the likely impact of this dedicated gradient, including improvements in SNR, CNR and higher b-value imaging. In addition, experiments on phantoms show that diffusion weighting with nonlinear gradients is feasible and produces ADC maps and DW images in agreement with those from conventional gradients.
Methods
Following the aforementioned specifications a prototype was designed by Tesla Engineering Ltd, who also provided the expected performance for gradient strength, rise time, maximum temperature, and device size. Simulations were performed in Matlab assuming equal T2* between prostate cancer and healthy peripheral zone tissue (32ms as measured at 3T in 3 patients) and D=0.36E-3 and 0.70E-3 for healthy and cancerous prostate tissue, respectively. Experiments were performed on a phantom of kiwi embedded in agarose gel. Both linear and nonlinear fields were mapped by a series of gradient echo images, and the resulting field maps were used to generate maps of gradient and b-value for each experiment. The signal from each voxel was fit to a monoexponential using b-values appropriate to that voxel, and those parameters were used to scale DWI images to a uniform diffusion weighting.Results
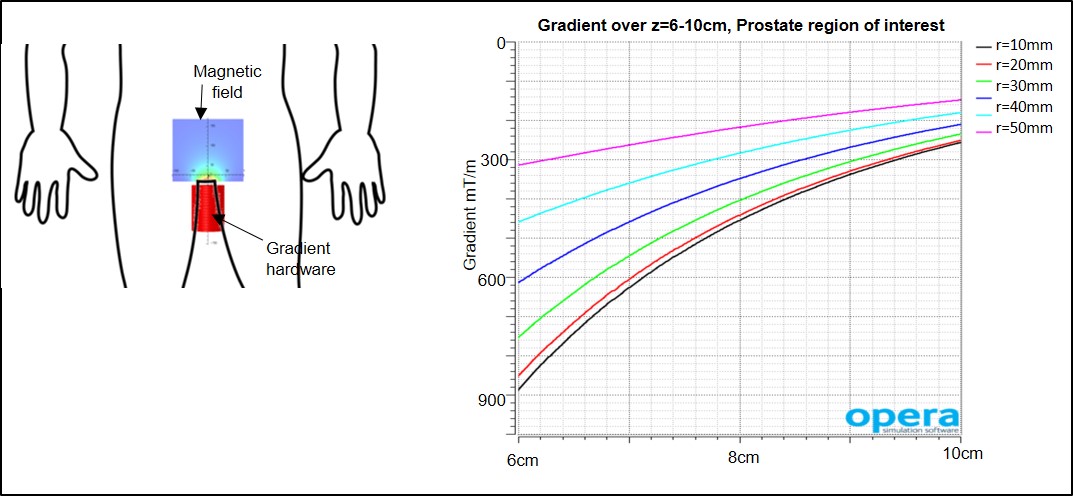
Figure 1 shows a schematic of the proposed device and the gradient (dBz/dz) it achieves across the prostate, which was found to be 6-10cm from the perineal surface according to MR images. The gradient is designed to be centered in the bore, which minimizes forces and coupling, and it can be controlled by simple trigger pulses in the pulse sequence. For patient comfort and safety, the device has a radius of 5cm and is water cooled to a maximum temperature of 43C.
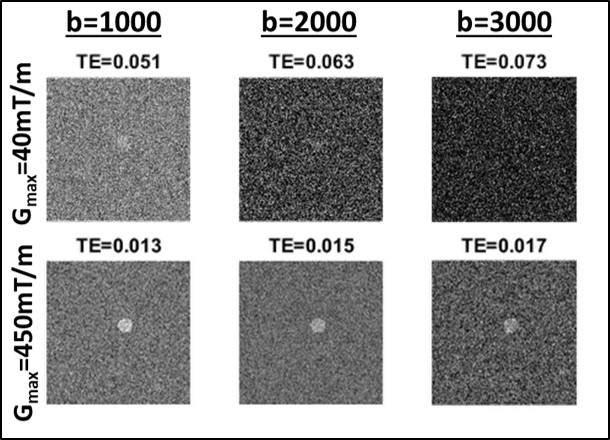
Figure 2 shows simulations of a circle of prostate cancer embedded in healthy prostate tissue. At a typical high b-value (b=1000) SNR can be very low, but using the gradient strengths achieved in our preliminary design requires less time, giving much better SNR. Furthermore, at the same noise level, it becomes feasible to explore still higher b-values while maintaining adequate SNR.
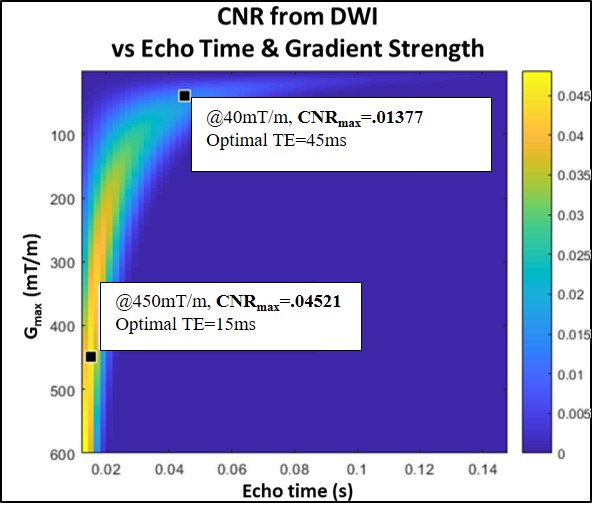
To look more generally at the achievable contrast, Figure 3 shows, for any combination of echo time and gradient amplitude (x and y axes, respectively), the contrast to noise ratio between prostate and prostate cancer (color scale). At 450mT/m, as achieved by the proposed hardware, much higher CNR is possible, encoded in less than 20ms with far less signal loss. These simulations suggest a tripling of contrast is possible with the proposed hardware.
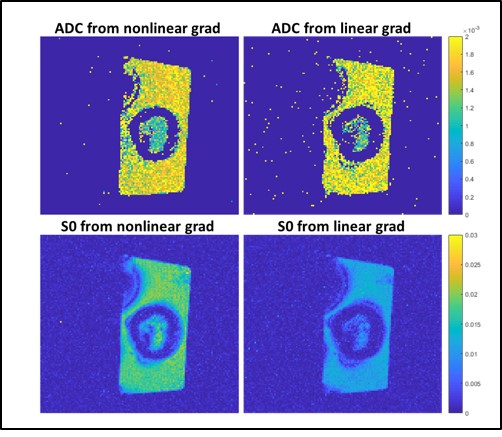
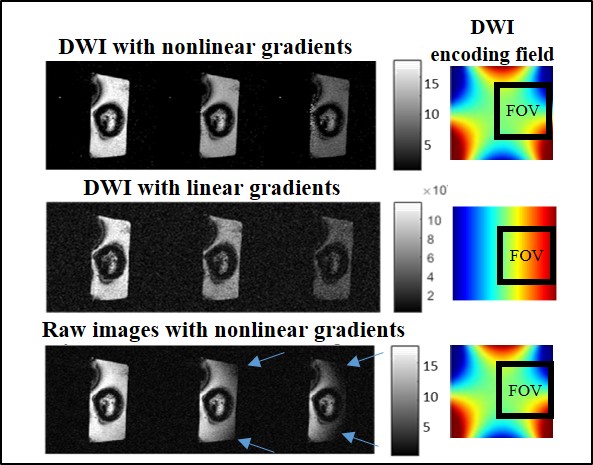
One key to achieving an order of magnitude increase in gradient strength is accepting nonlinearity in the field, which creates nonuniform diffusion weighting across the image. Figure 4 proves the experimental feasibility of encoding diffusion with nonlinear gradients. ADC maps generated from experiments with linear and nonlinear gradients have highly concordant values. Though these proof of concept experiments do not use gradients optimized for DWI, the nonlinear gradients required far less encoding time for comparable diffusion weighting because of their natural steepness at the periphery. This already lead to a doubling in SNR, as can be seen in maps of S0.
Figure 5 shows how results can also be used to generate DWI images with uniform diffusion weighting, again showing agreement between images acquired with nonlinear and linear gradients. The raw data acquired with nonlinear gradients (bottom row), show the spatial nonuniformity of b-weighting. However, this is easily and effectively corrected to yield images equivalent to those with linear gradients, but with higher SNR.
Conclusion
By abandoning typical requirements of an imaging gradient, especially nonlinearity, very strong diffusion weighting can be locally achieved using a single standard amplifier, greatly improving SNR in DWI. Prostate is an ideal first target, though this approach could find application in many other organs8.Acknowledgements
We thank Steve Bates and Xavier Mooney of Tesla Engineering Ltd for providing a preliminary design for this project. We also thank Andrew Dewdney of Siemens and Terry Nixon of Yale for contributing numerous helpful comments on design specifications.References
1. Weinreb JC, Barentsz JO, Choyke PL, et al. PI-RADS Prostate Imaging - Reporting and Data System: 2015, Version 2. Eur Urol. 2016;69(1):16-40.
2. Shaish H, Kang S, Rosenkrantz A. The utility of quantitative ADC values for differentiating high-risk from low-risk prostate cancer: a systematic review and meta-analysis. Abdom Radiol (NY).42:260-270.
3. deSouza NM, Riches SF, Vanas NJ, et al. Diffusion-weighted magnetic resonance imaging: a potential non-invasive marker of tumour aggressiveness in localized prostate cancer. Clin Radiol. 2008;63(7):774-782.
4. Kitajima K, Takahashi S, Ueno Y, et al. Do apparent diffusion coefficient (ADC) values obtained using high b-values with a 3-T MRI correlate better than a transrectal ultrasound (TRUS)-guided biopsy with true Gleason scores obtained from radical prostatectomy specimens for patients with prostate cancer? Eur J Radiol. 2013;82(8):1219-1226.
5. Siddiqui MM, Rais-Bahrami S, Turkbey B, et al. Comparison of MR/ultrasound fusion-guided biopsy with ultrasound-guided biopsy for the diagnosis of prostate cancer. JAMA. 2015;313(4):390-397.
6. Shin T, Smyth TB, Ukimura O, et al. Detection of prostate cancer using magnetic resonance imaging/ultrasonography image-fusion targeted biopsy in African-American men. BJU international. 2017;120(2):233-238.
7. Ong WL, Weerakoon M, Huang S, et al. Transperineal biopsy prostate cancer detection in first biopsy and repeat biopsy after negative transrectal ultrasound-guided biopsy: the Victorian Transperineal Biopsy Collaboration experience. BJU international. 2015;116(4):568-576.
8. Feng J, Littin S, Kroboth S, et al. Design of a breast gradient coil with the control of field nonlinearity. ISMRM 2018; 2018; Paris.
Figures