0361
Assessing somatotopic and mototopic organisation in Focal Hand Dystonia using high-resolution 7T fMRI1Sir Peter Mansfield Imaging Centre, School of Physics and Astronomy, University of Nottingham, Nottingham, United Kingdom, 2School of Psychology, University of Nottingham, Nottingham, United Kingdom, 3Department of Neurology, Nottingham University Hospitals Trust, University of Nottingham, Nottingham, United Kingdom
Synopsis
7T fMRI provides a non-invasive method to study somatotopy and mototopy. Here, healthy controls (HCs) and Focal Hand Dystonia (FHD) patients 4-weeks post-Botox injection undergo behavioural and fMRI assessment. Behavioural measures include temporal discrimination, amplitude thresholding and spatial acuity assessment. fMRI includes a somatosensory travelling wave and event-related paradigm, and mototopy travelling wave paradigm. In FHD patients, amplitude threshold, temporal discrimination threshold and spatial acuity was increased compared to HCs. Maps of somatotopy and mototopy are shown for FHD patients and HCs along with digit separation. FHD patients will be rescanned 3 months post-Botox to determine whether changes are evident.
Introduction
Somatotopic mapping of the digits in primary somatosensory cortex has been shown to be highly reproducible in healthy controls (HC) using high-resolution (7T) BOLD-fMRI and a travelling wave (TW) paradigm1,2, while event-related fMRI has demonstrated cortical digit overlap3. Previous studies in Focal Hand Dystonia (FHD) patients have shown reduced inter-digit distances4 and increased overlapping activity5 compared to HCs6. Somatosensory temporal discrimination thresholds (TDT) are often raised in both the affected and unaffected hands of FHD patients compared to HCs7 and correlate with disease severity, and spatial acuity thresholds are raised8.
Here, we aim to assess somatotopy and mototopy in FHD patients. A behavioural battery including TDT, amplitude thresholding and spatial acuity using a grating orientation task (GOT); and an fMRI battery involving a somatosensory TW and event-related paradigm, and a motor TW paradigm, was performed on 5 FHD patients 4-weeks post-Botulinum-Toxin A (Botox) treatment and 3 HCs. This is an ongoing study with patients returning 3 months post-injection to determine whether treatment induces cortical reorganisation.
Methods
The protocol, comprising behavioural and fMRI collection, was piloted on nine/seven healthy volunteers (behavioural/fMRI). To date, data has been collected on six FHD patients (5 right-handed (RH) and affected hand) and three age-matched HCs (all RH), with patients attending approximately 4 weeks post-injection. One patient was removed from fMRI analyses due to excessive movement.
Behavioural: TDT: Short stimuli were presented consecutively to the index (D2) and middle (D3) finger via piezo-electric stimulators and a descending staircase procedure used to determine TDT. The TDT was also conducted using a Brain Gauge9 (pneumatic mouse-like device). Amplitude thresholding: Performed on D2 at 31 and 200Hz in both hands. GOT: Plastic domes with square-wave gratings were presented to D2 of the affected hand in either proximal or lateral directions and the 75% correct gap width determined.
fMRI acquisition and analysis: Data were acquired on a 7T Philips Achieva scanner using a 32-channel Nova head coil. All fMRI scans were collected using GE-EPI with multiband3, TE=25ms, SENSE1.5 and 1.5mm isotropic voxels. Structural 1mm3 isotropic MPRAGE and T2*-weighted FLASH scans were collected for Freesurfer segmentation and alignment/vein masking. Somatosensory & Mototopy TW: TR=2000ms, FA=80°, 48 slices, 80 dynamics. A TW was performed in forward (D1-D5) and reverse directions (D5-D1) with 20s/cycle for 8 repeats on both hands. Fourier analysis produced maps of coherence and phase (digit correspondence). Mototopy was visually cued for 1Hz digit movement and quality controlled using a MRI compatible custom-built accelerometer system for independent monitoring of each digit. For somatotopy and mototopy, digit distance on the cortical surface was measured by computing the centre of mass of each digit-phase ROI (coherence=0.3, uncorrected p=0.0034) and estimating the Dijkstra’s and 3D-Euclidean distance of D1-D5. Event-related/ON-OFF: TR=1000ms, FA=57°, 36 slices, 285 dynamics. The ON-OFF paradigm (5s-ON, 24s-OFF) was performed on the affected hand only (2 scans) and stimuli randomised between D2, D3, and D4. A GLM analysis was performed to derive digit-specific HRFs and Z-score maps of each digit location from which digit overlap was assessed by the number of voxels shared between D2,D3,D4 ROIs.
Results
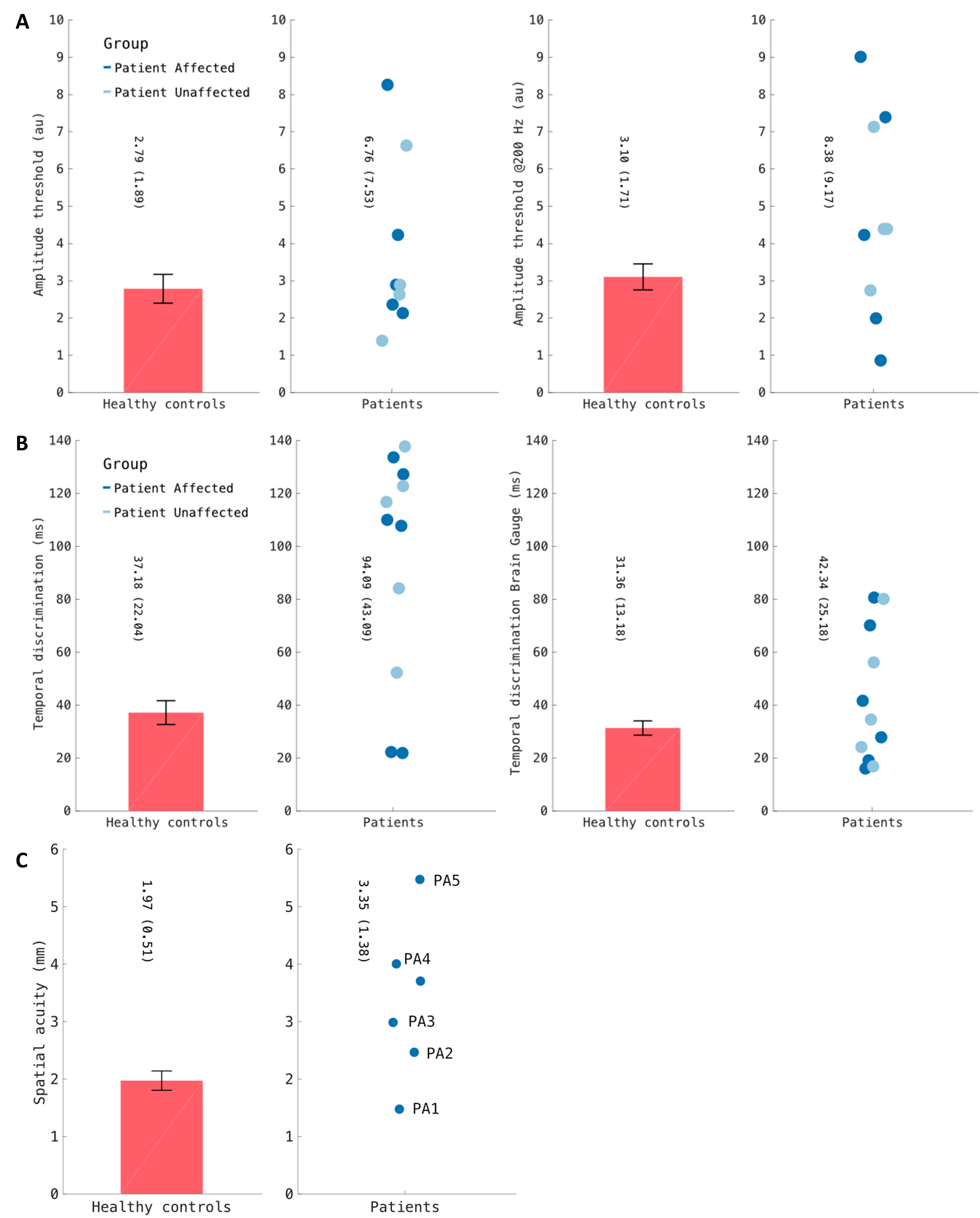
Behavioural: FHD patients had higher amplitude discrimination thresholds (31Hz HC:2.8±1.9, FHD:6.8±7.5; 200Hz HC:3.1±1.7, FHD:8.4±9.2, Fig.1A), TDT thresholds (piezos HC:37±22, FHD:94±43ms, Fig.1B) and GOT acuity (HC:2.0±0.5, FHD:3.3±1.4mm, Fig.1C) than HCs.
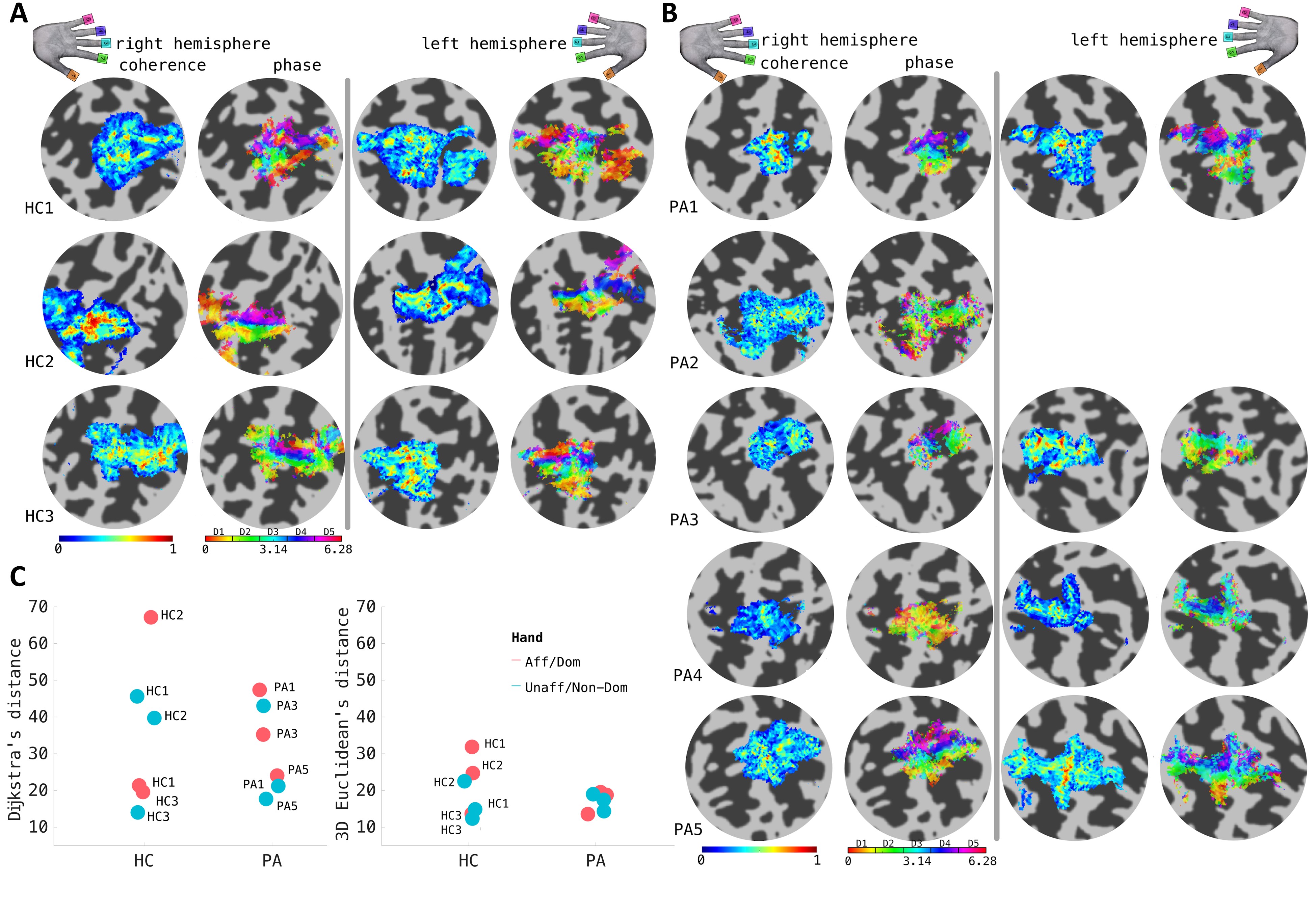
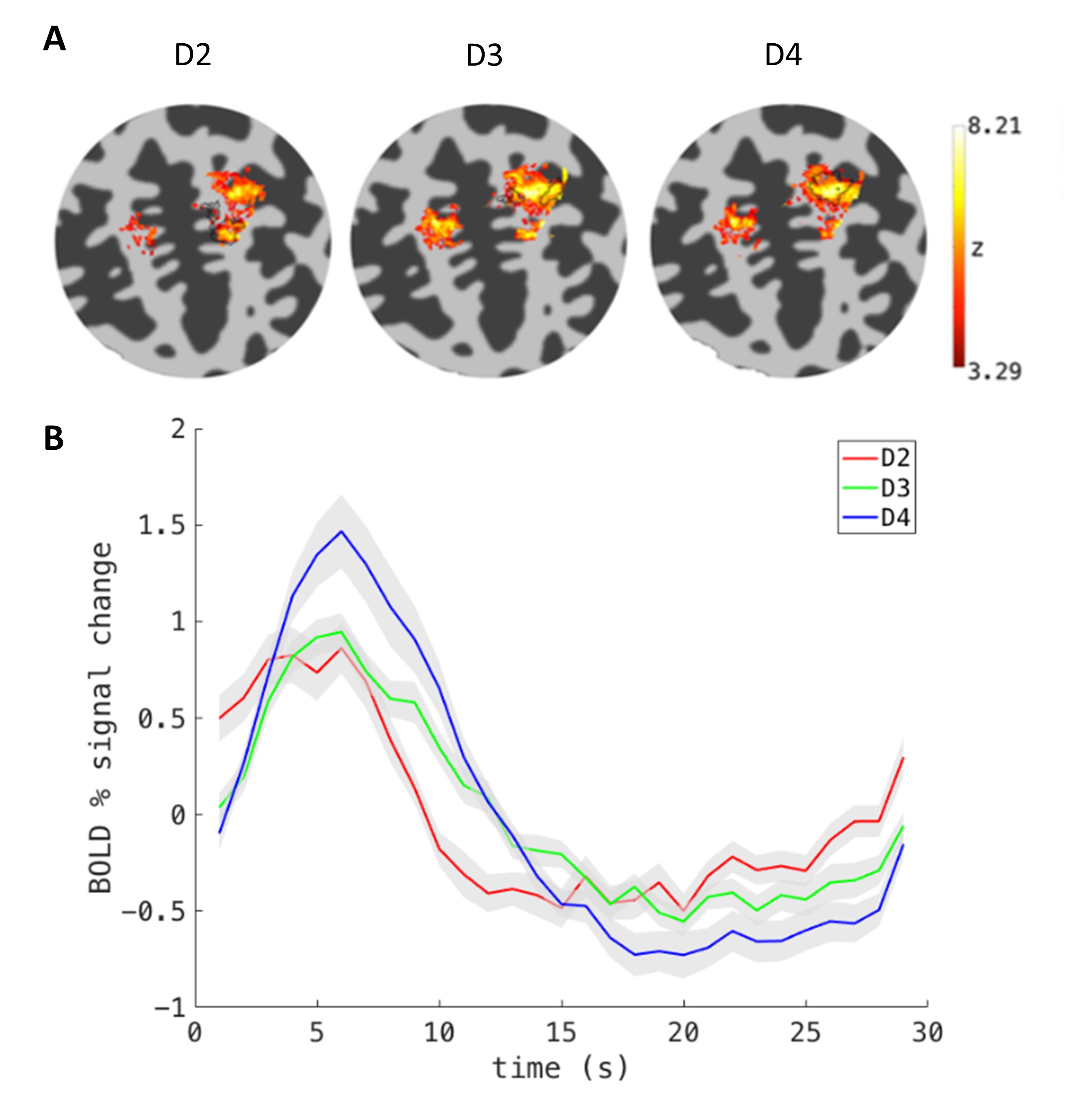
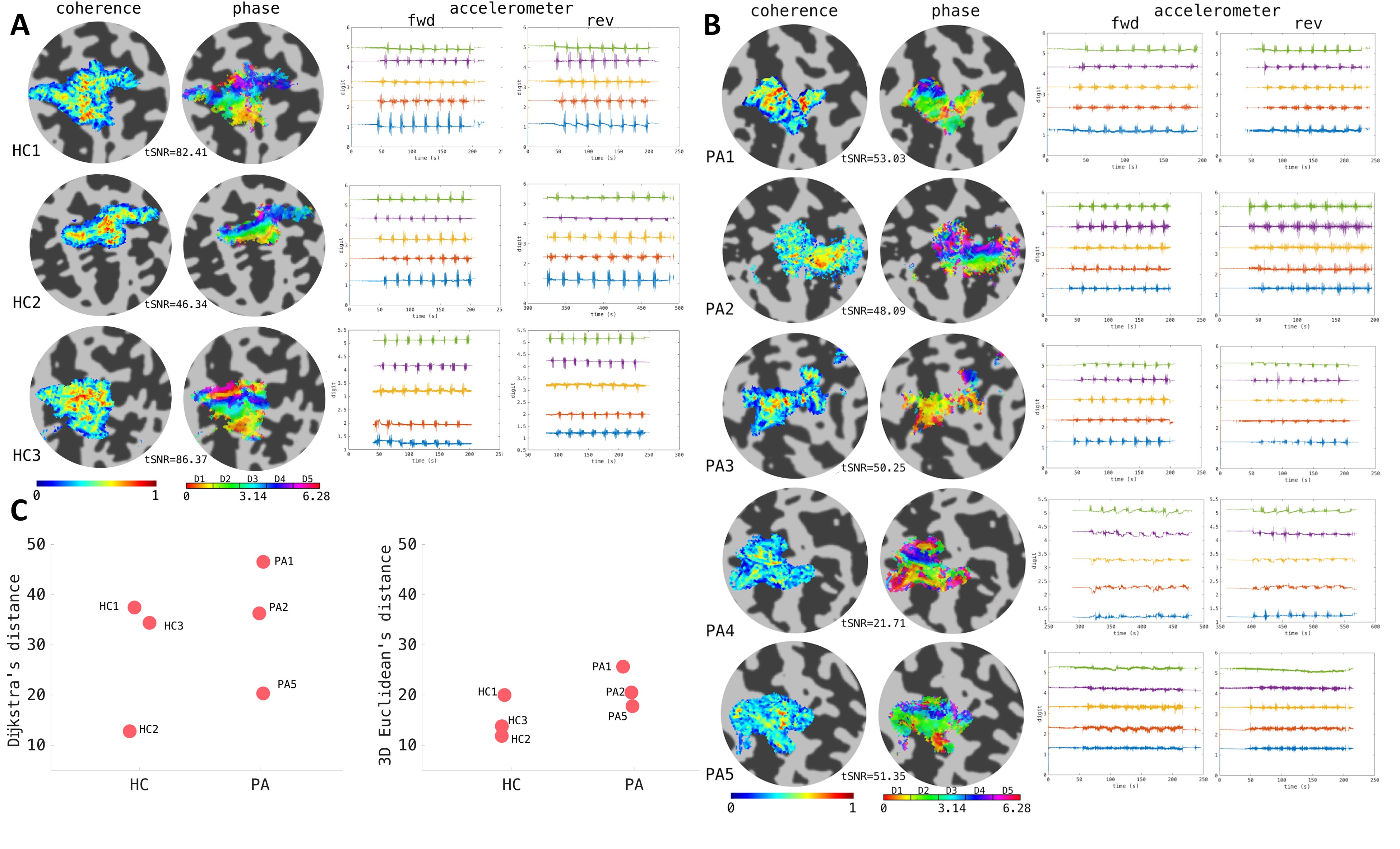
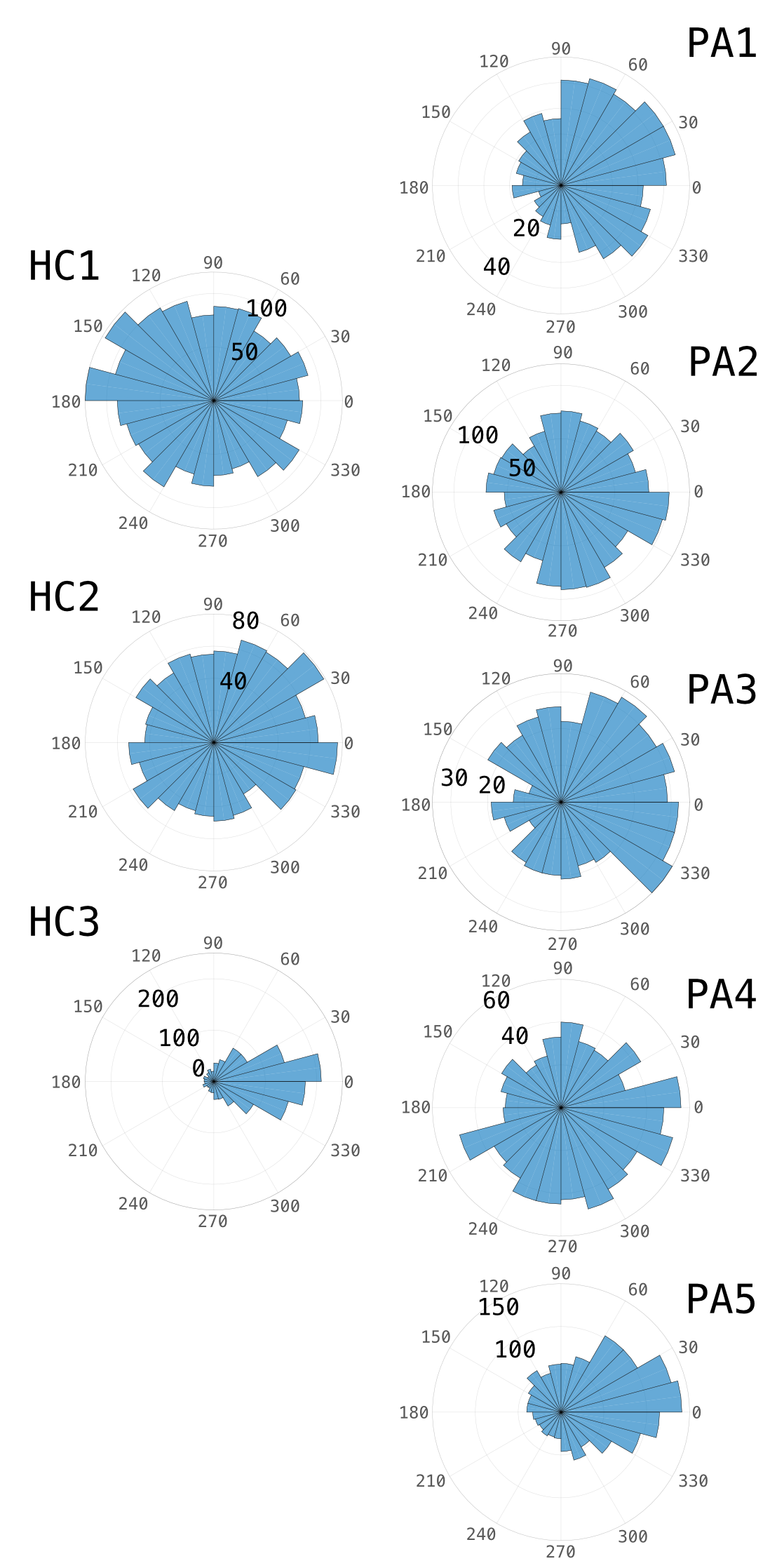
fMRI: Somatotopy coherence and phase maps are shown for HCs (Fig.2A) and FHD patients (Fig.2B) along with Dijkstra’s and 3D-Euclidean D1-D5 distance(Fig. 2C). All HCs showed clear somatotopic maps in the postcentral gyrus, S1, while only FHD patients PA1, PA3, and PA5 show clear maps. For the event-related paradigm (Fig.3), each digit produced significant activation but with little difference between HCs and FHD patients. Mototopy shows clear digit mapping in S1 for HCs (Fig.4A) with less apparent maps in the FHD patients (Fig.4B). Figure 5 shows the phase difference histograms in S1 between the somatotopy and mototopy.
Discussion
Behavioural measures of amplitude, temporal discrimination and spatial acuity were increased in FHD patients compared to HCs, consistent with literature7,8. Somatotopic and mototopic maps are presented, the accelerometer is used as an indicator of patient task compliance. The event-related paradigm showed that it was difficult to separate D2/D3/D4, but digit-specific HRFs could be obtained which could be used in somatosensory population receptive field (pRF) mapping10,11. In future, FHD patient data will be compared to a follow-up session 3 months post-Botox to determine the effects of treatment, by assessing the TW phase difference histogram between pre- and post-Botox.Conclusion
A standardised behavioural and fMRI battery has been developed in healthy controls and FHD patients to assess somatomotor function.Acknowledgements
This work was funded by the UK's Medical Research Council (MRC) grant code MR/M022722/1 and a Leverhulme fellowship to RSP.References
1. Sanchez-Panchuelo, R. et al. Regional structural differences across functionally parcellated Brodmann areas of human primary somatosensory cortex. NeuroImage. 2014;93:221-230.
2. Sengupta, A. et al. A Probabilistic Atlas of Digit Somatotopy in the Human Primary Somatosensory Cortex. Proc. Intl. Soc. Mag. Reson. Med. 2018; 26, abstract 0876
3. Besle, J. et al. Event‐related fMRI at 7T reveals overlapping cortical representations for adjacent fingertips in S1 of individual subjects. Hum. Brain Mapp. 2014;35(5):2027-2043.
4. Butterworth, S. et al. Abnormal cortical sensory activation in dystonia: An fMRI study. Mov. Disord. 2003;18(6):673-682.
5. Nelson, A.J. et al. Digit‐specific aberrations in the primary somatosensory cortex in Writer's cramp. Ann. Neurol. 2009;66(2):146-154.
6. Dresel, C. et al. Multiple changes of functional connectivity between sensorimotor areas in focal hand dystonia. J. Neurol. Neurosurg. Psychiatry. 2014;85(11):1245-1252.
7. Bara-Jimenez, W. et al. Sensory discrimination capabilities in patients with focal hand dystonia. Ann. Neurol. 2000;361-407.
8. Molloy, F. et al. Abnormalities of spatial discrimination in focal and generalized dystonia. Brain. 2003;126(10):2175-2182.
9. Brain Gauge. Cortical Metrics, Chapel Hill, NC, USA www.corticalmetrics.com
10. Asghar, M. et al. Using measured Haemodynamic Response Functions in Population Receptive Field mapping at 7 T. Proc. Intl. Soc. Mag. Reson. Med. 2018; abstract 0874
11. Asghar, M. Population Receptive Field Mapping of Human Somatosensory Cortex at 7 T. Proc. Intl. Soc. Mag. Reson. Med. 2017; abstract 0251
Figures