0353
Diffusion Tensor Imaging Tractography for Diagnosing Traumatic Brachial Plexus Root Avulsions: A Proof-of-Concept Study1Leeds Institute of Medical Research, University of Leeds, Leeds, United Kingdom, 2Department of Plastic and Recosntructive Surgery, Leeds Teaching Hospitals NHS Trust, Leeds, United Kingdom, 3Leeds Teaching Hospitals NHS Trust, Leeds, United Kingdom, 4Leeds Institute of Cardiovascular and Metabolic Medicine, University of Leeds, Leeds, United Kingdom, 5Advanced Imaging Centre, University of Leeds, Leeds, United Kingdom, 6Leeds Musculoskeletal Biomedical Research Unit, University of Leeds, Leeds, United Kingdom
Synopsis
Due to limitations in the accuracy of clinical MRI, adults with traumatic brachial plexus injuries (BPI) undergo major exploratory surgery to define their injury. Early exploration and reconstruction restores limb function and improves quality of life. Diffusion tensor imaging (DTI) tractography offers the potential to replace exploratory surgery by assessing the continuity of the roots of the brachial plexus. Twenty healthy adults were used for sequence development on a 3 Tesla system and the protocol validated on 12 patients with known patterns of BPI. DTI reliably reconstructs the normal and injured brachial plexus with high fidelity and superior diagnostic accuracy.
Background
Traumatic brachial plexus injuries (BPI) affect 1% of adults involved in major trauma1. Such injuries can result in permanent disability2–6, chronic pain7–9, psychological morbidity10, 11 and reduced quality of life2, 4, 12. Early reconstructive nerve surgery is associated with recovery of useful function and improved quality of life2, 3, 12, 13. MRI is the best indicator of BPI14, although its diagnostic accuracy is moderate at-best meaning that patients undergo major exploratory surgery or wait months for potential recovery. This study aimed to develop a novel sequence using diffusion tensor imaging (DTI) tractography, to visualise the normal and injured roots of the brachial plexus. The hypothesis was DTI could serve as a potential replacement for operative exploration or an adjunct diagnostic tool.Methods
Twenty asymptomatic healthy adults were recruited for sequence development. Twelve adults with known (operatively explored) patterns of unilateral traumatic brachial plexus root avulsions were recruited for technique validation. A Siemens Prisma (Siemens Healthcare GmBH, Erlangen, Germany) was used to acquire single-shot echo-planar imaging at 3 Tesla (20 directions, b1 0s/mm2, b2 1000 mm/s2, 2.5mm3, TE 66ms, TR 4300ms, 42 slices), to reconstruct the brachial plexus in 3D. Images were interpreted by an independent radiologist. Eigenvalues were calculated inline by the scanner, from the lateral recess of the vertebral foramen (where the root should be) from user-defined regions of interest Independent samples t-tests were used for comparisons.Results
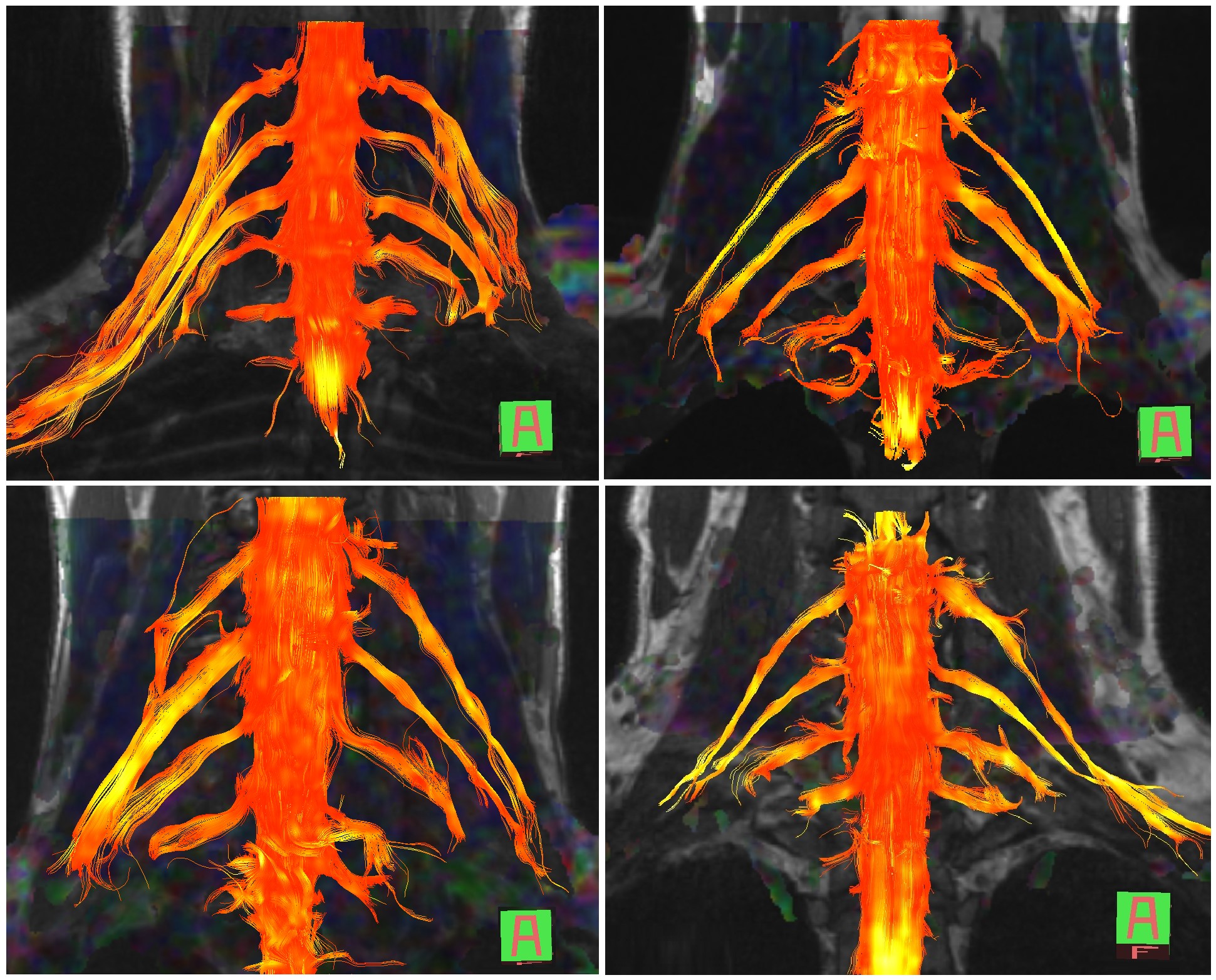
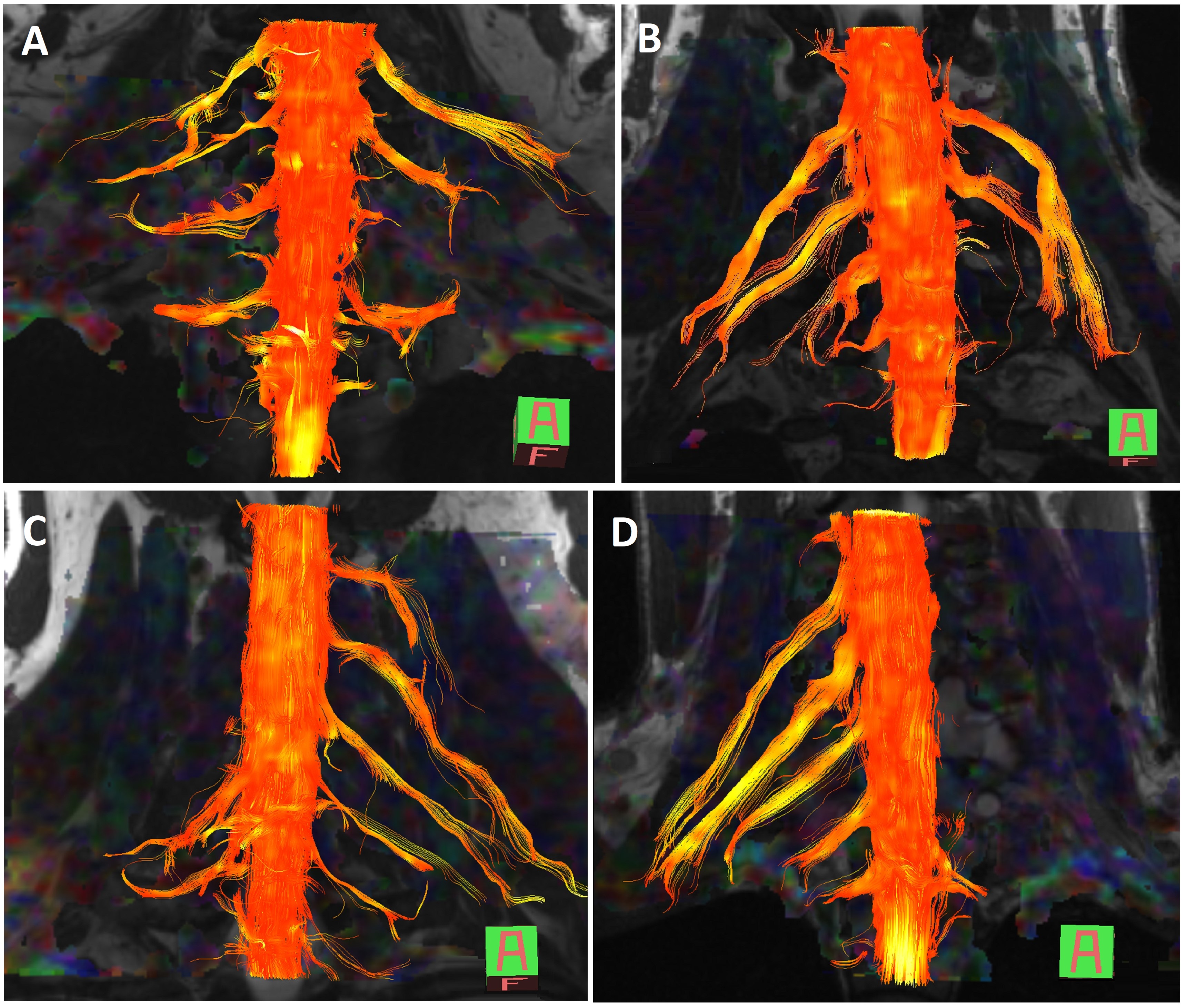
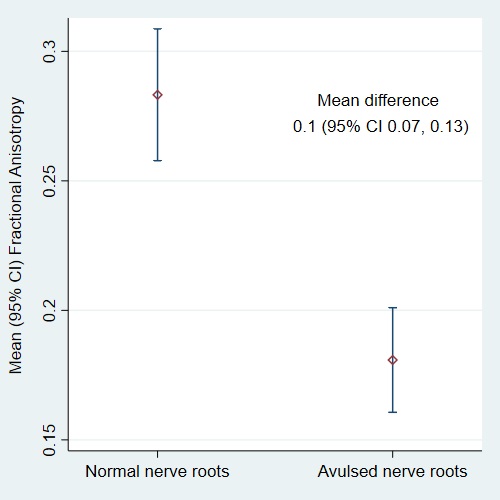
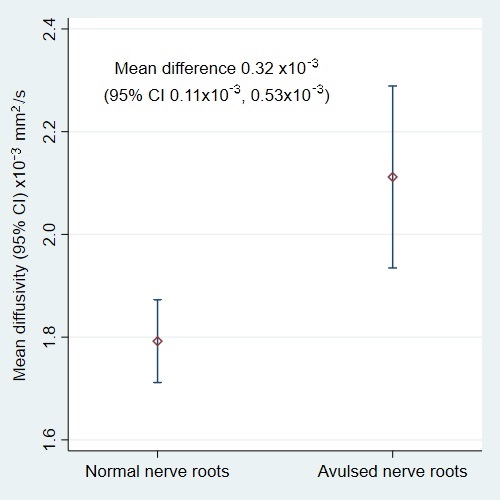
DTI tractography reconstructs the normal brachial plexus and root avulsions with high fidelity (Figures 1 and 2, respectively). Compared to healthy nerves roots, the fractional anisotropy (FA) of injured (avulsed) nerve roots was 10% lower (95% CI 7%, 13%; p<0.001; Figure 3) and the mean diffusivity (MD) was 0.32x10-3 mm2/s greater (95% CI 0.11x10-3, 0.53x10-3; p<0.001; Figure 4). The negative-predictive value of DTI for at least one root avulsion was 100% (95% CI 78, 100), with a specificity of 58% (95% CI 37%, 78%). DTI tractography was most sensitive to lower root avulsions (C7, C8 and T1; 89%, 100% and 100% respectively) but more specific for C5/6 avulsions (58% and 97%, respectively).Discussion
DTI tractography appears to reliably reconstruct the normal and injured brachial plexus. The FA values for normal and injured nerves are concordant with the literature although the MD of healthy nerves was greater than expected. This technique may protect patients from unnecessary exploratory surgery and conversely, may help to rapidly identify patients who need reconstructive surgery.Conclusions
The accuracy of this technique in acute injuries is currently being investigated through a multicentred diagnostic accuracy study funded by the National Institute for Health Research, recruiting patients from the North of England between 2018 and 2021.Acknowledgements
No acknowledgement found.References
1. The National Audit Office: Major Trauma Care in England, 2010
2. Franzblau LE, Shauver MJ, Chung KC: Patient Satisfaction and Self-Reported Outcomes After Complete Brachial Plexus Avulsion Injury. J Hand Surg Am 39:948–955.e4, 2014
3. Kretschmer T, Ihle S, Antoniadis G, et al: PATIENT SATISFACTION AND DISABILITY AFTER BRACHIAL PLEXUS SURGERY. Neurosurgery 65:A189–A196, 2009
4. Dolan RT, Butler JS, Murphy SM, et al: Health-related quality of life and functional outcomes following nerve transfers for traumatic upper brachial plexus injuries. J Hand Surg Eur Vol 37:642–51, 2012
5. Maldonado AA, Kircher MF, Spinner RJ, et al: Free Functioning Gracilis Muscle Transfer versus Intercostal Nerve Transfer to Musculocutaneous Nerve for Restoration of Elbow Flexion after Traumatic Adult Brachial Pan-Plexus Injury. Plast Reconstr Surg 138:483e–488e, 2016
6. Teixeira MJ, da Paz MG da S, Bina MT, et al: Neuropathic pain after brachial plexus avulsion - central and peripheral mechanisms. BMC Neurol 15:73, 2015
7. Lee KJ, Joo WI, Chough CK, et al: Long term effect of thalamic deep brain stimulation for pain due to brachial plexus injury. Stereotact Funct Neurosurg 90:161, 2012
8. Brill S, Aryeh IG: Neuromodulation in the management of pain from brachial plexus injury. Pain Physician 11:81–5, 2008
9. Teixeira MJ, da Paz MG da S, Bina MT, et al: Neuropathic pain after brachial plexus avulsion - central and peripheral mechanisms. BMC Neurol 15:73, 2015
10. Franzblau L, Chung KC: Psychosocial outcomes and coping after complete avulsion traumatic brachial plexus injury. Disabil Rehabil 37:135–143, 2015
11. Wilson TJ, Chang KWC, Yang LJ-S: Depression and Anxiety in Traumatic Brachial Plexus Injury Patients Are Associated With Reduced Motor Outcome After Surgical Intervention for Restoration of Elbow Flexion. Neurosurgery 78:844–850, 2016
12. Mancuso CA, Lee SK, Dy CJ, et al: Expectations and limitations due to brachial plexus injury: a qualitative study. Hand 10:741–749, 2015
13. Liu Y, Lao J, Gao K, et al: Functional outcome of nerve transfers for traumatic global brachial plexus avulsion. Injury 44:655–660, 2013
14. Vargas MI, Viallon M, Nguyen D, et al: New approaches in imaging of the brachial plexus. Eur J Radiol 74:403–410, 2010
Figures