0350
Cholesteatomas Detection using PSF-encoded EPI DWI1Center for Biomedical Imaging Research, Department of Biomedical Engineering, School of Medicine, Tsinghua University, Beijing, China, 2Philips Healthcare, Beijing, China, 3Department of Otorhinolaryngology, Peking Union Medical College Hospital, Beijing, China
Synopsis
DWI has proved to be valuable in detection of cholesteatoma, but there still remain challenges. Susceptibility artifacts and geometric distortions in single-shot EPI DWI affect the identification of subtle nidus. TSE-based DWI can reduce susceptibility-induced artifacts, but the disadvantages are SNR degradation and T2-blurring. In this work, point-spread-function (PSF) encoded EPI DWI was employed to overcome the aforementioned limitations for cholesteatomas detection. This technique has the capability to acquire high-quality, distortion- and blurring-free diffusion images with more accurate lesion boundary.
Introduction
Recent studies demonstrated that DWI has the ability to detect cholesteatoma, while there still remain challenges [1,2]. Single-shot EPI DWI is a fast diagnostic method, but susceptibility artifacts and geometric distortions severely affect the identification of cholesteatoma in the middle ear [3], where the susceptibility variations are dramatic. TSE-based DWI can mitigate susceptibility-induced artifacts, but the main drawbacks are SNR degradation and T2-blurring [4]. Recently, a fast distortion- and blurring-free imaging technique, termed “Tilted-CAIPI”, has been used to highly accelerate PSF-EPI for diffusion imaging [5]. In this study, we adopted the emerging technique for cholesteatoma detection.Methods
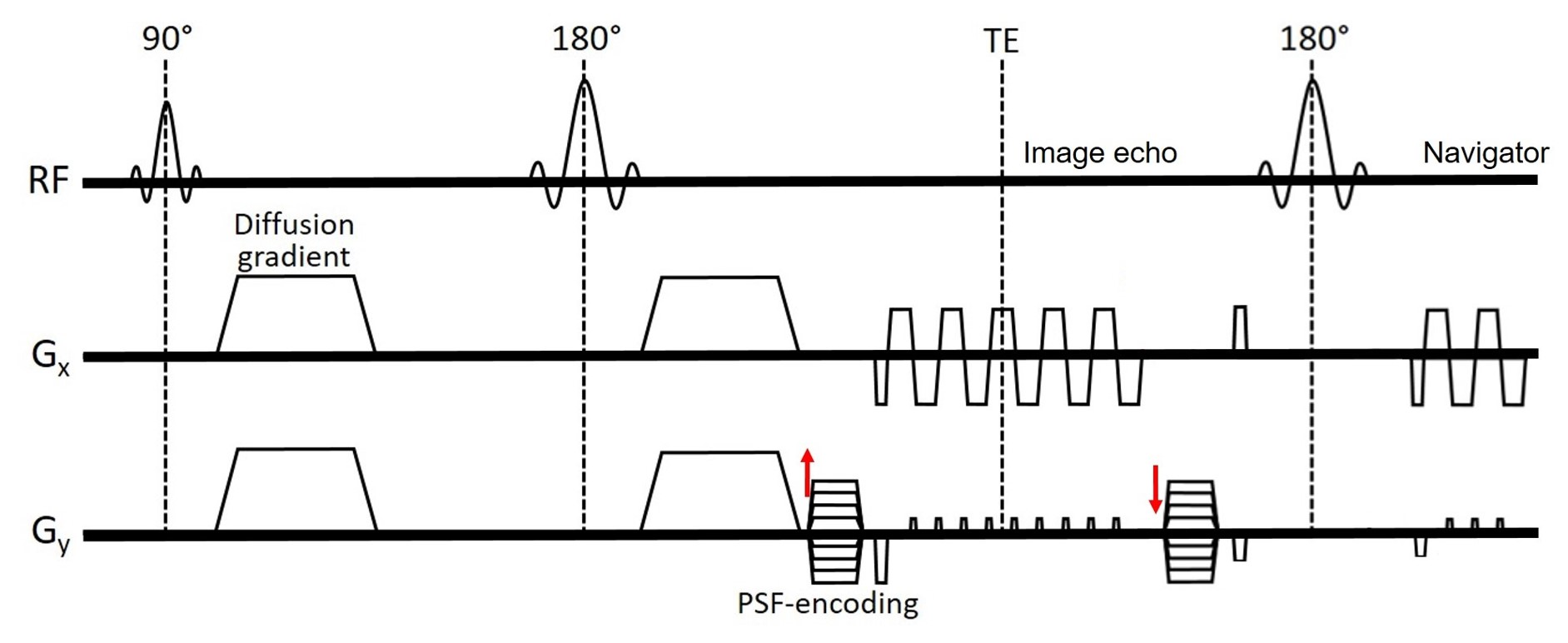
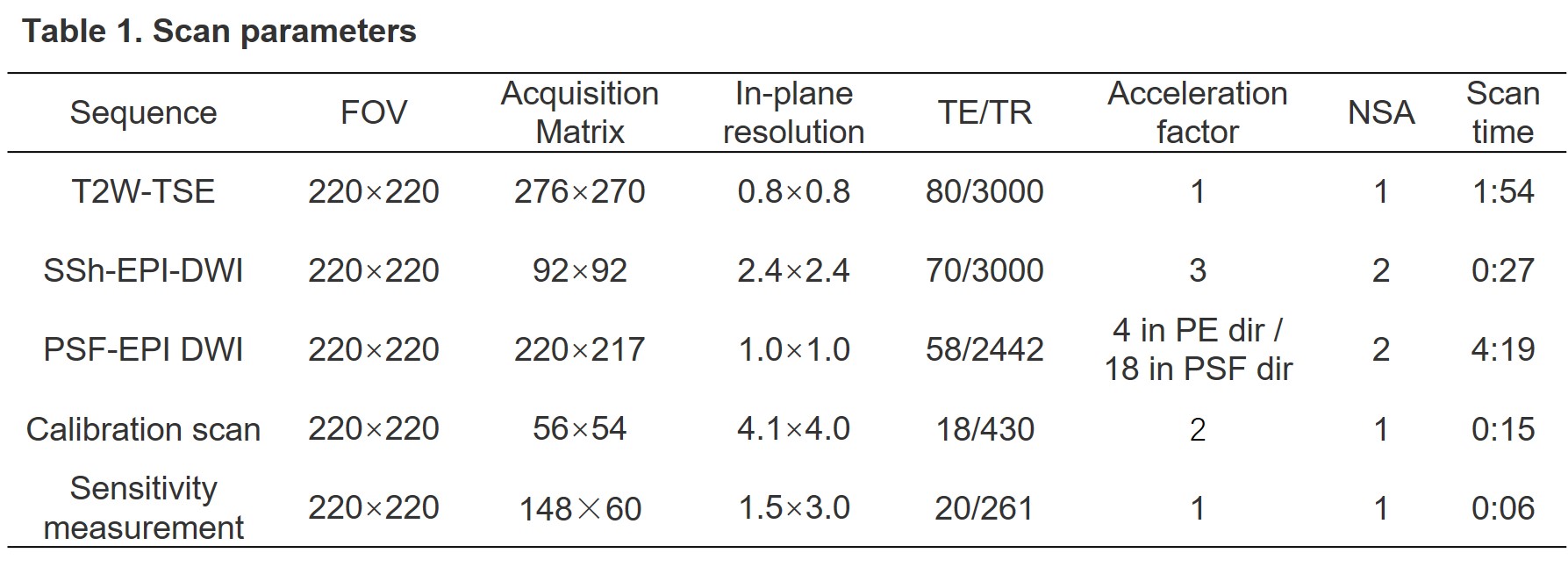
Under an IRB-approved protocol, two patients suspected of having cholesteatoma underwent preoperative MRI scan on a Philips Achieva 3.0T system (Philips, Best, The Netherlands) with a 32-channel head coil. Coronal diffusion weighted images (b value, 0 and 1000 s/mm2, 3 diffusion-encoding directions) were acquired using PSF-encoded EPI sequence (Fig. 1). Other imaging parameters were: FOV=220×220 mm2, matrix size= 220×217, in-plane resolution=1.0×1.0 mm2, TE/TR=58/2442ms, acceleration factor=4 in the PE direction, acceleration factor=18 in the PSF direction, 2 averages, the number of shots=13, scan time=4min40s (4min19s imaging scan + 21s calibration acquisition). 11 slices (no gap) with slice thickness of 3mm were used to cover the aural region. The DWI data were off-line reconstructed using the Tilted-CAIPI method [4]. Navigator information was used to correct for shot-to-shot phase variations. Besides, a single-shot EPI sequence was also used to acquire diffusion data with FOV=220×220 mm2, matrix size= 92×92, TE/TR=70/3000ms, SENSE=3, 2 averages, acquisition time=27s. In-plane resolution was 2.4×2.4 mm2, which was lower than that of PSF-EPI-DWI in order to reduce the geometric distortions. In addition, coronal TSE T2 weighted images at the same location were also obtained. FOV=220×220 mm2, in-plane resolution=0.8×0.8 mm2, TE/TR=80/3000ms, scan time=1min54s. The detailed scan parameters were listed in Table 1.
This study was approved by the Institutional Review Board and written informed consent was obtained from all the participants.
Results and Discussion
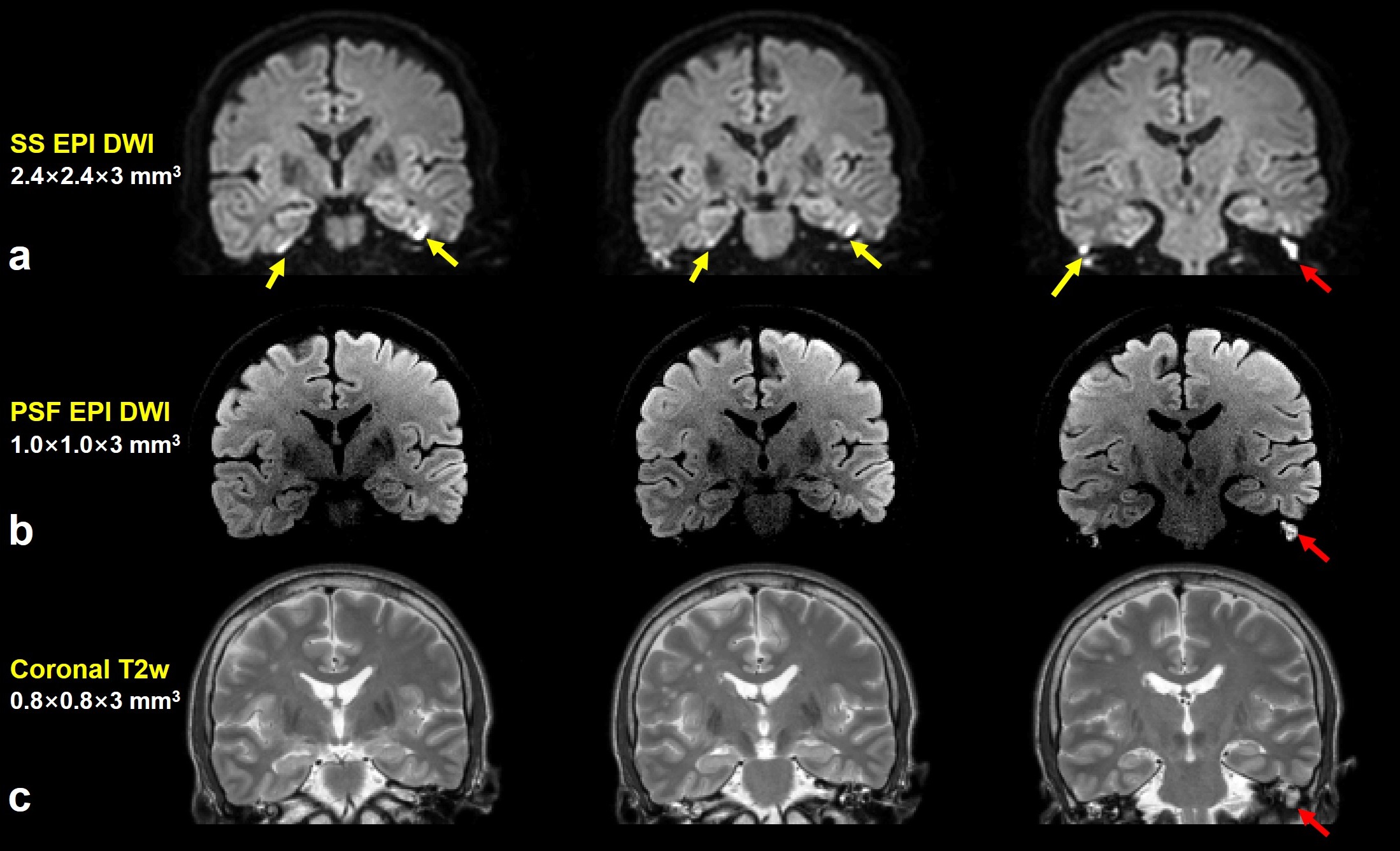
Three coronal slices of the T2 weighted images, single-shot EPI DWI, and PSF-encoded EPI DWI from one patient are shown in Fig. 2. There are multiple hyperintensities in the single-shot EPI diffusion images (Fig. 2a), which may provide false information and mislead the cholesteatoma detection due to the artifacts and distortions. Previous studies reported that cholesteatoma was diagnosed on DWI as a noticeable hyperintense signal in comparison with normal tissues [7-9]. Coil sensitivity correction was not conducted in PSF-encoded EPI DWI thus the central image looks dim. It is obvious that a marked hyperintensity is located at the left side of the middle ear in PSF-encoded EPI DWI (Fig. 2b), characterizing the lesion location accurately. The high-quality, distortion- and blurring-free diffusion weighted images are beneficial for cholesteatoma detection and diagnosis.
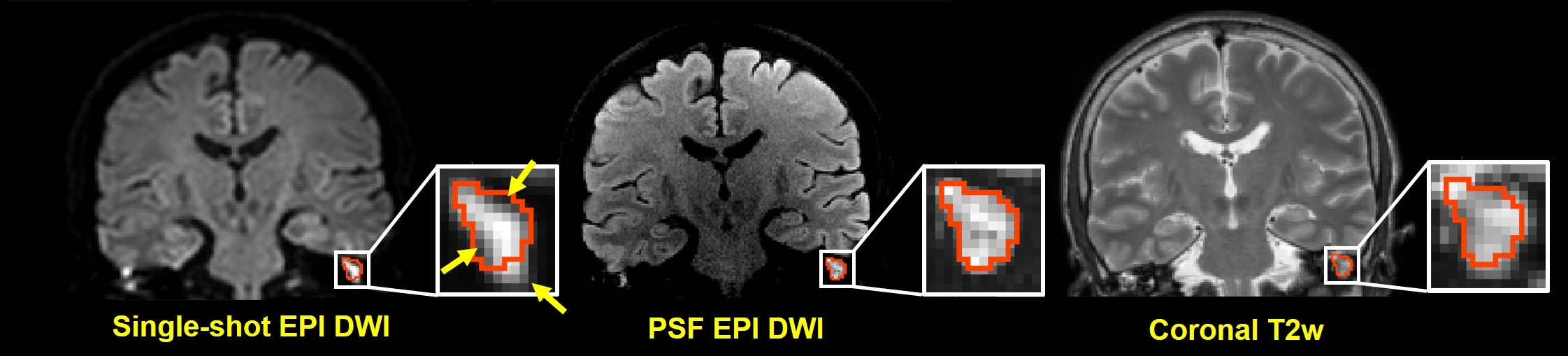
More detailed lesion boundary is presented in Fig. 3. The lesion contour extracted from T2W TSE image was overlaid on single-shot EPI DWI and PSF-encoded EPI DWI. Compared with single-shot EPI DWI, PSF-encoded EPI DWI can provide clearer lesion boundary without any distortion, and has higher diagnostic accuracy.
In this work, the resolution of single-shot EPI DWI (2.4×2.4 mm2) is lower than that of PSF-encoded EPI DWI (1.0×1.0 mm2). Acceleration factor of 3 was used to increase the bandwidth along the PE direction. Although only 31 phase-encoding lines were used in the single-shot EPI acquisition, there are still multiple artifacts in the ear canal due to severe susceptibility variations. Blurring degrades the image quality. The distortions and artifacts will become aggravated when higher spatial resolution is required. Therefore, single-shot EPI is not suitable for detection of small lesions in the middle ear cavity, while PSF-encoded EPI DWI provides better resolution without distortions.
In PSF-encoded EPI DWI, a longer examination time is required than in single-shot EPI, which is a limitation. In previous studies [3,9-11], TSE-based DWI is superior to single-shot EPI DWI in detecting cholesteatoma because of its ability to alleviate image distortion. However, in TSE DWI, the long echo train results in T2-blurring. If shortening the echo train by undersampling, SNR is sacrificed and long acquisition time is needed.
Conclusion
This study demonstrates the feasibility and advantage of PSF-encoded EPI DWI for cholesteatoma detection. The high-quality, distortion- and blurring-free diffusion weighted images are beneficial for detecting the cholesteatoma in the middle ear. They provided accurate lesion boundary to facilitate the subtle nidus detection. Further investigation will focus on the detection of smaller postoperative residual and recurrent cholesteatomas.Acknowledgements
No acknowledgement found.References
[1] Henninger, Benjamin, and Christian Kremser. "Diffusion weighted imaging for the detection and evaluation of cholesteatoma." World journal of radiology 9.5 (2017): 217.
[2] Vercruysse, Jean-Philippe, et al. "The value of diffusion-weighted MR imaging in the diagnosis of primary acquired and residual cholesteatoma: a surgical verified study of 100 patients." European radiology 16.7 (2006): 1461-1467.
[3] Schwartz, K. M., et al. "The utility of diffusion-weighted imaging for cholesteatoma evaluation." American Journal of Neuroradiology 32.3 (2011): 430-436.
[4] Hirata, Kenichiro, et al. "Comparison of the image quality of turbo spin echo-and echo-planar diffusion-weighted images of the oral cavity." Medicine 97.19 (2018).
[5] Dong, Zijing, et al. "Tilted‐CAIPI for highly accelerated distortion‐free EPI with point spread function (PSF) encoding." Magnetic resonance in medicine (2018).
[6] In, Myung-Ho, Oleg Posnansky, and Oliver Speck. "High-resolution distortion-free diffusion imaging using hybrid spin-warp and echo-planar PSF-encoding approach." Neuroimage 148 (2017): 20-30.
[7] Fitzek, Clemens, et al. "Diffusion-weighted MRI of cholesteatomas of the petrous bone." Magnetic Resonance in Medicine 15.6 (2002): 636-641.
[8] Vercruysse, J. Ph, et al. "Magnetic resonance imaging of cholesteatoma: an update." B-ENT 5.4 (2009): 233-240..
[9] De Foer, Bert, et al. "Detection of postoperative residual cholesteatoma with non-echo-planar diffusion-weighted magnetic resonance imaging." Otology & Neurotology 29.4 (2008): 513-517
[10] Elefante, Andrea, et al. "Diffusion weighted MR imaging of primary and recurrent middle ear cholesteatoma: an assessment by readers with different expertise." BioMed research international 2015 (2015).
[11] De Foer, Bert, et al. "Middle Ear Cholesteatoma: Non–Echo-planar Diffusion-weighted MR Imaging versus Delayed Gadolinium-enhanced T1-weighted MR Imaging—Value in Detection." Radiology 255.3 (2010): 866-872.
[12] Lehmann, P., et al. "3T MR imaging of postoperative recurrent middle ear cholesteatomas: value of periodically rotated overlapping parallel lines with enhanced reconstruction diffusion-weighted MR imaging." American Journal of Neuroradiology 30.2 (2009): 423-427.
Figures