0343
Evaluating microstructure of the corticospinal tract in normal pressure hydrocephalus with diffusion MRI using oscillating gradient spin-echo1Radiology, Juntendo University School of Medicine, Tokyo, Japan, 2Radiology, Graduate School of Medicine, The University of Tokyo, Tokyo, Japan, 3Radiological Sciences, Graduate School of Human Health Sciences, Tokyo Metropolitan University, Tokyo, Japan, 4Neurosurgery, Juntendo University School of Medicine, Tokyo, Japan, 5Neurosurgery, Juntendo Tokyo Koto Geriatric Medical Center, Tokyo, Japan, 6Siemens Healthcare K.K., Tokyo, Japan
Synopsis
We evaluated the corticospinal tract (CST) of normal pressure hydrocephalus (NPH) patients using the oscillating gradient spin-echo (OGSE) method. Diffusion time can be reduced greatly with OGSE and properties of the microstructure can be evaluated in more detail by collecting data using multiple diffusion times. The diffusivity of the CST increased and the diffusion time dependence was small in NPH patients compared with healthy controls. It is possible to estimate the structural change of CST in NPH by using multiple diffusion times with OGSE.
INTRODUCTION
Diffusion MRI with oscillating gradient spin-echo (OGSE, prototype sequence) applies waveform or oscillated trapezoidal motion probing gradient and greatly reduces diffusion time compared with conventional pulsed gradient spin-echo method1-3. Properties of the microstructure can be evaluated in more detail by collecting data using multiple diffusion times. Normal pressure hydrocephalus (NPH) is a clinical condition with enlargement of the ventricle without increasing cerebrospinal fluid pressure4,5. Previous studies using diffusion tensor imaging reported that fractional anisotropy and apparent diffusion coefficient increased in the corticospinal tract (CST) of NPH patients6,7. These changes were presumed to be due to compression of CST by the enlarged lateral ventricle. The purpose of this study was to evaluate the CST of NPH patients using the OGSE method.METHODS
Nine patients with NPH (mean age 78.1 years, range 67–89 years), and 10 age-matched healthy volunteers (mean age 74.8 years, range 70–80 years) were included in this study. Diffusion MRI data were obtained with a 3T MRI scanner (MAGNETOM Prisma, Siemens Healthcare GmbH, Erlangen, Germany) using b-values of 0 and 800 s/mm2 with six directions. OGSE with a trapezoid-cosine waveform was performed with an effective diffusion time of 6.5 ms (frequency = 30 Hz), 9.3 ms (20Hz) and 35.2 ms (0Hz). Other parameters for acquisition were as follows: repetition time = 7800 ms; echo time = 168 ms; field of view = 164 × 164 mm2; matrix size = 82 × 82; slice thickness = 5 mm. The diffusion tensor of the CST was estimated and tractography was performed by using TrackVis 0.6.1 (www.trackvis.org). The height from the superior longitudinal fasciculus to the foramen of Monro level was set as the volume of interest (VOI) of upper CST and the height from the foramen of Monro to the cerebral peduncle was set as the VOI of lower CST (Figure 1). Axial, radial and mean diffusivity (AD, RD, MD) were calculated and the changes due to the difference in diffusion time were measured for each value.RESULTS
The measurement results are shown in Table 1. In the upper CST, AD, RD and MD measured at 0 Hz were higher in NPH patients than in controls. The diffusivity increased with shorter diffusion time and the change rate between 0 Hz and 30 Hz was significantly smaller in AD (+ 12.6% vs + 8.9%), RD (+ 22.9% vs + 16.5%) and MD (+ 16.9% vs + 12.0%) in NPH patients than in controls (Figure 2). In the lower CST, there was no significant difference in the diffusivity between NPH patients and controls, and there was no significant difference in the change rate.DISCUSSION
In the present study, the diffusivity of the CST increased and the diffusion time dependence was small in NPH patients compared with healthy controls. Increasing diffusivity at the upper CST of NPH is consistent with previous studies. According to a study examining the relationship between cerebral infarction and diffusion time, the diffusivity decreased with infarction, and changes in diffusivity due to changes in diffusion time were greater8,9. In the CST of NPH, the time dependence of AD was smaller than that of controls and this change is opposite to the change of cerebral infarction. This result seems to enhance the hypothesis that nerve fibers are compressed and stretched straight in NPH.CONCLUSION
It is possible to estimate the structural change of CST in NPH by using multiple diffusion times with OGSE.Acknowledgements
This work was supported by JSPS KAKENHI Grant Number 17K16486, the program for Brain Mapping by Integrated Neurotechnologies for Disease Studies (Brain/MINDS) from Japan Agency for Medical Research and development, AMED, and in part by a High Technology Research Center Grant from the Ministry of Education, Culture, Sports, Science, and Technology of Japan (MEXT).References
1. Martin M. Measuring restriction sizes using diffusion weighted magnetic resonance imaging: a review. Magn Reson Insights. 2013;6:59-64.
2. Wu D, Martin LJ, Northington FJ, et al. Oscillating gradient diffusion MRI reveals unique microstructural information in normal and hypoxia-ischemia injured mouse brains. Magn Reson Med. 2014;72(5):1366-1374.
3. Does MD, Parsons EC, Gore JC. Oscillating gradient measurements of water diffusion in normal and globally ischemic rat brain. Magn Reson Med. 2003;49(2):206-215.
4. Adams RD, Fisher CM, Hakim S, et al. Symptomatic occult hydrocephalus with "normal" cerebrospinal-fluid pressure. A treatable syndrome. N Engl J Med. 1965;273:117-126.
5. Hakim S, Adams RD. The special clinical problem of symptomatic hydrocephalus with normal cerebrospinal fluid pressure. Observations on cerebrospinal fluid hydrodynamics. J Neurol Sci. 1965;2(4):307-327.
6. Assaf Y, Ben-Sira L, Constantini S, et al. Diffusion tensor imaging in hydrocephalus: initial experience. AJNR Am J Neuroradiol. 2006;27(8):1717-1724.
7. Hattori T, Yuasa T, Aoki S, et al. Altered microstructure in corticospinal tract in idiopathic normal pressure hydrocephalus: comp. AJNR Am J Neuroradiol. 2011;32(9):1681-1687.
8. Baron CA, Kate M, Gioia L, et al. Reduction of Diffusion-Weighted Imaging Contrast of Acute Ischemic Stroke at Short Diffusion Times. Stroke. 2015;46(8):2136-2141.
9. Boonrod A, Hagiwara A, Hori M, et al. Reduced visualization of cerebral infarction on diffusion-weighted images with short diffusion times. Neuroradiology. 2018;60(9):979-982.
Figures
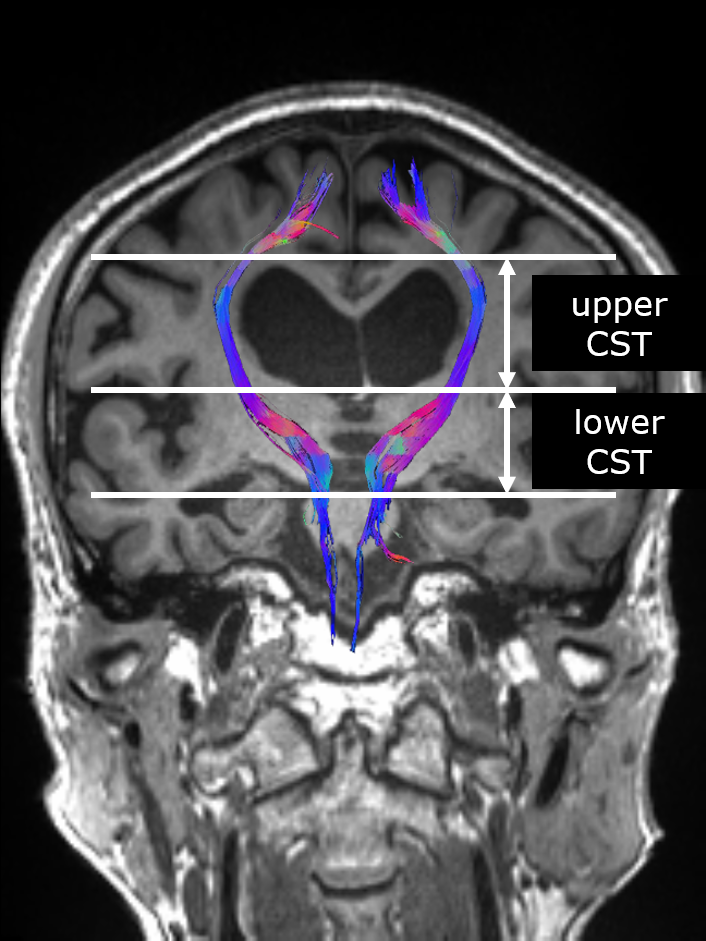
Figure 1. Tractography of the corticospinal tract on the T1-weighted coronal image.
The height from the superior longitudinal fasciculus to the foramen of Monro level was set as the volume of interest (VOI) of upper CST and the height from the foramen of Monro to the cerebral peduncle was set as the VOI of lower CST.
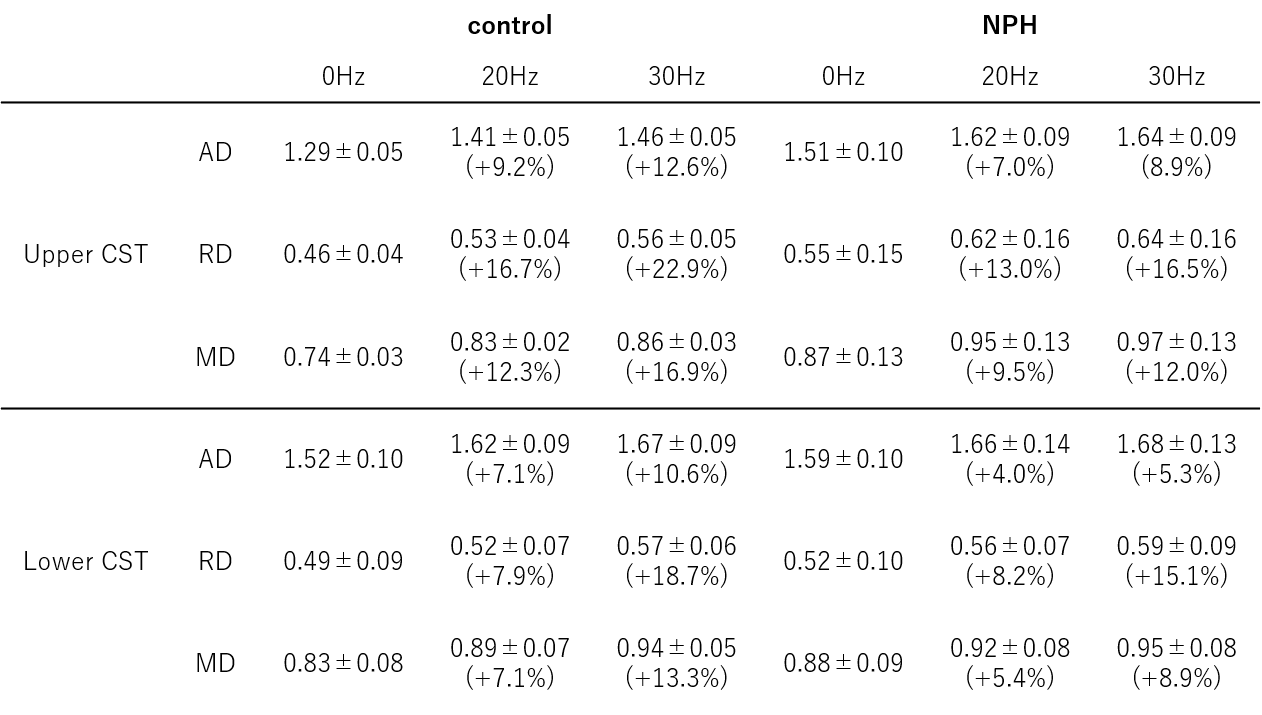
Table 1. The measurement results of diffusivity in the corticospinal tract.
The values represent mean±SD (10-3mm2/s). The value in parentheses is the ratio to the value of 0Hz. NPH = normal pressure hydrocephalus, CST = corticospinal tract, AD = axial diffusivity, RD = radial diffusivity, MD = mean diffusivity
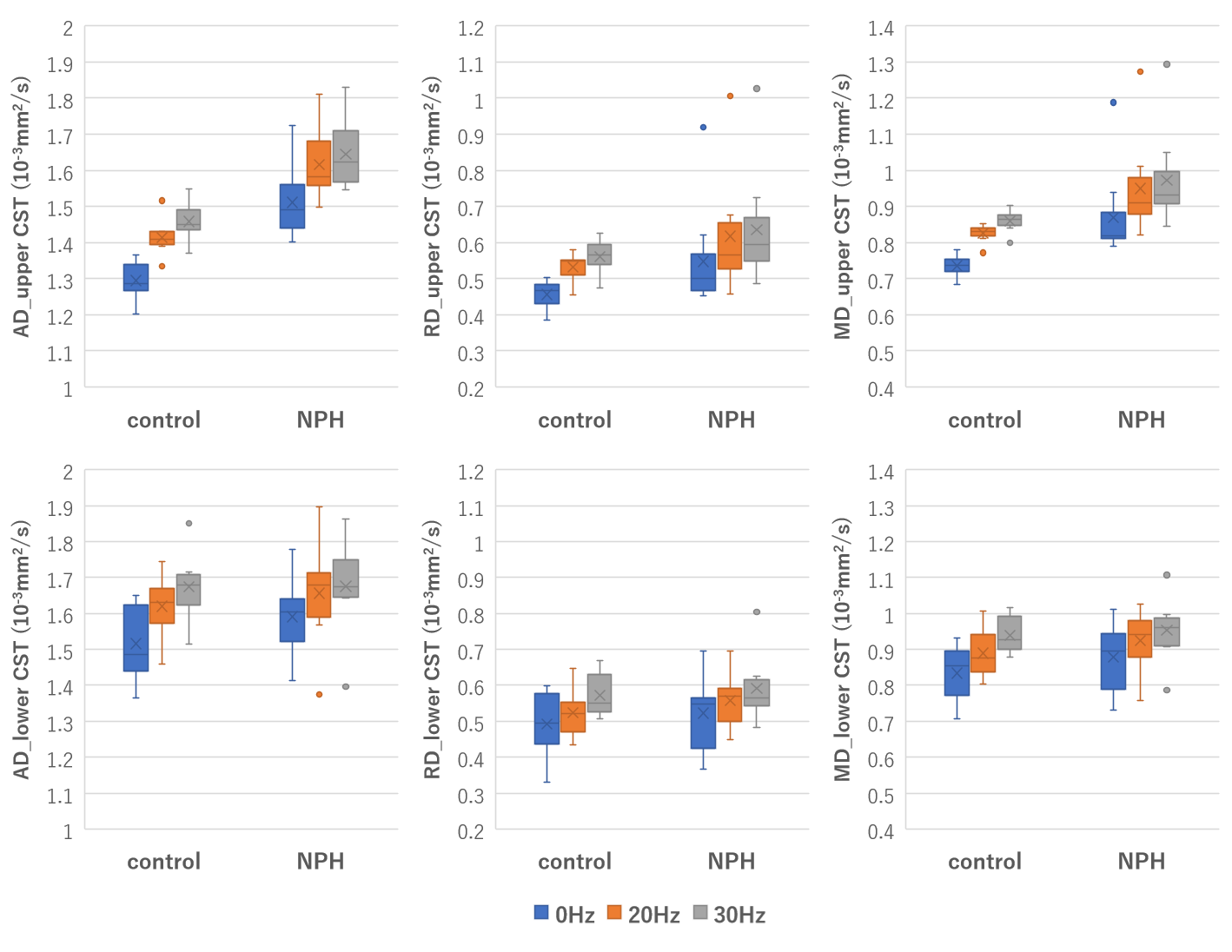
Figure 2. Boxplots of the axial, radial and mean diffusivity in the upper and lower CST at each frequency.
The diffusivity of the upper CST increased and the diffusion time dependence was small in NPH patients compared with healthy controls. In the lower CST, there was no significant difference in the diffusivity between NPH patients and controls, and there was no significant difference in the change rate due to difference in diffusion time.