0316
Single Breath-Hold T2 Quantification utilizing a Spiral Multi-Contrast TSE Sequence1Center for Magnetic Resonance Research, Department of Radiology, University of Minnesota, Minneapolis, MN, United States
Synopsis
A single breath-hold multi-contrast TSE sequence with spiral k-space sampling is introduced for T2 quantification. Sparsity constraint image reconstruction was applied to reconstruct undersampled datasets acquired under single breath-holding. The feasibility of the proposed sequence and image reconstruction were tested in brain and thoracic imaging for normal volunteers. The proposed method achieved T2 quantification of the thoracic region without clear cardiac motion artifacts.
Purpose
T2 contrast is widely used to differentiate lesions from normal tissues for various disorders in clinical diagnosis. While T2 quantification provides valuable information about the tissue properties, it is challenging in thoracic imaging, where it suffers from severe respiratory and cardiac motion and strong susceptibility effects in the air-tissue interface. In this study, we introduce a single breath-hold multi-contrast TSE sequence with spiral k-space sampling for T2 quantification. Spiral sampling trajectory achieves more efficient k-space sampling than conventional Cartesian sampling, which enabled the single breath-holding scan. Additionally, spiral sampling minimized cardiac motion artifacts due to its known insensitivity to motion. The feasibility of the proposed method was tested in brain and thoracic imaging of normal volunteers.Methods
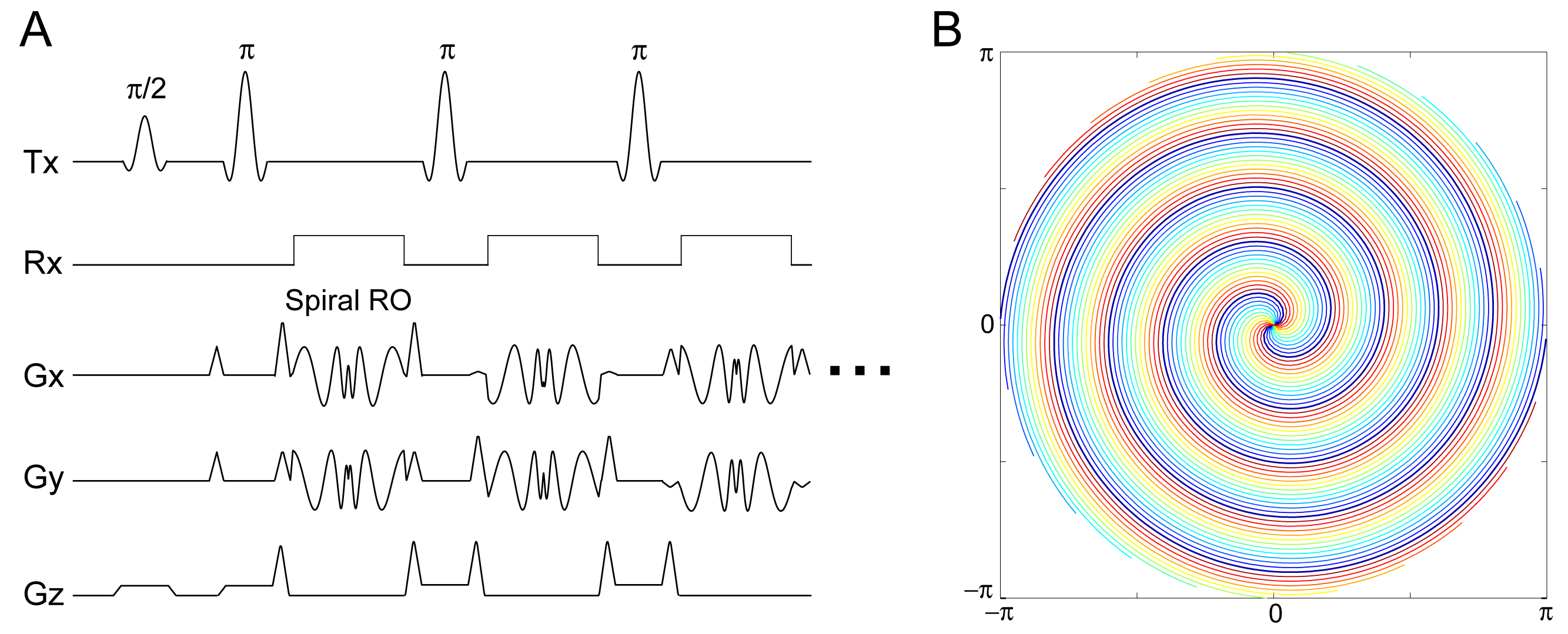
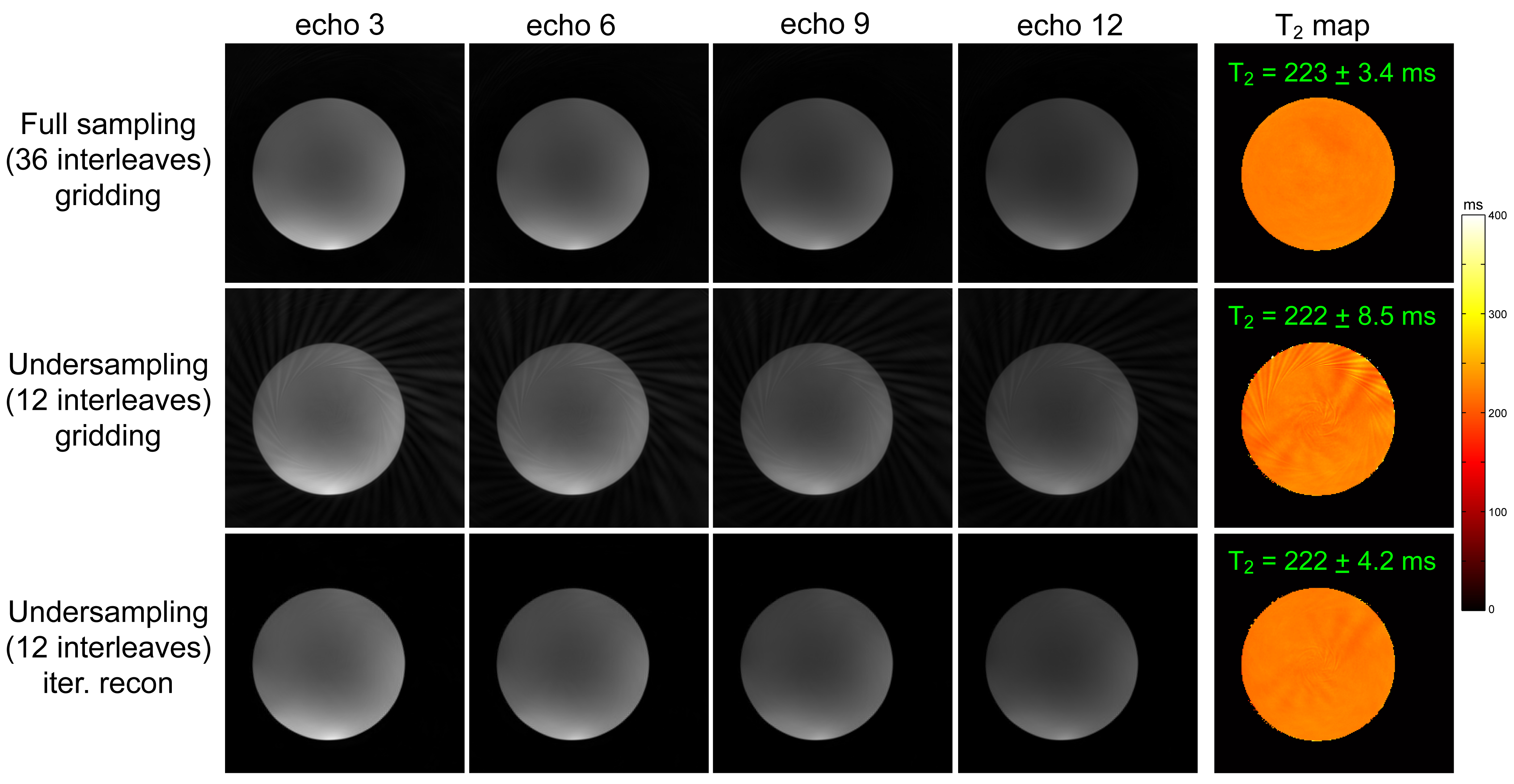
MR imaging was performed with a 3T Siemens Prisma MRI scanner. A sequence diagram of the proposed multi-contrast TSE sequence is shown in Fig.1a. Each readout traverses a spiral-in and -out trajectory in k-space (Fig.1b). Because only a limited amount of data can be acquired in a single breath-hold scan (usually 15-25 sec), iterative reconstruction with sparsity constraints was implemented. Sparsity constraints were applied by wavelet thresholding in the spatial domain and a low rank constraint with nuclear norm thresholding in the multi-contrast (TE) domain (1). To test the proposed sequence and image reconstruction, a phantom measurement was conducted. The capability of scan acceleration/undersampling was studied with two datasets of 36 spiral interleaves (full sampling) and 12 interleaves (undersampling). Sequence parameters for the phantom scan were: TR = 2 sec, echo spacing (esp) = 11.8 ms, echo train length (etl) = 12, 1.14 mm in-plane resolution, slice thickness = 5 mm and scan time (TA) = 76/26 sec for 36/12 interleaves. A T2 map was estimated by fitting the single exponential model, S(TE)=exp(−TE/T2), to the signal intensity decay of the reconstructed images in the least squares method.
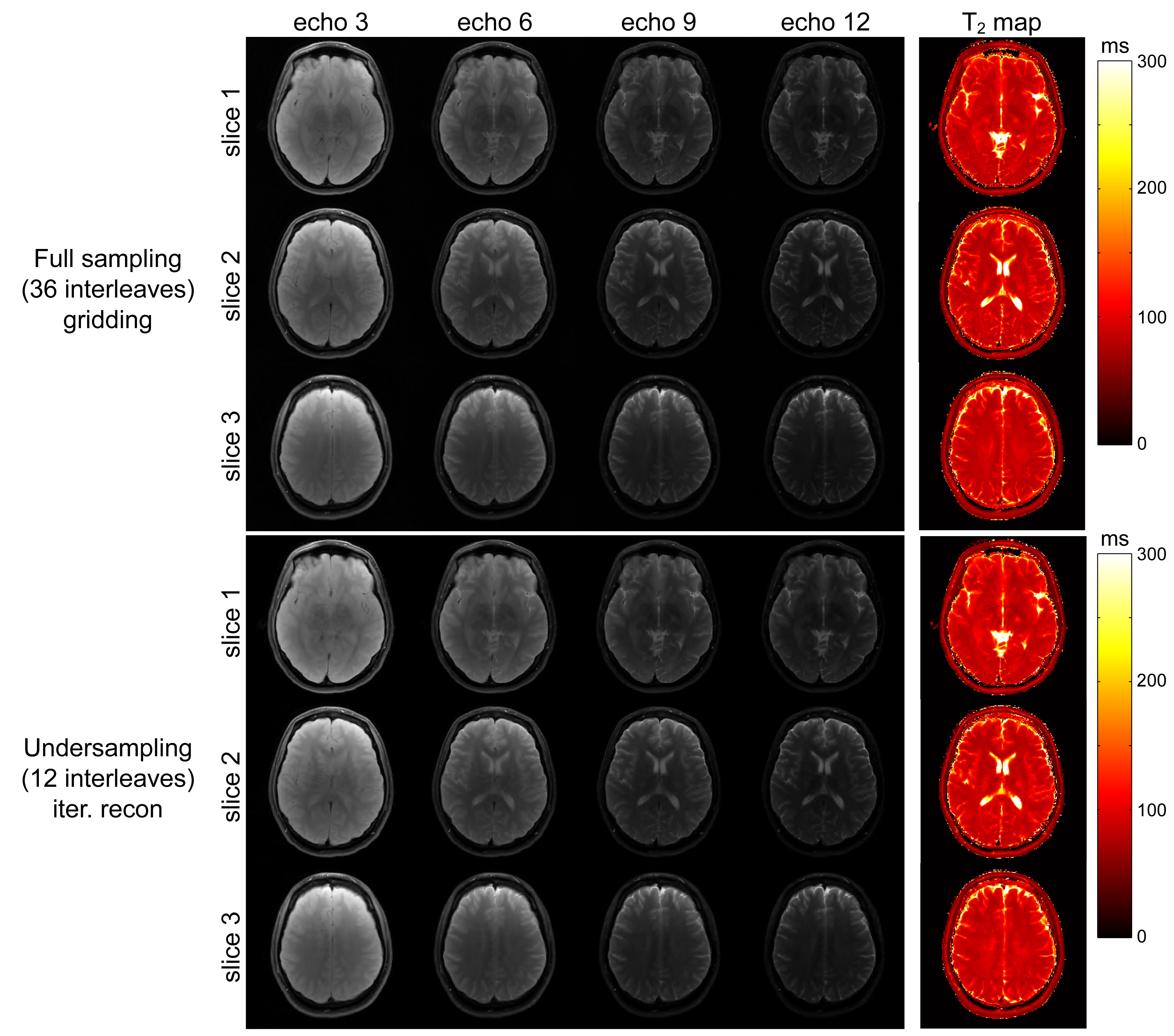
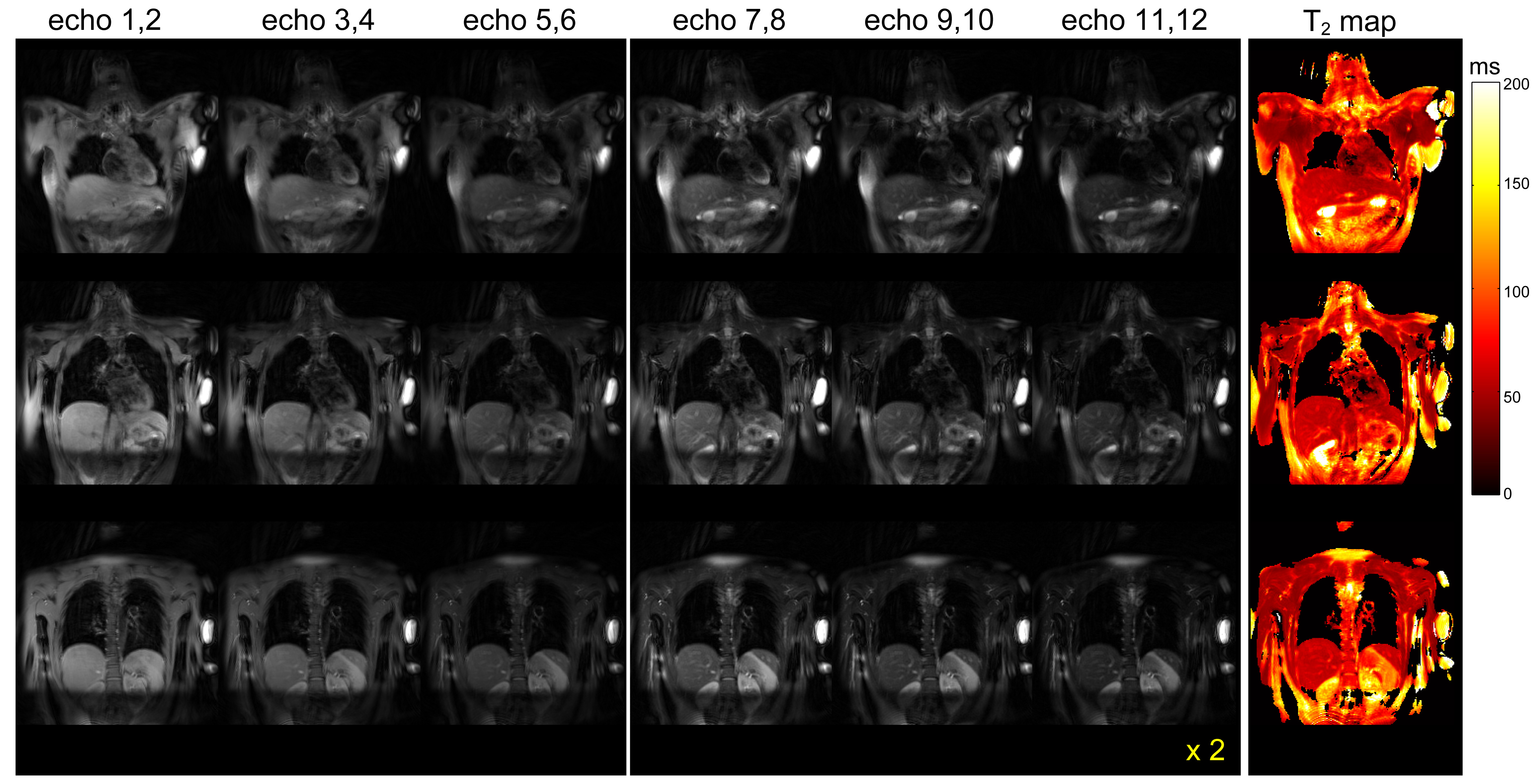
Normal volunteer scans were performed under an IRB approved protocol. In brain imaging, full sampling (36 interleaves) and undersampling (12 interleaves) datasets were acquired for comparison. Sequence parameters for brain imaging were: TR = 2 sec, esp = 13 ms, etl = 12, 1.14 mm in-plane resolution, slice thickness = 5 mm, TA = 76/26 sec for 36/12 interleaves. In thoracic imaging, an undersampling dataset (12 interleaves) was acquired due to the time limitation of single breath holding. Thoracic imaging parameters were: TR = 1.4 sec, esp = 11.2 ms, etl = 12, 2.2 mm in-plane resolution and slice thickness = 10 mm. To make breath holding doable without much difficulty, TR was cut down to 1.4 sec, which resulted in a scan time of 18 sec. Although spiral sampling is tolerant to motion artifacts due to repeated sampling of the k-space center region, 12 spiral interleaves were not always sufficient to avoid cardiac motion artifacts. Therefore, in thoracic image reconstruction, 6 images were reconstructed from the 12 echo data by combining adjacent two echoes (e.g. echo 1 and 2).
Results
In phantom measurements, the images and T2 map obtained from the undersampled data with gridding reconstruction showed undersampling/aliasing artifacts, whereas sparsity constrained reconstruction produced images with almost complete absence of those artifact and that are nearly indistinguishable from images reconstructed from fully sampled data (Fig.2). In brain imaging, the sparsity constraint reconstruction of the undersampled dataset also provided images and T2 maps consistent with those reconstructed from full sampling dataset (Fig.3). In thoracic imaging, there were no clear motion artifacts in the reconstructed images even without cardiac gating (Fig.4).Discussion
One potential application of the proposed method is to characterize indeterminate lung nodules. In lung cancer diagnosis, T2 quantification can be one useful marker to differentiate benign and malignant lung nodules (2). Clinically relevant lung nodules are typically of a size of 8 mm or greater in diameter. Considering the resolution and image quality achieved in this study, it would be promising to quantify T2 values of the clinically relevant nodules. One potential difficulty in patient exams is the lower breath holding capability of patients, since they may usually have a reduced lung function compared to normal subjects. The ability to characterize the clinically relevant lung nodules with the proposed method needs to be elucidated in future patient studies.Conclusions
The single breath-hold multi-contrast TSE sequence with spiral k-space sampling achieved T2 quantification of the thoracic region without clear cardiac motion artifacts.Acknowledgements
This study was supported by NIH grant P41EB015894 and 1S10OD017974-01.References
1. Zhang T, Pauly JM, Levesque IR. Accelerating parameter mapping with a locally low rank constraint. Magnetic resonance in medicine. 2015;73(2):655-61.
2. Kurihara Y, Matsuoka S, Yamashiro T, et al. MRI of pulmonary nodules. AJR American journal of roentgenology. 2014;202(3):W210-6.
Figures