0305
Establishing a Relationship Between Pain and Spinal Cord Demyelination using Magnetization Transfer Imaging and Thermal Sensory Testing1Department of Anesthesiology, Critical Care and Pain Medicine, Boston Children's Hospital, Boston, MA, United States, 2Department of Neurology, Boston Children's Hospital, Boston, MA, United States
Synopsis
Myelitis is a demyelinating disorder of the spinal cord . It can occur as an isolated syndrome or in the context of an autoimmune condition such as MS. Pain is a significant problem in myelitis and has a major impact on treatment response and rehabilitation efforts. Magnetization Transfer Imaging has the ability to provide a marker for myelin content. Defining a relationship between pain and demyelination could lead to improved disease outcome. Our results showed significant differences in spinal cord MTR (C1 to T12) and pain (heat/cold stimuli) between patients and controls, and strong correlation between MTR and heat detection thresholds.
Introduction
Myelitis
is a neurological disease characterized by inflammation and subsequent
demyelination of the spinal cord. It can occur as an isolated condition or may
be the first presentation of a relapsing acquired demyelinating syndrome such
as multiple sclerosis (MS). Pain is a significant problem in myelitis and 65%
to 90% of patients with myelitis rate their pain as severe, and interfering
with rehabilitative efforts.1,2
Conventional MRI has been shown to have poor correlation with the clinical
status of patients with myelitis.2 Magnetization
Transfer Imaging (MTI) could be a sensitive method for detection of myelin loss.3,4 To our
knowledge, no standardized technique has been developed to assess pain and how
it relates to myelin loss in pediatric myelitis. The aims of this study were to
(1) determine the feasibility of performing pain sensory testing in pediatric
myelitis, and (2) examine differences in pain values between patients and
healthy controls, and (3) investigate the relationship between pain and MTI.Methods
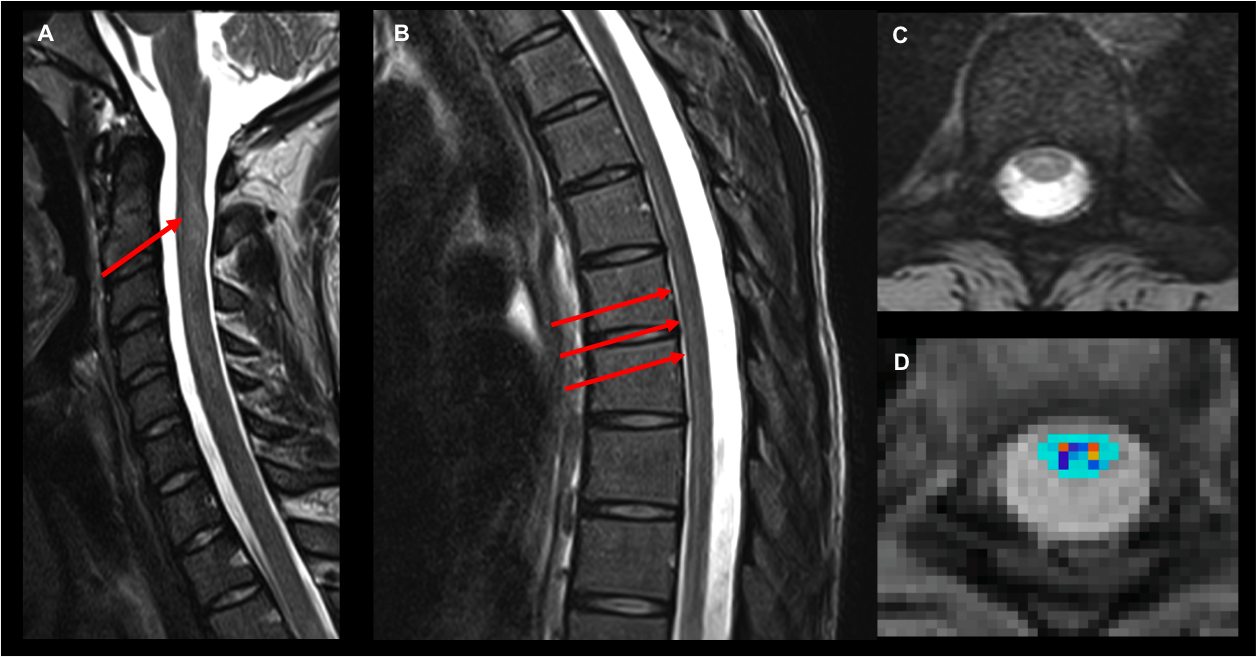
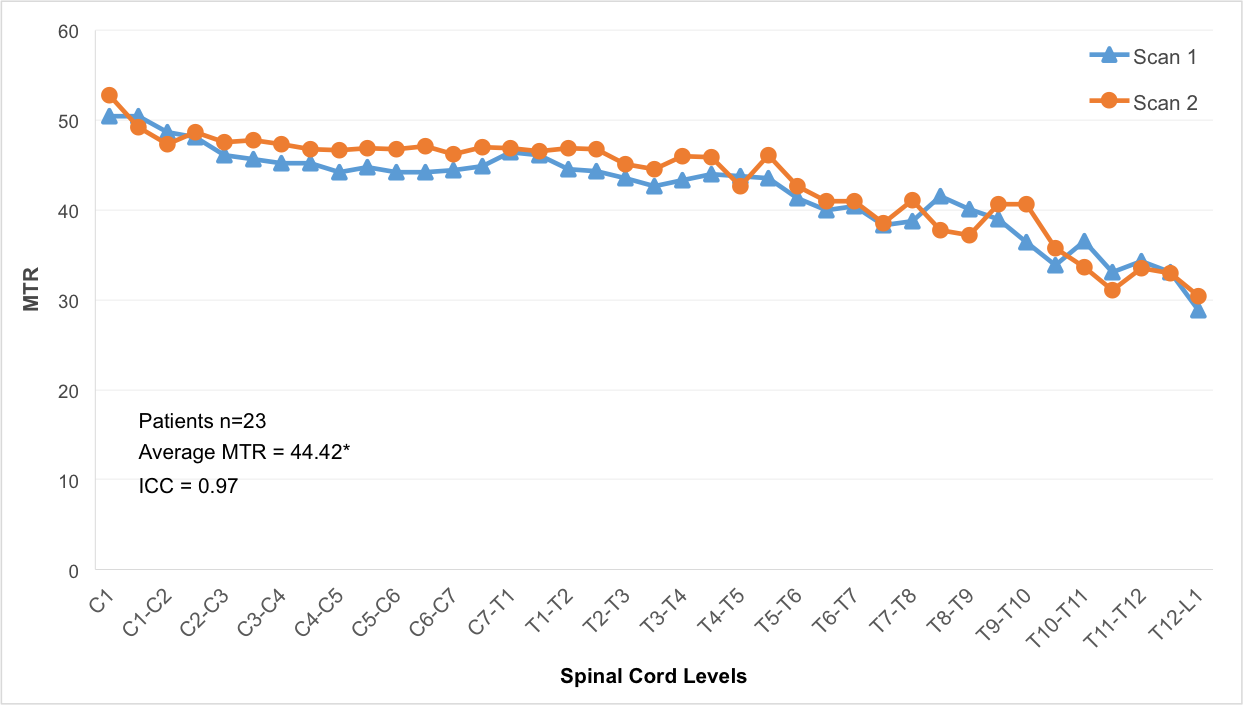
The study was approved by the Institutional Review Board and written informed consent was obtained from all participants and/or parents. Subjects: 23 patients with myelitis (mean age = 14.9 years, lesions spanning C1 to T12), and 16 age-matched healthy controls (mean age = 14.6 years). Pain assessment: Pain sensory testing was performed using the Thermal Sensory Analyzer (Medoc Ltd., Haifa, Israel). A contact thermode was placed on the level of injury (corresponding dermatome) delivering painful and non-painful stimuli at temperatures -10ºC to 54ºC. Four measures were obtained: heat and cold detection thresholds (HDT, CDT) and heat and cold pain thresholds (HPT, CPT). Imaging: Subjects were scanned using a 3T MRI system. The imaging protocol included axial T2-weighted images, and MTI (28 axial slices, TR/TE=1190/4.37ms, 1.3x0.9x5mm3, 2 averages, flip angle=20°,BW=3800Hz/Px, pulse duration=9984μs, frequency offset=1200 Hz, acquisition time=12min). Magnetization Transfer Ratio (MTR) calculations were performed using Spinal Cord Toolbox V3.0.8.5 (Figure 1) and values were reported for the entire spinal cord (C1 to T12). Statistical analysis: All statistical analyses were performed using SPSS v24 (IBM, Armonk, NY) and Stata v15.0 (StataCorp, College Station, TX). Modeling using generalized estimating equations (GEE) was performed between the patients and controls to evaluate significant differences in mean MTR, HDT, CDT, HPT and CPT values. Reproducibility between scans 1 and 2 was established using the Intraclass correlation coefficients (ICC). Pearson’s correlation coefficient was used to analyze the correlation between MTR and pain measures. A two-side alpha of 0.05 was used to determine statistical significance.Results
Our findings showed strong agreement in MTR values between scan 1 and scan 2 for patients and controls. Figure 2 shows results for the patient group. There were significant differences in MTR values, and all four pain measures (CDT, HDT, CPT and HPT) between patients and healthy controls (P<0.001) (Table). When correlated with pain measures, there was a significant correlation between MTR and HDT (r=0.26, P<0.05).Discussion
The relationship between spinal cord demyelination and pain was examined in a large cohort of pediatric patients and healthy controls. Our results showed significant differences in spinal cord MTR (C1-T12) between the two groups, and significant differences in Cold Detection Threshold (CDT), Heat Detection Threshold (HDT), Cold Pain Threshold (CPT), and Heat Pain Threshold (HPT). Additionally we confirmed a significant correlation between MTR and HDT. Pain in myelitis involves damage to nociception processing pathways (spinothalamic tract). The sequence of events leading to pain may start following a lesion involving the dorsal horn of the spinal cord, and subsequently alterations in the myelinated axons. The demyelinated axons will exhibit a reduction in electrical conduction, which may contribute to the sensation of pain.6 Thermal sensory testing examines the function of A-delta nerve fibers (responsible for cold detection threshold) and C nerve fibers (heat detection threshold).7 The measured group differences between in MTR and pain measures, and the positive correlation between myelin content and heat detection thresholds are presumed to be due to demyelination, and alterations in the A-delta and C fiber function. Further analysis will include comparisons by lesion level, and correlation between MTR, additional pain measures (e.g. pressure, pin prick), disability scores, and other imaging modalities.Acknowledgements
Research reported in this publication was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), (K25, PI: Barakat).References
1. Sadowsky CL, Becker D, Bosques G, et al. Rehabilitation in transverse myelitis. Continuum (Minneap Minn). 2011;17(4):816-830.
2. Defresne P, Hollenberg H, Husson B, et al. Acute transverse myelitis in children: Clinical course and prognostic factors. Journal of Child Neurology. 2003;18(6):401-406.
3. Pradat P, Cohen-Adad J, El Mendili M, et al. Diffusion and magnetization transfer imaging detects spinal cord lesions in amyotrophic lateral sclerosis. Proc Intl Soc Mag Reson Med. 2011;19:2465.
4. Zackowski KM, Smith SA, Reich DS, et al. Sensorimotor dysfunction in multiple sclerosis and column-specific magnetization transfer-imaging abnormalities in the spinal cord. Brain. 2009;132(Pt 5):1200-1209.
5. De Leener B, Levy S, Dupont SM, et al. SCT: Spinal cord toolbox, an open-source software for processing spinal cord MRI data. Neuroimage. 2017;145(Pt A):24-43.
6.
Serra J, Bostock H, Sola R, et al. Microneurographic identification of
spontaneous activity in C-nociceptors in neuropathic pain states in humans and
rats. Pain. 2012;153(1):42-55.
7. Krumova EK, Geber C, Westermann A, Maier C. Neuropathic pain: Is quantitative sensory testing helpful? Curr Diab Rep. 2012;12(4):393-402.
Figures