0300
Cervical Spine inhomogeneous Magnetization Transfer (ihMT) Imaging Using ECG-Triggered 3D Rapid Acquisition Gradient-Echo (ihMT-RAGE)1Siemens Healthcare SAS, Saint-Denis, France, 2Aix-Marseille Univ, CNRS, CRMBM, Marseille, France, 3APHM, Hôpital Universitaire Timone, CEMEREM, Marseille, France, 4Radiology, Division of MR research, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, United States
Synopsis
Inhomogeneous magnetization transfer (ihMT) is a promising MRI modality that provides high sensitivity and specificity to myelinated tissue. Demyelinating pathologies in the central nervous system could then be addressed by this technique. The goal of this work is to demonstrate that the combination of ihMT preparation with Rapid Acquisition Gradient Echo (ihMT-RAGE), as recently proposed for the brain, can be adapted to an ECG-triggered 3D exploration of the cervical spinal cord within a clinically-compatible scan time. The in-vivo ihMT results from healthy cervical spinal cord demonstrate the great potential of the ihMT-RAGE technique for future investigations of degenerative spinal cord pathologies.
Introduction
Inhomogeneous magnetization transfer (ihMT) is a promising MRI modality that provides high sensitivity and specificity to myelinated tissue1-3. This technique is attractive to address demyelinating pathologies in the central nervous system.
State-of-the-art 3D sequences proposed for brain imaging have consisted of either ihMT prepared Rapid Acquisition Gradient Echo (ihMT-RAGE4) or interleaved ihMT gradient echo (ihMT-GRE5) repeated to reach a steady state.
As a small moving organ surrounded by pulsatile cerebrospinal fluid (CSF), the spinal cord is a difficult region to image using MRI. The first methodological developments of ihMT in cervical spine (c-spine) consisted of ECG-triggered 2D single-shot readouts, such as Haste or EPI, and were further applied to both healthy and patient populations6-9. More recently, c-spine ihMT ratio (ihMTR) was measured at 3T using segmented 3D GRE acquisition10. Limitations of previous work consist in i. the use of 2D single-shot techniques which limits spatial coverage and induces blurring or susceptibility artefacts or ii. the use of 3D ihMT-GRE whose steady-state is not compatible with physiological triggering.
The goal of this work was to demonstrate that the ihMT-RAGE sequence can be adapted to an ECG-triggered 3D exploration of the cervical spinal cord in healthy volunteers.
Methods
A sensitivity-enhanced ihMT preparation5,11 was implemented to mitigate sensitivity to B1+ spatial variations as recently proposed in the brain at 3T12. Briefly, the ihMT RF irradiation was concentrated with 4 bursts of 16 Tukey-shaped RF pulses interleaved with a long mixing period, leading to a total ihMT preparation time of 1.06s. The ihMT preparation was directly followed by a centric-out RAGE readout to keep the ihMT signal maximum in the central part of k-space. The sequence chronogram and ihMT parameters are described in Fig1.
Experiments were performed on three healthy volunteers (age:40±4yo.) on a 3T Verio (Siemens Healthcare GmbH, Erlangen, Germany) using standard coil setup for c-spine imaging. Localized shim was performed prior to ihMT scanning at C1-C7 levels. A reference volume (M0) and ihMT volumes (MT+/MT+-/MT-+/MT-) repeated 3 times were acquired transversally with 0.9mm in-plane resolution and 10mm slice thickness. The ihMT-RAGE sequence was first repeated with and without ECG synchronization and then compared with single-slice ECG-triggered ihMT-Haste acquisition obtained at C3 level only7. Each scan lasted ~8-10min depending on the subject’s heartrate. TRihMT-RAGE was set to 2.2s for the non-triggered acquisition. An additional ihMT-RAGE was performed in one subject with factory shim settings to evaluate potential effects of B0 inhomogeneity.
All MT-prepared volumes were first co-registered to the M0 reference using rigid motion correction. ihMTR was then calculated as Mean[MT++MT--MT+--MT-+]/M0. MT ratio was also computed for comparison using 1-MT+/M0 only. ihMTR values in grey and white matter (GM/WM) were extracted from manual segmentation within the cervical levels C1-C6.
Results & Discussion
Fig2 shows ihMTRs and MTRs from triggered and non-triggered ihMT-RAGE acquisitions as well as triggered ihMT-Haste obtained in Subject#1. The spinal cord specific WM and butterfly-shape GM can easily be seen in the triggered scan while the structure disappears in some cervical levels for the non-triggered one. The triggered ihMT-Haste scan exhibits a slightly lower ihMTR in whole cord at C3 level (6.1±0.3%vs.7.3±1.6% for ihMT-RAGE), as expected by the enhanced preparation12. Additionally, because of in-plane blurring, the butterfly-shape GM is harder to distinguish and presented a similar value than WM as compared to ihMT-RAGE (GM:6.0±0.3%vs.5.2±0.6%; WM:6.1±0.3%vs.8.4±1.4%).
The importance of cardiac synchronization is further highlighted in Fig3, presenting two cervical levels with and without ECG-triggering. Repeating multiple 3D readouts without cardiac synchronization, i.e. with acquisitions performed during different phase of the CSF-pulsatility cycle, led to ihMTR contamination by small physiological motion. This behavior can also been seen in the sagittal reformat presented in Fig4. This figure also emphasizes the high importance of localized shimming in the c-spine.
Mean±SD ihMTR measured in the 3 subjects from C1-C6 was 9.2±2.5% in GM and 11.3±2.0% in WM. ihMTR values were higher than previously reported10.
On one hand, ihMT-RAGE appears more robust and reliable to provide contrasted GM/WM ihMTR on multiple cervical levels than single-slice ihMT-Haste or even multi-slice multi-angle (MSMA) 2D EPI acquisitions which suffer from blurring, susceptibility artefacts or slice-timing relaxation correction. On the other hand, partial volume effect (PVE) is expected to be more dominant using single 3D volume with thick slices as compared to MSMA 2D techniques, which could be disadvantageous when addressing patient population.
Conclusion
Further work will focus on optimizing the spatial resolution, in particular to limit PVE, while shortening scan time with advanced reconstruction techniques. Spatial coverage, resolution and ihMT signal gains achieved with ECG-triggered 3D RAGE readout gives new insights in the use of ihMT in cervical spinal cord clinical investigations.Acknowledgements
This project has received funding from the European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie grant agreement No713750. Also, it has been carried out with the financial support of the Regional Council of Provence-Alpes-Côte d’Azur and with the financial support of the A*MIDEX (n° ANR- 11-IDEX-0001-02), funded by the Investissements d'Avenir project funded by the French Government, managed by the French National Research Agency (ANR).References
- Varma G, Duhamel G, de Bazelaire C, at al. Magnetization Transfer from Inhomogeneously Broadened Lines: A Potential Marker for Myelin. Magn. Reson. Med. 2015;73:614–622. doi: 10.1002/mrm.25174.
- Girard OM, Prevost VH, Varma G, et al. Magnetization transfer from inhomogeneously broadened lines (ihMT): Experimental optimization of saturation parameters for human brain imaging at 1.5 Tesla. Magn. Reson. Med. 2015;73:2111–2121. doi: 10.1002/mrm.25330.
- Prevost VH, Girard OM, Cayre M, et al. Validation of inhomogeneous Magnetization Transfer (ihMT) as a myelin biomarker. In: Proceedings of the ISMRM. Honolulu, HI, USA; 2017, #4549.
- Varma G, Girard OM, Mchinda S, et al. 3D inhomogeneous magnetization transfer and rapid gradient echo (ihMTRAGE) imaging. . In: Proceedings of the ISMRM. Paris, France; 2018, #5503.
- Mchinda S, Varma G, Prevost VH, et al. Whole brain inhomogeneous magnetization transfer (ihMT) imaging: Sensitivity enhancement within a steady-state gradient echo sequence. Magn. Reson. Med. 2017. doi: 10.1002/mrm.26907.
- Girard OM, Callot V, Prevost V, et al. Magnetization Transfer from Inhomogeneously Broadened Lines (ihMT): Improved Imaging Strategy for Spinal Cord Applications. Magn. Reson. Med. 2017. doi: 10.1002/mrm.26134
- Taso M, Girard OM, Duhamel G, et al. Tract-specific and age-related variations of the spinal cord microstructure: a multi-parametric MRI study using diffusion tensor imaging (DTI) and inhomogeneous magnetization transfer (ihMT). NMR Biomed 2016;29(6):817-32.
- Rasoanandrianina H, Grapperon AM, Taso M, et al. Region-specific impairment of the cervical spinal cord (SC) in amyotrophic lateral sclerosis: A preliminary study using SC templates and quantitative MRI (diffusion tensor imaging/inhomogeneous magnetization transfer). NMR Biomed 2017. doi: 10.1002/nbm.3801
- Rasoanandrianina H, Duhamel G, Massire A et al. A new rapid and high-resolution multi-slice inhomogeneous Magnetization Transfer protocol to evaluate diffuse and regional cervical cord myelination at 3T. In: Proceedings of the ISMRM. Paris, France; 2018, #1855.
- Ercan E, Pinho MC, Varma G, et al. 3D Steady-State Inhomogeneous Magnetization Transfer (ihMT) Gradient Echo Sequence for Spinal Cord Imaging at 3T. In: Proceedings of the ISMRM. Paris, France; 2018, #5502.
- Varma G, Girard OM, Mchinda S, et al. Low duty-cycle pulsed irradiation reduces magnetization transfer and increases the inhomogeneous magnetization transfer effect. J. Magn. Reson. 2018. doi: 10.1016/j.jmr.2018.08.004
- Mchinda S, Varma G, Draveny R, et al. Whole brain inhomogeneous Magnetization Transfer (ihMT) imaging at 3T: concentrating RF power to mitigate RF inhomogeneities effects. In: Proceedings of the ISMRM. Paris, France; 2018, #0786.
Figures

Schematic chronogram of the ECG-triggered 3D ihMT-RAGE sequence. Only one off-resonance dual-frequency MT experiment is illustrated here.
Bursts of 16 RF-pulses, followed by a time with RF power set off, were repeated every BTR=345ms prior to a centric-out RAGE readout. The 1.06s preparation time helps to achieve ihMT steady-state while being compatible with cardiac synchronization. This sequence kernel is repeated every two heartbeat to fill k-space in the second phase encoding direction. A total of thirteen transversal 3D volumes (M0+[M+/M+-/M-/M-+]*3, yellow box) were acquired in 8-10 minutes. Localized shim was performed prior scanning at C1-C7 levels (green box).
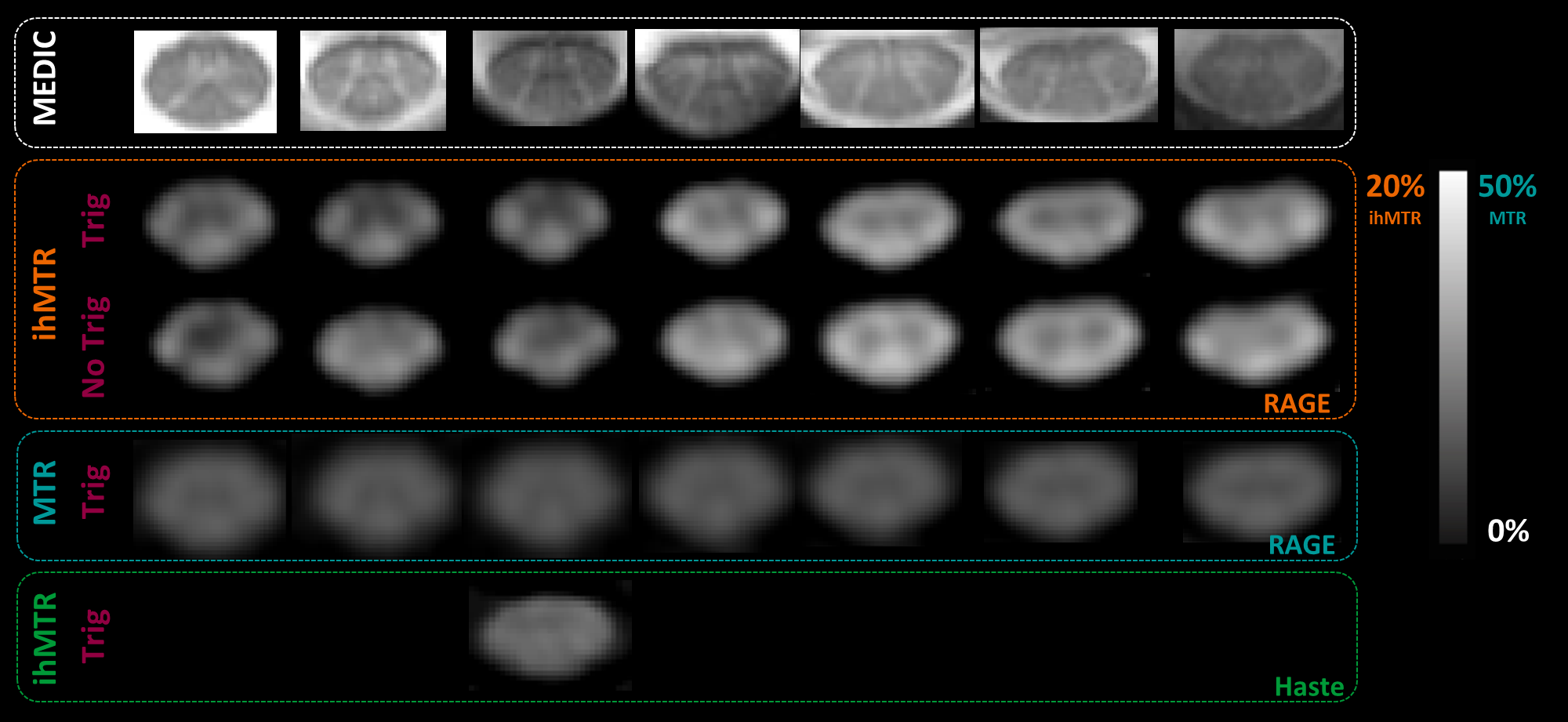
Representative images from Subject#1 showing ihMTR from C1 to C7 levels for ECG-triggered and non-triggered ihMT-RAGE acquisitions (orange).
MTR was computed from the triggered ihMT-RAGE data using single positive MT pulses (blue).
For comparison, ihMTR was also acquired using ECG-triggered and TR-sorted single-shot Haste acquisition at C3 level only (green). Acquisition time of both ihMT-RAGE and ihMT-Haste sequences was ~8min.
ECG-triggered acquisition preserved well the grey and white matter cervical structures (see for example the sharp delineation of the grey matter dorsal horns), as highlighted by comparison with the multi-echo spoiled T2*-weighted MEDIC images acquired at the same levels (white).
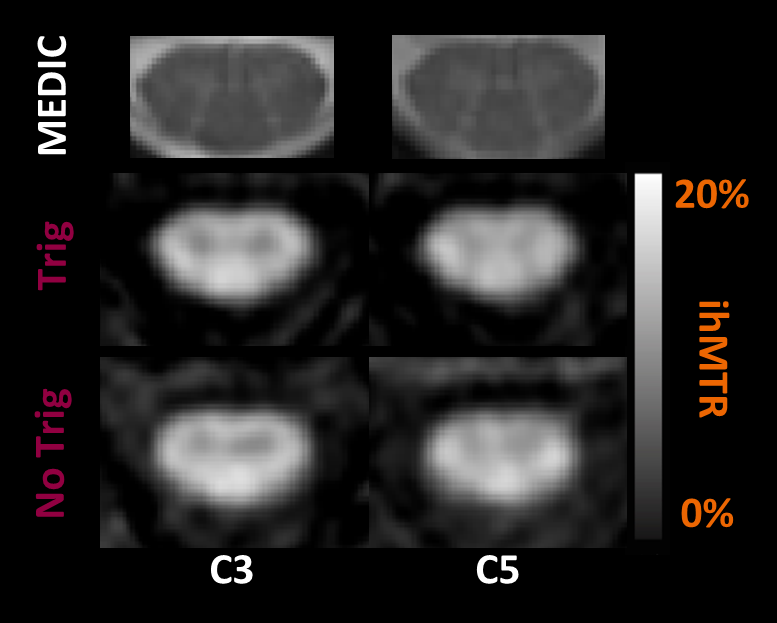
Inhomogeneous magnetization transfer ratio (ihMTR) zoomed at C3 and C5 levels for triggered (middle) and non-triggered (bottom) ihMT-RAGE acquisitions on Subject#2.
ECG-triggered acquisition preserved grey and white matter shapes (see for instance GM dorsal horns), while preventing from CSF signal contamination (slightly more blurring at the WM/CSF interface).
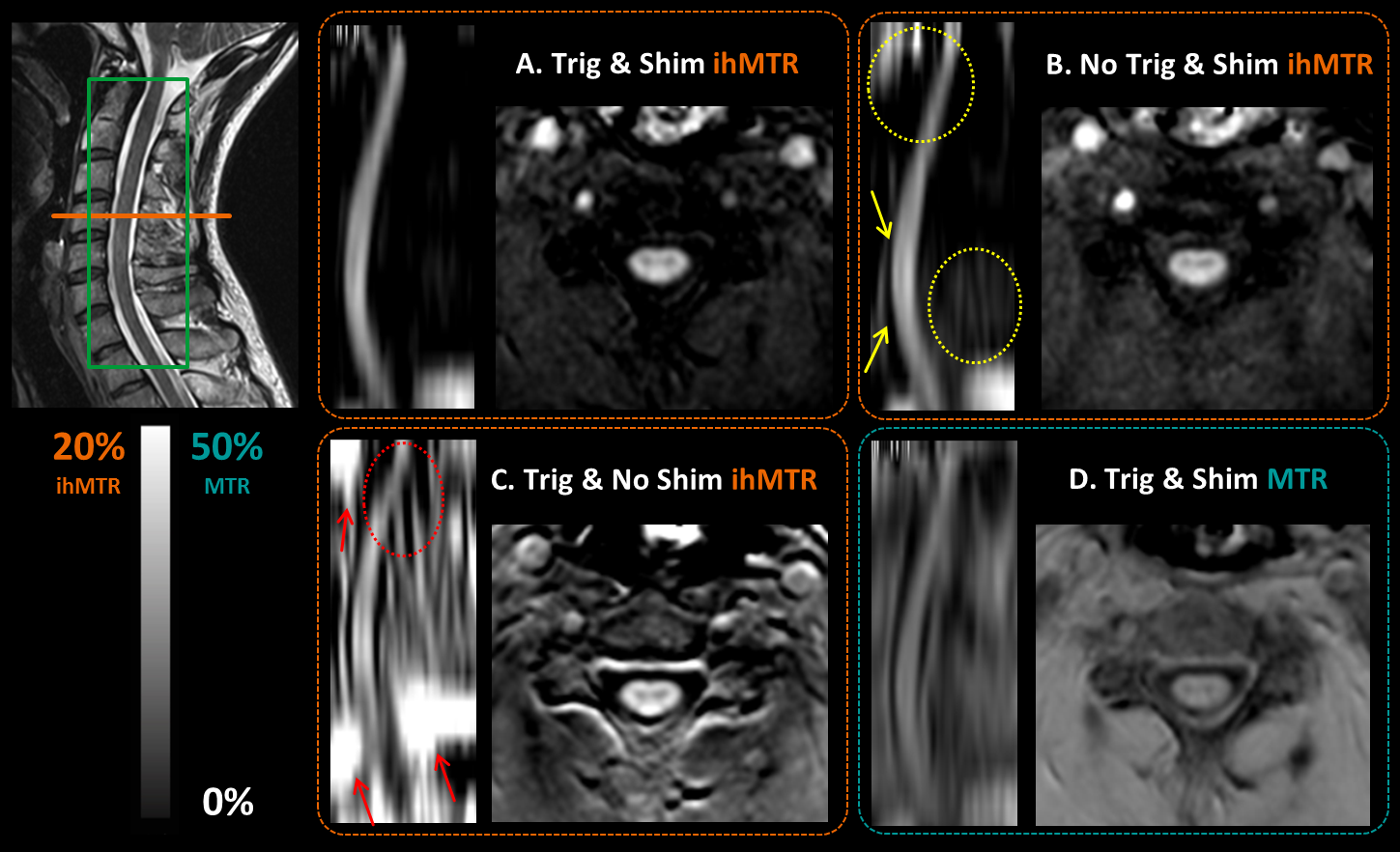
ihMTR presented in native transverse orientation and sagittal reformat in front of the anatomical T2*-weighted image. ihMTR was computed from A.ECG-triggered and localized shim, B.constant TRihMT-RAGE=2.2s and localized shim and C.ECG-triggered and factory shim.
ECG triggering helps to maintain sharp spinal cord structure (yellow arrows) and prevents unwanted ihMTR variation along the field of view (yellow circles).
The localized shim helps to prevent unpredictable ihMTR offsets in the region of interest (red arrows) or ihMT distortions caused by on-resonance effects of the MT pulses (red circle).
MTR was computed in D. with the data from A. to highlight the lack of specificity of traditional MT.