0299
Advanced Magnetic Resonance techniques in Post-Mortem Human Spinal Cord Injury: Correlations with Histopathology1International Collaboration on Repair Discoveries, Vancouver, BC, Canada, 2Radiology, University of British Columbia, Vancouver, BC, Canada, 3Physics and Astronomy, University of British Columbia, Vancouver, BC, Canada, 4UBC MRI Research Centre, Vancouver, BC, Canada, 5Pathology and Laboratory Medicine, University of British Columbia, Vancouver, BC, Canada, 6Vancouver Spine Surgery Institute, Vancouver, BC, Canada, 7Vancouver General Hospital, Vancouver, BC, Canada, 8Medicine, University of British Columbia, Vancouver, BC, Canada
Synopsis
Spinal cord injury prognosis assessments rely on subjective clinical evaluations and often poorly predict outcome; quantitative imaging biomarkers for spinal cord injury evaluation would aid clinical decision making. Our study applied two advanced MRI techniques to the imaging of post-mortem human spinal cord injury samples. We compared in-homogeneous magnetisation transfer and NODDI metric maps with six histological stains to relate the MR image contrast to biological correlates. We found a correlation trend between ihMT signal with strong T1D-filtering and Luxol Fast Blue optical density (myelin phospholipid stain) in white and grey matter.
Introduction
Current techniques for spinal cord injury (SCI) assessment rely on subjective clinical evaluations and often poorly predict outcome. Understanding the microstructural pathology of SCI and establishing biomarkers for clinical outcomes is a vital area of research1. MRI biomarkers which have been previously suggested include ‘intramedullary lesion length’ on conventional MRI and fractional anisotropy in diffusion tensor imaging2–4. Once a biomarker has been identified, histopathological validation is key to understanding the biological correlates for the image contrast. The goal of our study was to investigate two advanced MRI techniques in post-mortem human SCI and compare them qualitatively and quantitatively with six histological stains.
Inhomogeneous Magnetisation Transfer (ihMT) is a novel enhanced magnetisation transfer method which combines images prepared with single and dual-frequency saturation prepulses to produce an inhomogeneous magnetisation transfer ratio (ihMTR) map showing areas with dipolar order5,6. The ihMT saturation prepulses can be varied in order to include or filter the short dipolar relaxation time (T1D) components of the tissue7. Myelin lipids have long T1D (T1DWM ~ 6ms)8 and so filtering out short T1D components increases myelin specificity at the cost of reducing total signal intensity. ihMT was recently examined in formalin-fixed brain9, but has not yet been applied in SCI.
Neurite Orientation Dispersion and Density Imaging (NODDI) is a three-compartment diffusion model: it separates the diffusion signal into the intra-neurite space, which gives the neurite orientation dispersion (OD) and the intra-cellular volume fraction (ICVF), the extracellular space, and an isotropic Gaussian diffusion compartment related to CSF or free water (volume fraction given by IsoVF)10. This technique has recently been validated with histology in post-mortem multiple sclerosis spinal cord11.
Methods
Acquisition: Six full-length spinal cords from patients with acute SCI were donated to the International Spinal Cord Injury Biobank (see Figure 1 for subject information). Formalin-fixed 4.5cm segments of spinal cord, centred at the injury epicentre, were imaged at room temperature with a 35 mm inner-diameter quadrature volume coil at 7T (Bruker Biospec) to obtain: (1) ihMT (single-slice FLASH, 9 mm rostral and caudal to injury epicentre, TE = 3.95, frequency offset = +/- 8 kHz, obtained with two saturation schemes: no T1D-filtering (2 cosine-modulated pulses of 1 ms, TR=50ms) and strong T1D-filtering (12 frequency-alternated pulses with a repetition time of 3.3ms, TR=100ms). (2) Diffusion (multi-shell 3D diffusion weighted SE EPI, TE/TR = 41.21/250ms, six b=0 scans, 5 shells with b=500,1000,2000,3500,5000,7000s/mm2 and 6, 15, 24, 42, 60 and 80 directions respectively, distributed uniformly over the sphere determined by a Spherical Code optimization algorithm12).
MRI analysis: All MRI data were preprocessed using non-local mean denoising13. ihMTR maps were created with an in-house MatLab procedure as (Spos+Sneg–2Sdual)/2S0. Diffusion data were corrected for susceptibility and eddy current related distortion with FSL ‘top up’ and ‘eddy’ and then fit with the NODDI tissue model using the AMICO software package10.
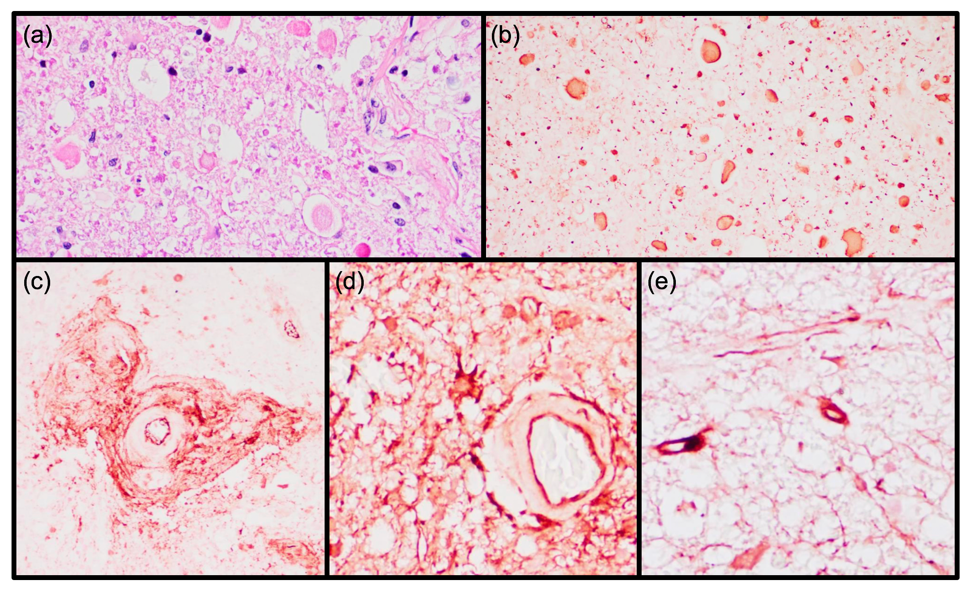
Histology: After MRI, the 4.5cm long epicentre blocks were cut into 15 segments using a 3D-printed mold for MRI-histology alignment, and paraffin-embedded. 5μM sections were stained with H&E (nuclei/cytoplasm), Luxol Fast Blue (LFB, myelin phospholipids), myelin basic protein, phosphorylated neurofilament (axons) and fibrinogen (blood-spinal cord barrier breakdown).
Correlation analysis: Optical density of LFB was determined using Image Pro Premier in twenty white and grey matter regions of interest (ROI) per sample, chosen so as not to overlap boundaries between tissue type and distributed throughout the cord cross-section. This data was compared to corresponding ROIs on strong and no T1D-filtering ihMTR metric maps using Spearman correlation analysis.
Results and Discussion
The two MRI techniques can be seen to highlight different aspects of anatomy (Figure 2). NODDI OD showed marked increases in areas of low myelin as measured by strong T1D-filtering ihMT (Figure 3a). Optical density of LFB in white matter and grey matter showed a trend-level correlation with strong T1D-filtering ihMTR (Figure 4). Figure 5 shows representative high magnification histology images displaying axonal spheroids and blood-spinal cord barrier breakdown, thought to be a key contributor to secondary pathogenesis in SCI14.Conclusion
We have demonstrated the use of two advanced MRI techniques in the analysis of post-mortem human SCI. We found clear histological evidence for blood-spinal cord barrier breakdown, which is a driver for secondary injury in SCI. We observed histological and MRI evidence for Wallerian degeneration in the lateral corticospinal tract of one subject. We found a trend level correlation between LFB, a stain for myelin phospholipids and strong T1D-filtering ihMT, but no correlation between no T1D-filtering ihMT and LFB supporting the hypothesis that T1D-filtering increases myelin specificity.Acknowledgements
We would like to thank the patients and families for tissue donation, the International Spinal Cord Injury Biobank, Blusson Integrated Cures Partnership (BICP) and the VGH and UBC Hospital Foundation. Funding was provided by an International Collaboration on Repair Discoveries (ICORD) seed grant and NSERC.References
1. Elizei, S. S. & Kwon, B. K. The translational importance of establishing biomarkers of human spinal cord injury. Neural Regen. Res. 2017; 12, 385–388.
2. Shanmuganathan, K. et al. Diffusion Tensor Imaging Parameter Obtained during Acute Blunt Cervical Spinal Cord Injury in Predicting Long-Term Outcome. J. Neurotrauma 2017; 34, 2964–2971.
3. Kurpad, S. et al. Impact of Baseline Magnetic Resonance Imaging on Neurologic, Functional, and Safety Outcomes in Patients With Acute Traumatic Spinal Cord Injury. Glob. Spine J. 2017; 7, 151S-174S.
4. Haefeli, J. et al. Multivariate Analysis of MRI Biomarkers for Predicting Neurologic Impairment in Cervical Spinal Cord Injury. AJNR Am. J. Neuroradiol. 2017; 38, 648–655.
5. Varma, G., Duhamel, G., de Bazelaire, C. & Alsop, D. C. Magnetization Transfer from Inhomogeneously Broadened Lines: A Potential Marker for Myelin. Magn. Reson. Med. 2015; 73, 614–622.
6. Girard, O. M. et al. Magnetization transfer from inhomogeneously broadened lines (ihMT): Experimental optimization of saturation parameters for human brain imaging at 1.5 Tesla. Magn. Reson. Med. 2015; 73, 2111–2121.
7. Prevost, V. H. et al. Optimization of inhomogeneous magnetization transfer (ihMT) MRI contrast for preclinical studies using dipolar relaxation time (T1D) filtering. NMR Biomed. 2017; 30, e3706.
8. Varma, G. et al. In vivo measurement of a new source of contrast, the dipolar relaxation time, T1D , using a modified inhomogeneous magnetization transfer (ihMT) sequence. Magn. Reson. Med. 2017; 78, 1362–1372.
9. Lam, M. et al. Comparison of Inhomogeneous Magnetization Transfer and Myelin Water Fraction Ex-Vivo at 7T. in ISMRM Congr. (2018).
10. Zhang, H., Schneider, T., Wheeler-Kingshott, C. A. & Alexander, D. C. NODDI: practical in vivo neurite orientation dispersion and density imaging of the human brain. NeuroImage 2012; 61, 1000–1016.
11. Grussu, F. et al. Neurite dispersion: a new marker of multiple sclerosis spinal cord pathology? Ann. Clin. Transl. Neurol. 2017; 4, 663–679 .
12. Cheng, J., Shen, D., Yap, P.-T. & Basser, P. J. Single- and Multiple-Shell Uniform Sampling Schemes for Diffusion MRI Using Spherical Codes. IEEE Trans. Med. Imaging 2018; 37, 185–199.
13. Coupe, P. et al. An optimized blockwise nonlocal means denoising filter for 3-D magnetic resonance images. IEEE Trans. Med. Imaging 2008; 27, 425–441.
14. Mautes, A. E., Weinzierl, M. R., Donovan, F. & Noble, L. J. Vascular Events After Spinal Cord Injury: Contribution to Secondary Pathogenesis. Phys. Ther. 2000; 80, 673–687.
Figures
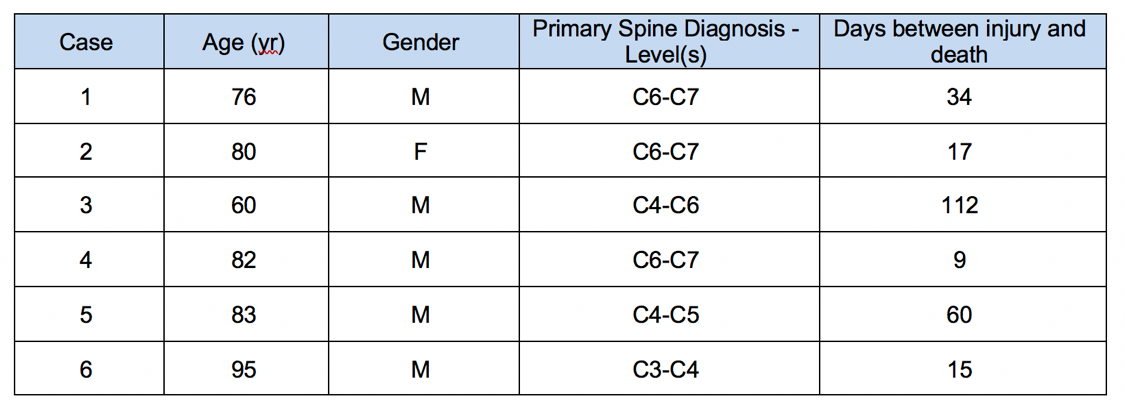
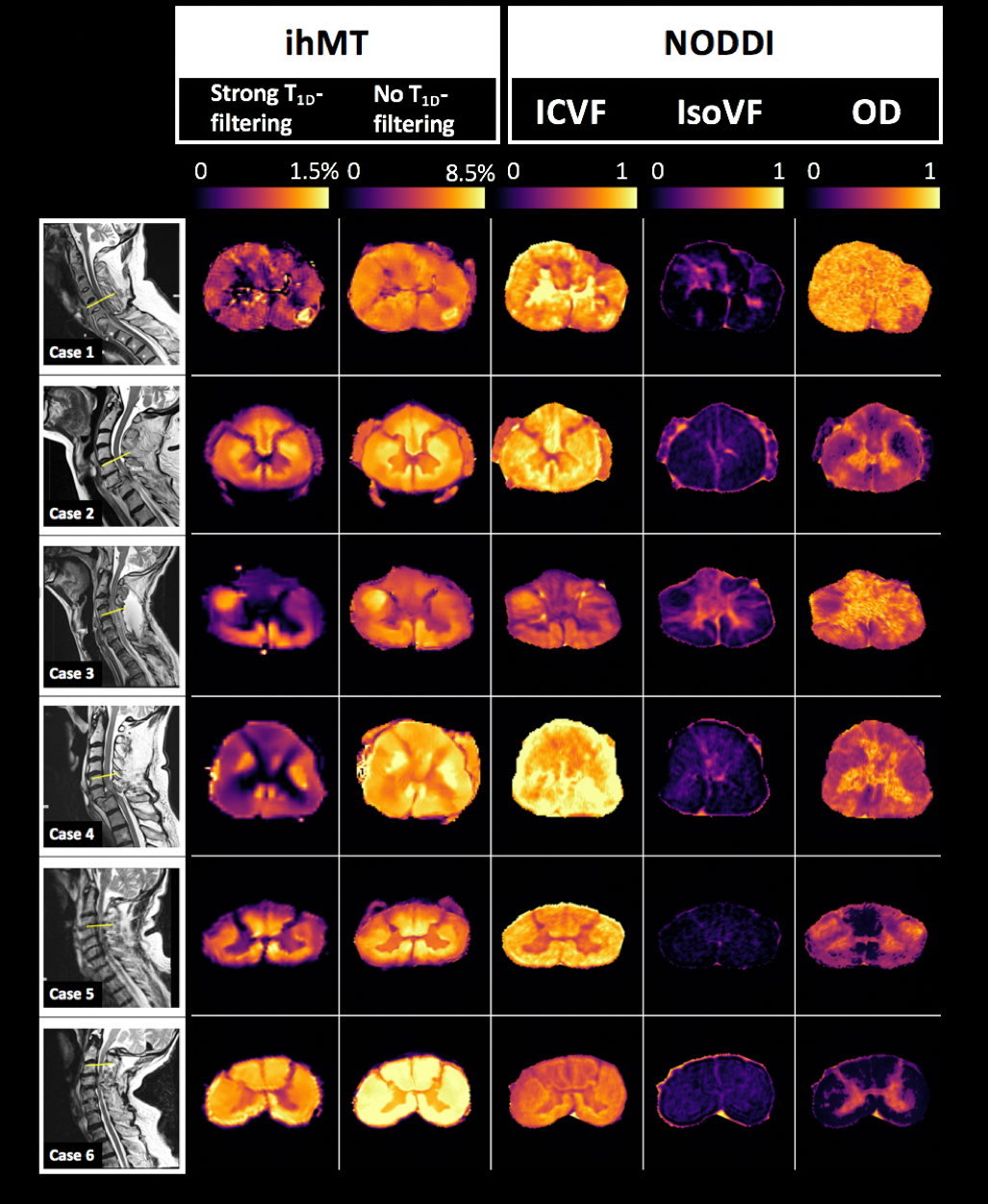
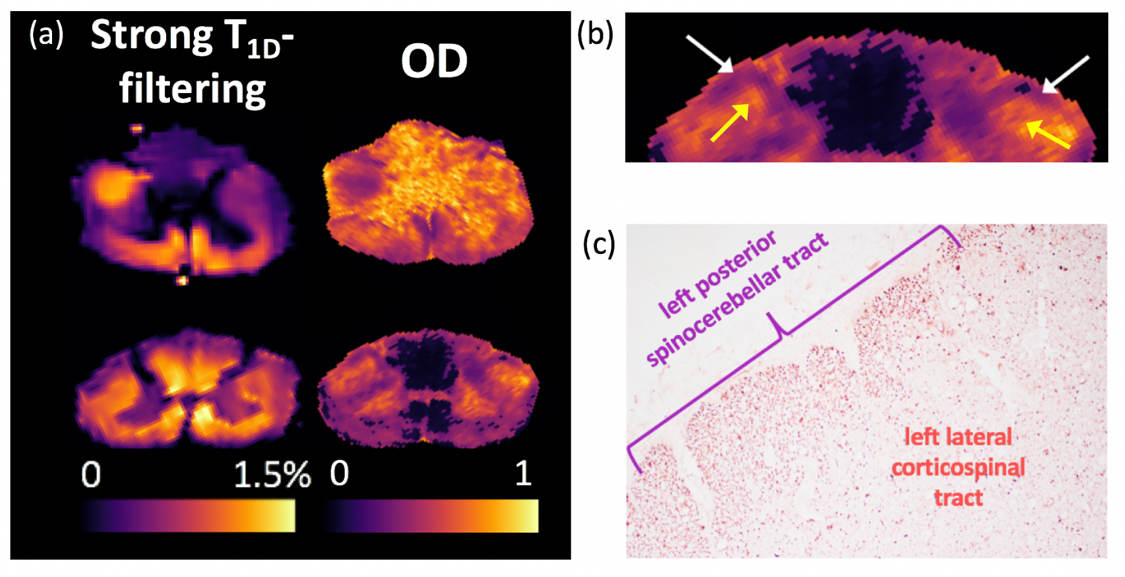
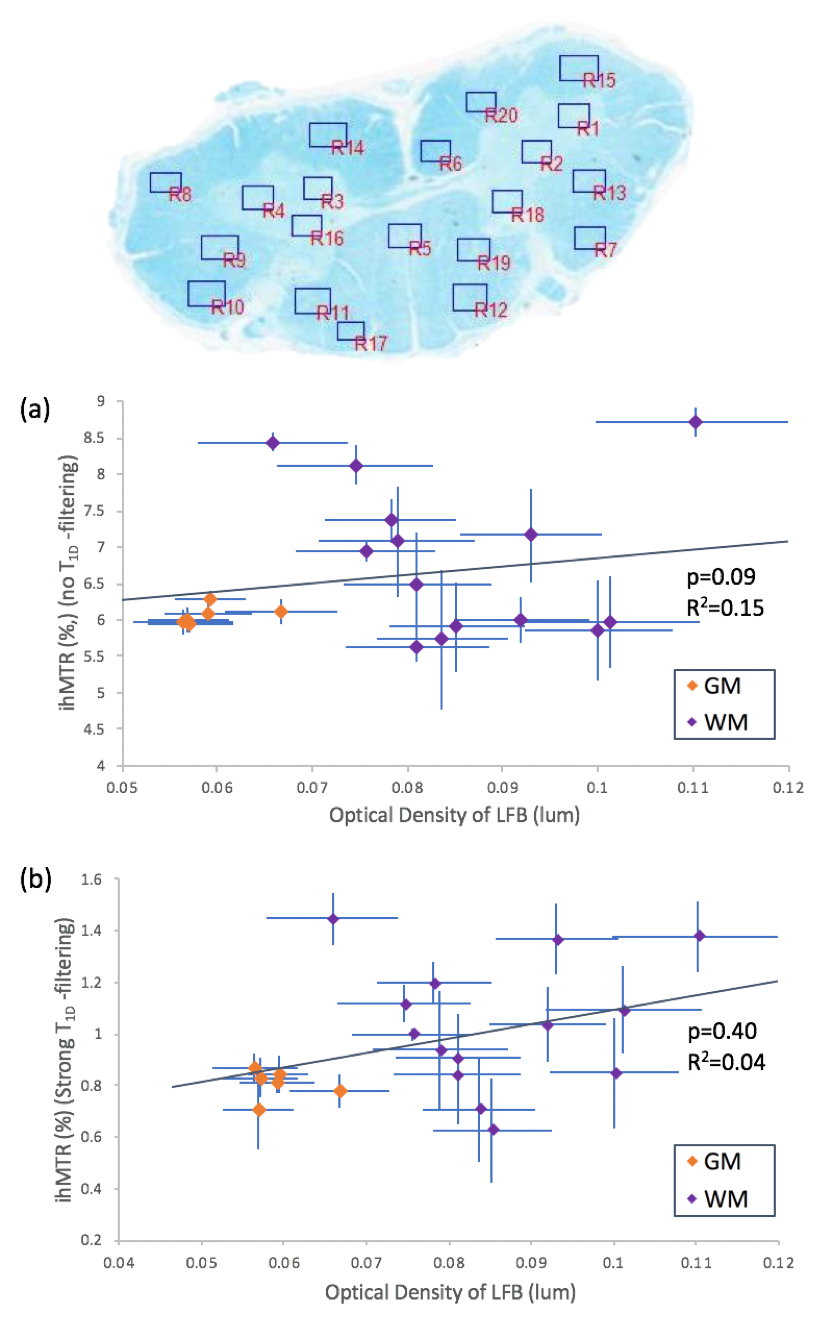
Figure 4: Regions of interest chosen in white matter (WM) and grey matter (GM). (a) No T1D-filtering ihMTR showed no correlation with LFB optical density (R2=0.04, p=0.40), (b) strong T1D-filtering ihMTR displayed a trend level correlation with LFB optical density (R2=0.15, p=0.09).