0293
White matter microstructural alterations in chronic, episodic, and aura migraine1Radiology, Center for Biomedical Imaging, New York University School of Medicine, New York, NY, United States, 2Neurology, Beth Israel Deaconess Medical Center, Brookline, MA, United States, 3Neurology, New York University School of Medicine, New York, NY, United States
Synopsis
Migraine is associated with increased risk for stroke and white matter abnormalities, though the exact nervous tissue pathology remains poorly understood. This study used diffusion kurtosis imaging, a clinically feasible extension of diffusion tensor imaging, to compare white matter microstructural changes in migraineurs to healthy controls, and between their different subtypes: chronic, episodic, with and without aura. Using a voxel-wise statistical approach, we found that axial and radial kurtosis were significantly altered depending on migraine subtype. While radial kurtosis is significantly reduced in all migraine patients compared to controls, axial kurtosis is increased in episodic migraines with and without aura, suggesting different underlying pathology.
Introduction
Migraine is a common primary headache disorder affecting approximately 12% of population with associated disability and burden1,2. Migraine can be classified as migraine with and without aura based on presence or absence of transient focal neurological symptoms. Aura is experienced by up to 30% of individuals with migraine3. In addition, migraine can be classified based on attack frequency into episodic migraine (EM) or chronic migraine (CM)4. Migraine is considered as a neurovascular headache with complex poorly understood pathophysiology with genetic component5-7. Epidemiological data suggest that migraine with aura in particular, can be associated with increased risk for stroke and white matter (WM) abnormalities8-12.
Diffusional kurtosis imaging (DKI)13 provides mesoscopic detail by quantifying and localizing barriers to diffusion in tissue, providing insight into cellular pathology such into inflammation, gliosis, or demyelination. In this study, we used DKI to characterize the microstructural pathology associated with four different types of migraine compared to healthy controls.
Materials and Methods
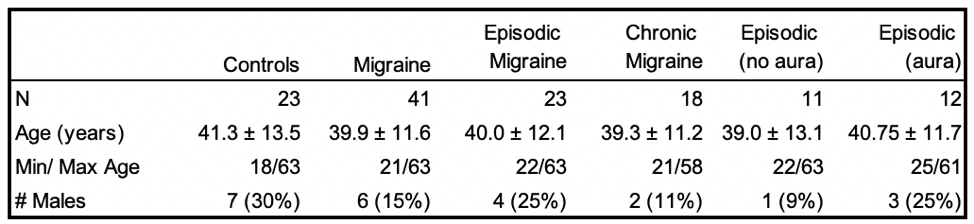
This retrospective analysis was approved by institutional review board and included 23 healthy control patients and 41 migraine patients. The group demographics are described in table 1. All patients underwent diffusion MRI on a Siemens Skyra MRI scanner (Siemens, Erlangen, Germany) with (1.69 x 1.69mm resolution, 3.0mm slice-thickness, b = 0, 250, 1000, & 2000 s/mm2, TR/TE = 3500/95ms). Diffusion data was processed using DESIGNER14 to generate parameter maps of mean, radial and axial diffusivity (MD, RD & AD), fractional anisotropy (FA), mean, radial and axial kurtosis (MK, RK & AK). Group statistical analysis of DKI parameters was carried out using FSL-TBSS (tract-based spatial statistics)15. The primary endpoint analysis was to test for overall differences between the migraine and control groups. Secondary analysis consisted of a comparison between controls, chronic and episodic migraineurs. All chronic migraine patients did not demonstrate signs of aura, therefore tertiary analysis was performed between chronic migraine (no aura), episodic migraine without aura, and episodic migraine patients with aura. For each analysis the general linear model was used to perform a two-sided t-test to measure the differences in parameters between groups using age and gender as nuisance effects. A correction for multiple comparisons was performed using threshold-free-cluser-enhancement16.Results
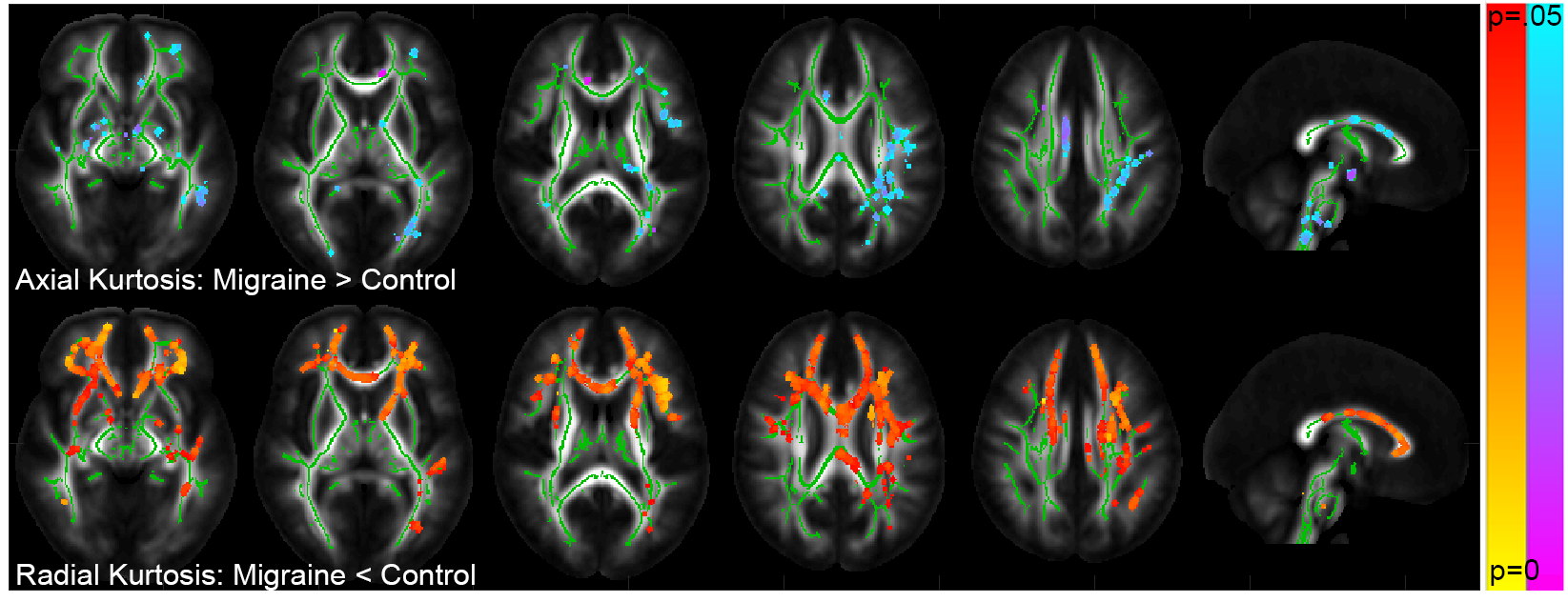
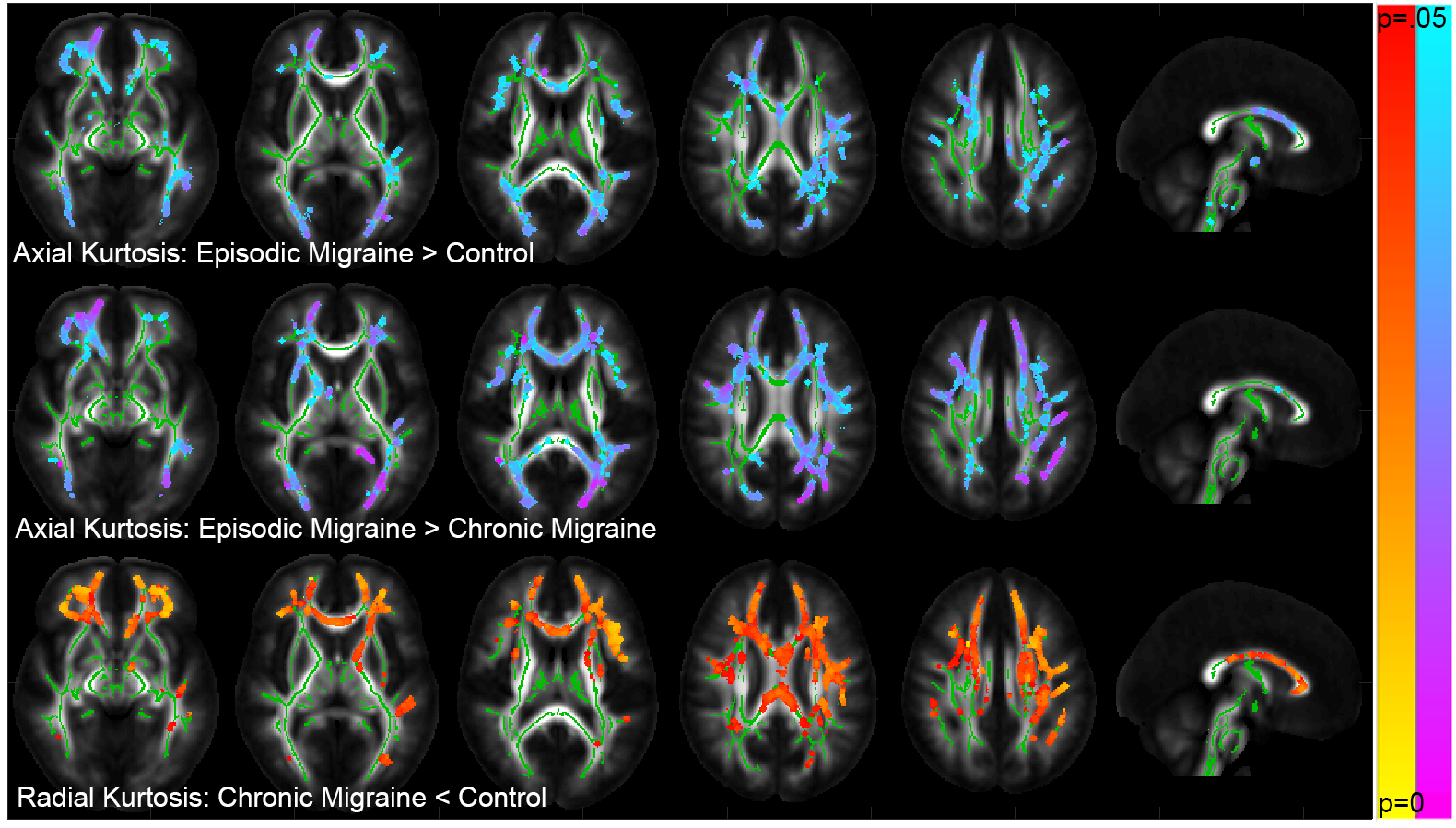
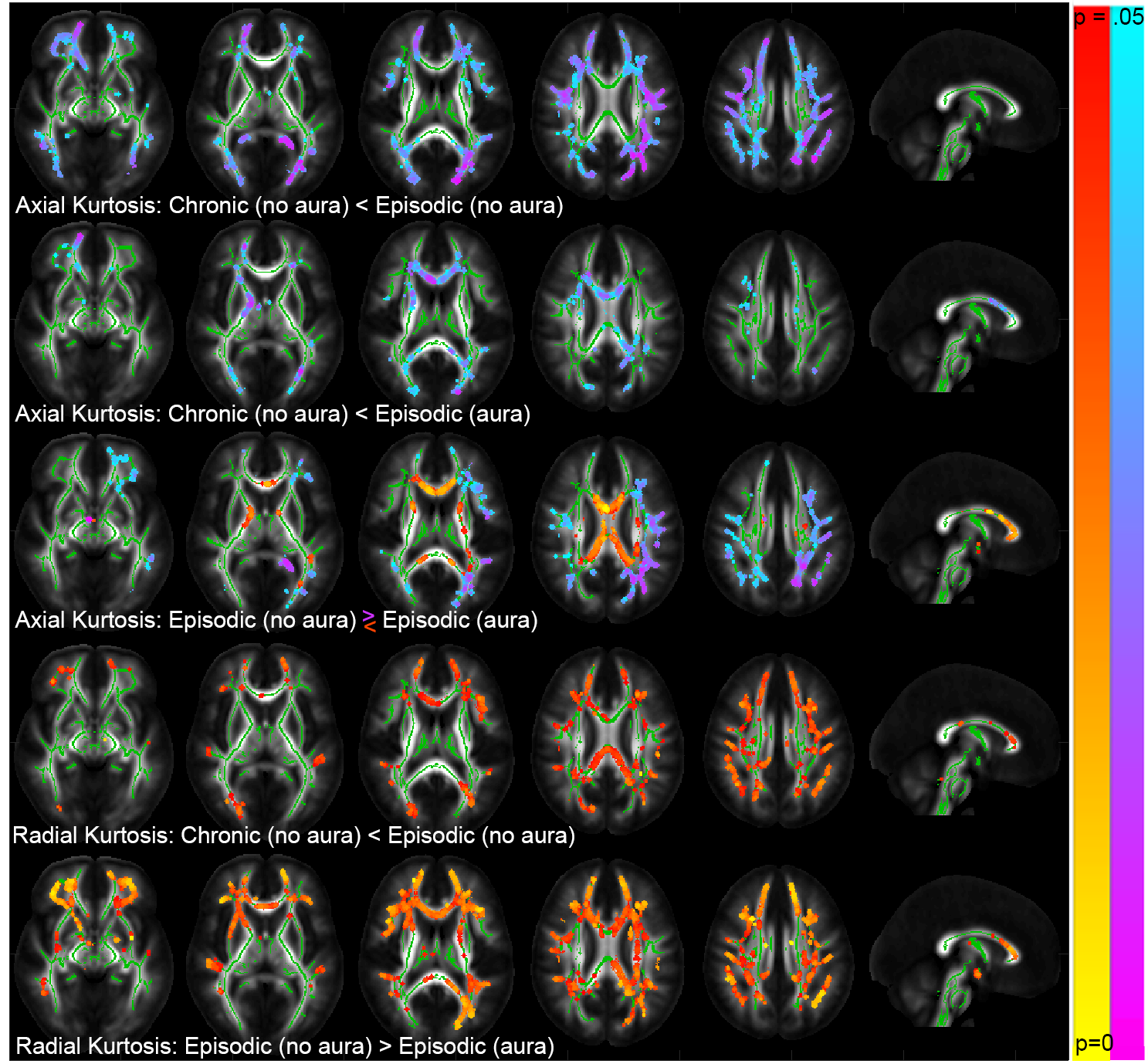
Primary analysis showed a significant (p < 0.05) increase in axial and decrease in radial kurtosis in migraineurs as compared to controls in respectively 2.8% and 14.9% voxels of the white matter skeleton. Figure 1 shows that RK is decreased in migraineurs as compared to controls primarily in frontal white matter regions including the genu of the corpus callosum, anterior limb internal capsule and frontal corona radiata, while AK is increased in the parietal corona radiata and superior longitudinal fasciculus. Interestingly, the secondary analyses shown in Figure 2 revealed that increased AK is only present in episodic migraineurs (compared to both controls and chronic migraineurs) in frontal and occipital white matter, while the decreased RK is predominantly present in chronic migraineurs. Figure 3 shows the results of the final group subset comparing chronic (no aura) with episodic (aura) and episodic (no aura). AK is increased in episodic patients with and without aura compared to chronic migraineurs, while RK is decreased in episodic patients with aura and in chronic patients as compared to episodic migraineurs without aura.Discussion
This study reports white matter alterations in the RK and AK the genu corpus callosum, corona radiata and internal capsule, regions previously shown to be affected in migraine, albeit with DTI17. Furthermore, we reported heterogeneity in white matter changes within the migraineurs depending on frequency and presence of aura, which can partially explain the lack of significant findings in DTI parameters. Remarkably, the observed changes differ depending on whether they are in the radial or axial direction. The observed increase in AK in episodic migraineurs is the same directional change (increase), though to a smaller extent, as seen in acute stroke infarcts18 compared to normal appearing white matter, and potentially could be explained here by changes in the intra-axonal environment. In addition, the specific location of increased AK in episodic patients may depend on the presence of aura. The decrease in RK present in chronic migraineurs and those with aura, on the other hand, may suggest myelin loss.Conclusion
We found clear differences in diffusion kurtosis (and not DTI) between migraine patients and controls, as well in between the migraine patients stratified by their clinical syndrome and features. A future longitudinal study of how migraine symptoms progress in relation to diffusion parameters may yield further insight into the pathology represented by the changes observed in this study.Acknowledgements
Research was supported by The National Institute of Neurological Disorders and Stroke of the NIH under award number R01 NS088040, and was performed at the Center of Advanced Imaging Innovation and Research (CAI2R, www.cai2r.net), and NIBIB Biomedical Technology Resource Center P41 EB017183.References
1. Lipton RB, Stewart WF, Diamond S, Diamond ML, Reed M. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache 2001 Jul;41(7):646-57.
2. Stovner LJ, Hagen K, Jensen R, Katsarava Z, Lipton R, Scher A, et al. The global burden of headache: a documentation of headache prevalence and disability worldwide. Cephalalgia 2007 Mar;27(3):193-210.
3. Le H, Tfelt-Hansen P, Skytthe A, Kyvik KO, Olesen J. Increase in self-reported migraine prevalence in the Danish adult population: a prospective longitudinal population-based study. BMJ Open 2012;2(4).
4. The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 2013 Jul;33(9):629-808.
5. Olesen J, Burstein R, Ashina M, Tfelt-Hansen P. Origin of pain in migraine: evidence for peripheral sensitisation. Lancet Neurol 2009 Jul;8(7):679-90.
6. Charles A. Advances in the basic and clinical science of migraine. Ann Neurol 2009 May;65(5):491-8.
7. Freilinger T, Anttila V, de VB, Malik R, Kallela M, Terwindt GM, et al. Genome-wide association analysis identifies susceptibility loci for migraine without Aura. Nat Genet 2012 Jul;44(7):777-82.
8. Bashir A, Lipton RB, Ashina S, Ashina M. Migraine and structural changes in the brain: a systematic review and meta-analysis. Neurology 2013 Oct 1;81(14):1260-8.
9. Kurth T, Slomke MA, Kase CS, Cook NR, Lee IM, Gaziano JM, et al. Migraine, headache, and the risk of stroke in women: a prospective study. Neurology 2005 Mar 22;64(6):1020-6.
10. Peng KP, Chen YT, Fuh JL, Tang CH, Wang SJ. Migraine and incidence of ischemic stroke: A nationwide population-based study. Cephalalgia 2017 Apr;37(4):327-35.
11. Schurks M, Rist PM, Bigal ME, Buring JE, Lipton RB, Kurth T. Migraine and cardiovascular disease: systematic review and meta-analysis. BMJ 2009 Oct 27;339:b3914.
12. Spector JT, Kahn SR, Jones MR, Jayakumar M, Dalal D, Nazarian S. Migraine headache and ischemic stroke risk: an updated meta-analysis. Am J Med 2010 Jul;123(7):612-24.
13. Jensen JH, Helpern JA, Ramani A, Lu H, Kaczynski K. Diffusional kurtosis imaging: the quantification of non-gaussian water diffusion by means of magnetic resonance imaging. Magn Reson Med 2005 Jun;53(6):1432-40.
14. Ades-Aron, B., Veraart, J., Kochunov, P., McGuire, S., Sherman, P., Kellner, E., ... & Fieremans, E. (2018). Evaluation of the accuracy and precision of the diffusion parameter EStImation with Gibbs and NoisE removal pipeline. NeuroImage, 183, 532-543.
15. Smith, S. M., Jenkinson, M., Johansen-Berg, H., Rueckert, D., Nichols, T. E., Mackay, C. E., ... & Behrens, T. E. (2006). Tract-based spatial statistics: voxelwise analysis of multi-subject diffusion data. Neuroimage, 31(4), 1487-1505.
16. Smith, S. M., & Nichols, T. E. (2009). Threshold-free cluster enhancement: addressing problems of smoothing, threshold dependence and localisation in cluster inference. Neuroimage, 44(1), 83-98.
17. Chong CD, Schwedt TJ. Migraine affects white-matter tract integrity: A diffusion-tensor imaging study. Cephalalgia 2015 Nov;35(13):1162-71.
18. Spampinato, M. V., Chan, C., Jensen, J. H., Helpern, J. A., Bonilha, L., Kautz, S. A., ... & Feng, W. (2017). Diffusional kurtosis imaging and motor outcome in acute ischemic stroke. American Journal of Neuroradiology.
Figures