0287
Arterial Spin Labeling Underestimates CBF in Regions with Fast Arrival Times: a Simultaneous [15O] PET/MRI Study with Acetazolamide Challenge1Radiology, Stanford University, Stanford, CA, United States, 2Neurosurgery, Tokyo Medial and Dental University, Tokyo, Japan, 3Center for Stroke Research Berlin (CSB), Charité - Universitätsmedizin Berlin, Berlin, Germany, 4Bioengineering, University of California Riverside, Riverside, CA, United States, 5Global Applied Science Lab, GE Healthcare, Menlo Park, CA, United States, 6Neurosurgery, Stanford University, Stanford, CA, United States
Synopsis
In this study, we investigated the effects of arterial transit time (ATT) reduction and the quantitative accuracy of standard and multi-delay arterial spin labeling (ASL) MRI on healthy controls and Moyamoya patients using acetazolamide (ACZ) by the voxel-wise parametric testing.
Administration of ACZ shortened ATT and extended the region where cerebral blood flow (CBF) was underestimated by standard ASL and by multi-delay ASL compared to simultaneous [15O]-water PET reference. Consideration of short ATT is critical for accurate ASL measurements of CBF in the deep gray matter and for quantification of cerebrovascular reactivity after a vasodilation challenge that decreases ATT.
Introduction
Arterial spin labeling (ASL) MRI is a promising cerebral blood flow (CBF) measurement method that does not require contrast agents. The accuracy of CBF quantification with ASL depends on image acquisition at an appropriate timing after radiofrequency pulse labeling of arterial blood. Particularly in cases involving cerebral vascular stenosis, the arterial transit time (ATT) becomes regionally prolonged, making it difficult to measure accurate CBF with a single post-labeling delay (PLD). While multi-delay ASL has been reported to improve perfusion assessment in long ATT settings,1 the quantitative capability of ASL in brain regions with short ATT is still unclear.
Acetazolamide (ACZ) is a pharmacological vasodilator that increases CBF and is used for measurement of cerebrovascular reactivity (CVR), an important index of cerebral ischemia. Vasodilation also leads to an increase in blood flow velocity, such that ATT decreases after ACZ administration. In this study, we investigated the effects of ATT reduction after ACZ on the quantitative accuracy of standard and multi-delay ASL acquisitions. We compared ASL to concurrent [15O]-PET reference scans with simultaneous PET/MRI in healthy controls and Moyamoya patients as a model of cerebrovascular stenosis.
Methods
Data were acquired from 11 healthy controls (HC) and 17 Moyamoya patients (MM) on a hybrid PET/MRI system (Signa, GE Healthcare, Waukesha, WI). Each subject was scanned twice: once at baseline and once after administration of ACZ (15mg/kg). Subjects received intravenous injections of [15O]-water (863 ± 112 MBq). Two ASL sequences and cardiac-gated phase-contrast (PC) MRI scans were performed simultaneously with each [15O]-PET scan. Standard ASL (PLD: 2025ms) and Hadamard encoded multi-delay (3 PLDs, spaced evenly between 300 – 3700ms). ASL scans were acquired with vascular crushing and pseudo-continuous labeling. The multi-delay ASL enabled measurement of and correction for arterial transit time (ATT). For a reference standard, we scaled static PET maps using whole-brain global CBF values from PC-MRI. This method, called PC-PET, was previously shown to provide reliable absolute CBF maps without invasive arterial blood sampling, including in cerebrovascular disease.2
ASL CBF for each subject group was compared with the PC-PET reference by voxel-wise parametric testing at baseline and post-ACZ, using SPM12. Mean ATT and ATT distributions were evaluated in brain regions identified with CBF over- or under-estimation by ASL compared to PC-PET.
Results
CBF and ATT maps in a representative Moyamoya patient are shown in Figure 1. Statistical parametric mapping in HC and MM showed that both standard and multi-delay ASL underestimated baseline CBF in the deep gray matter, where ATT is shorter than 800ms (Figure 2, 3). This underestimation was not observed in the caudate nucleus of MM patients, as ATT was not short in this area. Both ASL scans also overestimated baseline CBF in the splenium of the corpus callosum.
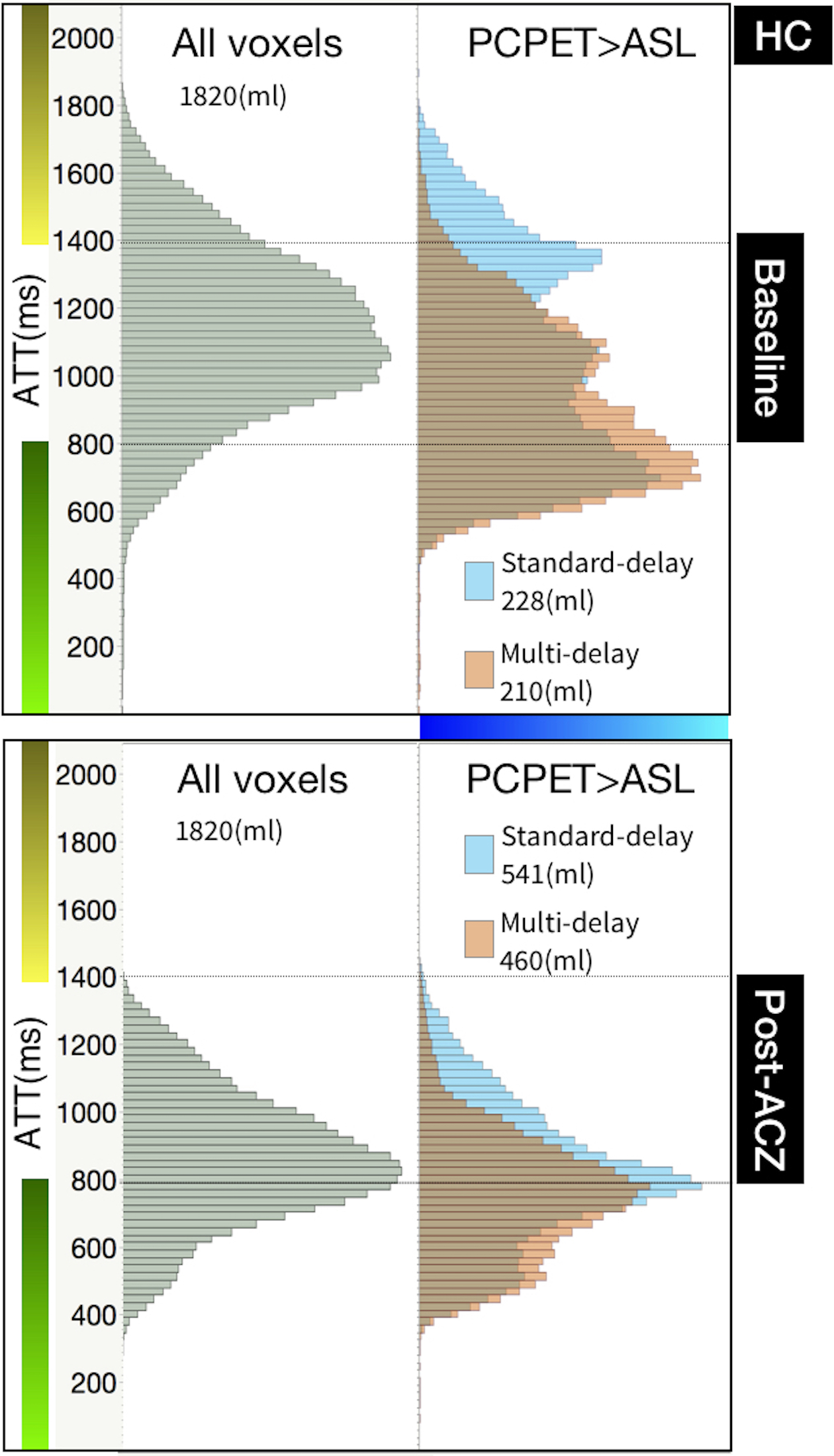
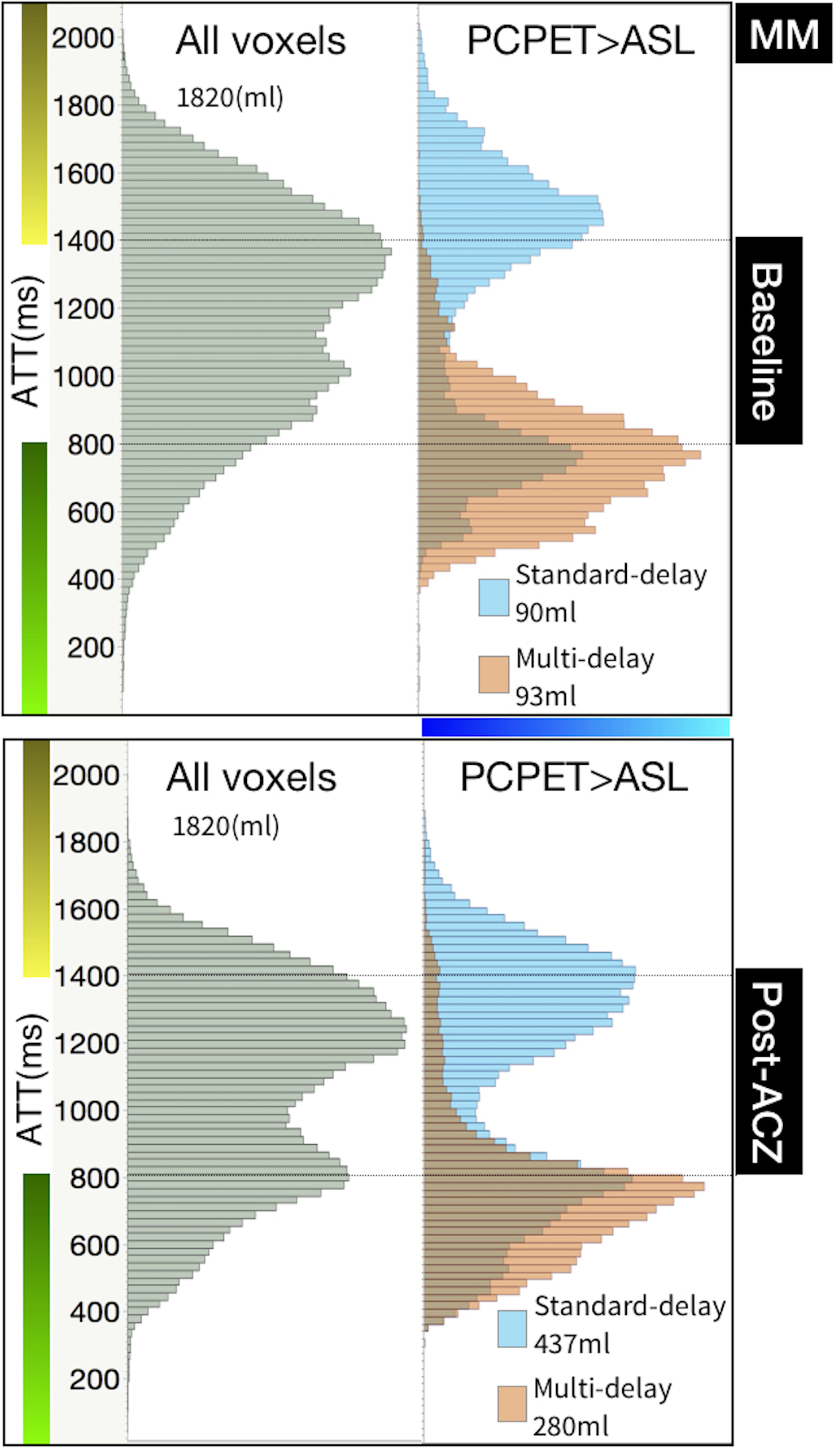
After ACZ administration, the regions where ASL underestimated CBF compared with PC-PET were larger than at baseline and showed good spatial agreement with regions that showed short ATT due to ACZ challenge. From histogram analysis, voxels where ASL underestimated CBF in HCs were distributed with short ATTs, with peak around 800ms in both standard and multi-delay ASL (Figure 4). In Moyamoya patients, standard ASL underestimated CBF in voxels with pathologically long ATT, with peak around 1450ms. While multi-delay acquisition mitigated long ATT effects, both ASL sequences showed CBF underestimation in voxels with short ATT (Figure 5).
Discussion
In the present study, standard delay ASL underestimated CBF in areas of elongated ATT, particularly in Moyamoya patients, while no significant difference was observed between multi-delay ASL and the PC-PET reference. However, even in multi-delay ASL, CBF underestimation was observed in the regions with intrinsically short ATT like deep gray-matter and after administration of ACZ, which was shown to lower ATT.
In ASL, labeled spins in the blood arriving at the capillary space exchange with spins in the brain tissue. In regions with short ATT, the label spends more time in the tissue compartment. Therefore, in regions with short ATT, it is expected that tissue T1 contributes more significantly to the longitudinal relaxation of the labeled spins in ASL3,4, and thus the quantitative accuracy of ASL CBF. In putamen and thalamus, tissue T1 has been reported to be 100-500 ms shorter than frontal gray-matter, which likely is the cause of the significant CBF underestimation by ASL in regions with low ATT.5,6
Conclusion
Administration of ACZ globally reduces ATT and extends the regions where CBF is underestimated by standard and multi-delay ASL compared to simultaneous [15O]-water PET reference. Consideration of short ATT is critical for accurate ASL measurements of CBF in deep gray matter and for quantification of cerebrovascular reactivity after a vasodilation challenge that decreases ATT.Acknowledgements
No acknowledgement found.References
1. Wang DJJ, Alger JR, Qiao JX, Gunther M, Pope WB, Saver JL et al. Multi-delay multi-parametric arterial spin-labeled perfusion MRI in acute ischemic stroke - Comparison with dynamic susceptibility contrast enhanced perfusion imaging. Neuroimage: Clinical 2013; 3: 1–7.
2. Ishii Y, Thamm T, Guo J, Khalighi MM, Wardak M, Holley D et al. Validation of Cerebrovascular Reactivity by Arterial Spin Labeling MRI in Moyamoya Disease with Simultaneously Measured 15O-PET and Phase-contrast MRI. Joint Annual Meeting ISMRM-ESMRMB 2018. https://www.ismrm.org/18/program_files/PP03.htm (accessed 6 Nov2018).
3. Wang J, Fernández-Seara MA, Wang S, Lawrence KSS. When Perfusion Meets Diffusion: in vivo Measurement of Water Permeability in Human Brain. J Cereb Blood Flow Metab 2007; 27: 839–849.
4. Debacker CS, Daoust A, Köhler S, Voiron J, Warnking JM, Barbier EL. Impact of tissue T1 on perfusion measurement with arterial spin labeling. Magn Reson Med 2017; 77: 1656–1664.
5. Gelman N, Ewing JR, Gorell JM, Spickler EM, Solomon EG. Interregional variation of longitudinal relaxation rates in human brain at 3.0 T: Relation to estimated iron and water contents. Magn Reson Med 2001; 45: 71–79.
6. Lu H, Nagae‐Poetscher LM, Golay X, Lin D, Pomper M, Zijl PCM van. Routine clinical brain MRI sequences for use at 3.0 Tesla. J Magn Reson Imaging 2005; 22: 13–22.
Figures

Representative CBF maps from [15O] PET-water PET scaled quantitatively by phase-contrast total blood flow (PC-PET), standard-delay and multi-delay ASL, and arterial transit time (ATT) maps from multi-delay ASL, at baseline and after acetazolamide (post-ACZ) scans are depicted.
In regions with very long ATT due to vessel stenosis (yellow arrows), standard ASL underestimated both baseline and post-ACZ CBF, whereas multi-delay ASL showed visually similar CBF maps compared to PC-PET. In the left insular cortex (pink arrowheads), ATT values were moderate in baseline scan and became extremely short in the post-ACZ scan. Correspondingly, both ASL methods underestimated left insula CBF compared to PC-PET in the post-ACZ scan.
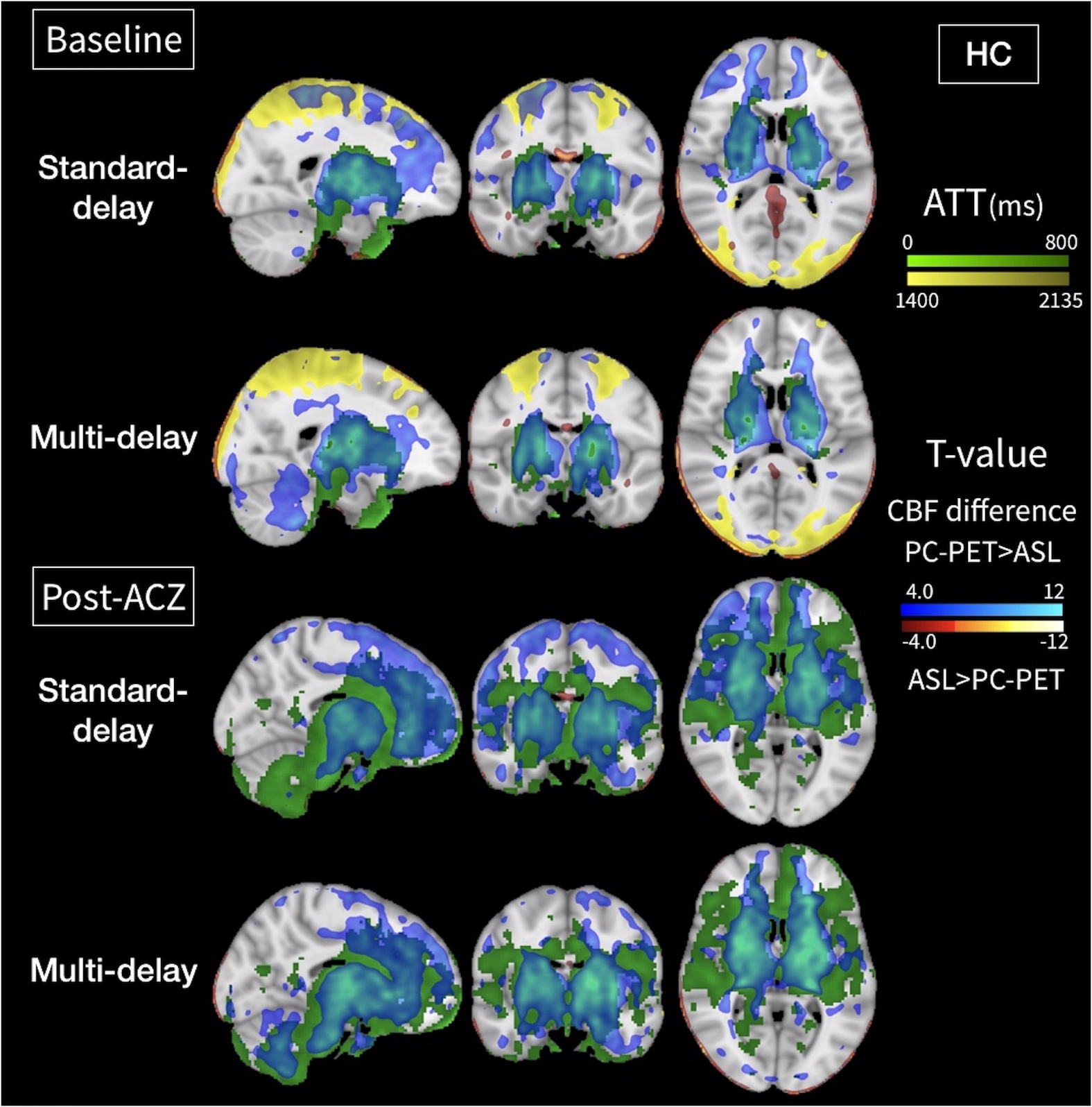
Relationship between voxel-wise parametric mapping and ATTs in healthy controls (HC). Voxel-wise parametric testing reveals areas of CBF under-estimation (blue) and over-estimation (red-orange) by each ASL method as compared to the PC-PET reference. Significant voxels are shown at the P=0.01 level (false discovery rate: 0.05). Green areas have ATT less than 800 ms, and yellow areas have ATT greater than 1400 ms.
At baseline, areas of CBF underestimation are primarily seen in the basal ganglia. Post-ACZ, the region with short ATT expanded to much of the anterior-circulation, and the extent of CBF underestimation by each ASL scan also expanded in the same regions.
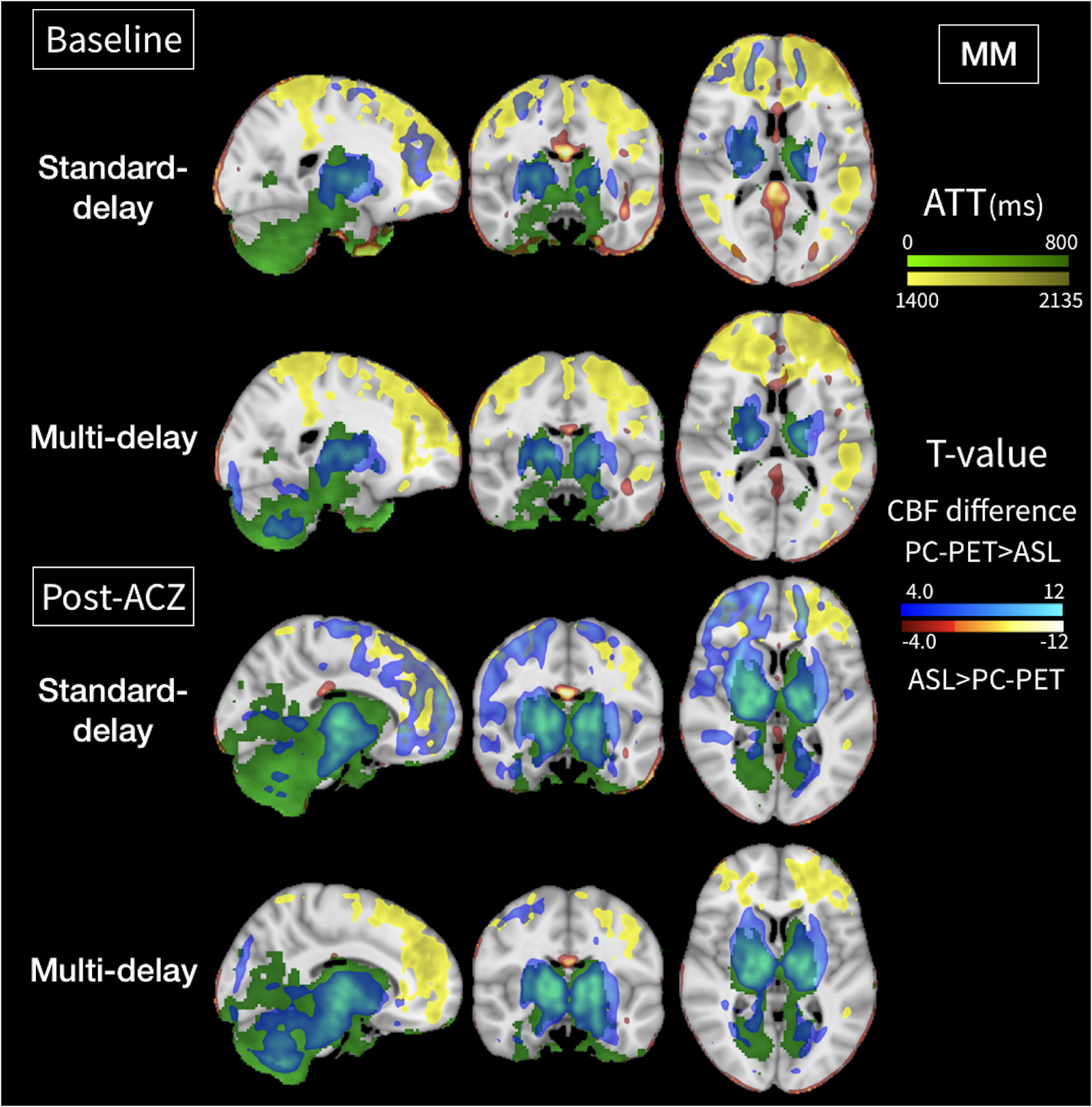
Relationship between voxel-wise parametric mapping and ATTs in Moyamoya patients (MM). Voxel-wise parametric testing reveals areas of CBF under-estimation (blue) and over-estimation (red-orange) by each ASL method as compared to PC-PET reference. Significant voxels are shown at P=0.01 level (false discovery rate: 0.05). Green areas have ATT less than 800ms, and yellow areas have ATT greater than 1400ms.
At baseline, areas of CBF underestimation by standard ASL are seen in some pathological areas with long ATT and in basal ganglia. Post-ACZ, the region with short ATT expanded in deep gray-matter and posterior circulation, and extent of CBF underestimation by multi-delay ASL expanded in same regions.