0286
Convolutional neural network uses pre-chemotherapy breast MRI data to predict which tumors will exhibit a pathologic complete response post-chemotherapy1Weill Cornell Medicine, New York, NY, United States, 2Memorial Sloan Kettering Cancer Center, New York, NY, United States
Synopsis
In this study, we evaluate the performance of a convolutional neural network (CNN) to predict pathologic complete response based on pre-treatment breast MRI images. We achieved moderate accuracy in this initial feasibility study. Future work with larger patient datasets will improve CNN performance.
Introduction
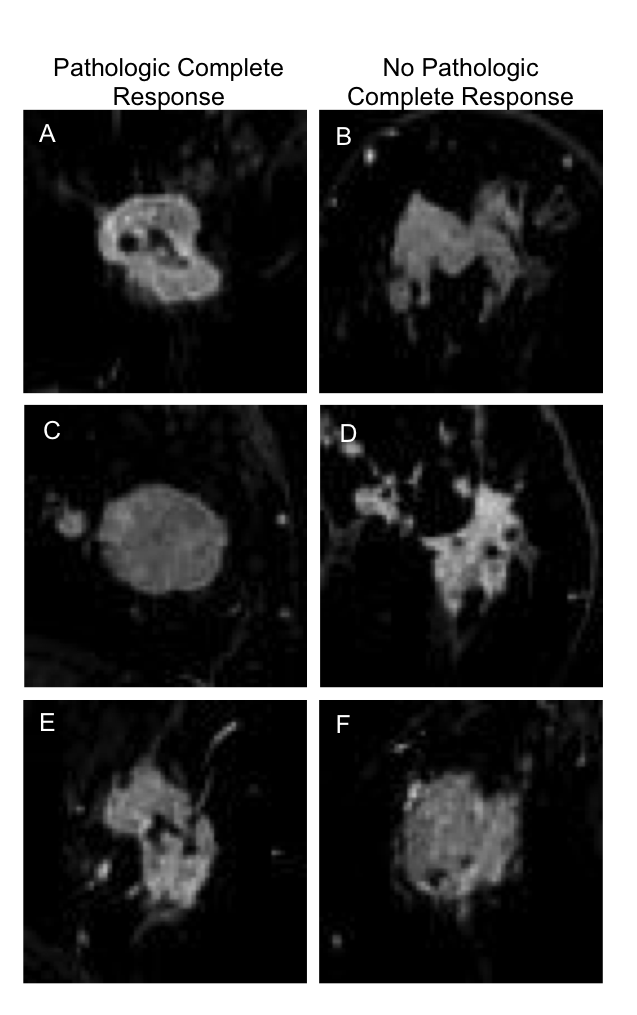
Neoadjuvant chemotherapy (NAC) is administered to breast cancer patients with locally advanced disease in an effort to downstage their tumor pre-operatively, thus permitting less extensive surgery and fewer surgical complications. Randomized controlled trials show that NAC induces a pathologic complete response (pCR) in a subset of patients, and several ongoing studies are evaluating the safety of eliminating surgery completely in patients with pCR.1,2 But predicting pCR based on preoperative imaging alone has proven challenging.3 Convolutional neural networks (CNNs) have recently emerged as a powerful tool for image classification and prediction.4 Unlike traditional machine learning methods that rely on a finite number of hand-crafted features, multi-layer non-linear CNN architectures permit automated extraction and amplification of CNN-derived complex features, which allow classification tasks to be performed in a highly complex subspace. In this work, we investigate the ability of a CNN to predict post-NAC pCR of breast tumors using pre-NAC breast MRI data.Methods
This retrospective Health Insurance Portability and Accountability Act (HIPAA)-compliant study received Institutional Review Board (IRB) approval and informed consent was waived. Between 2014-2017, 277 consecutive women 18 years of age or older with operable invasive carcinoma treated with NAC were consecutively identified with: (1) pre-NAC breast MRI, and (2) a post-NAC surgical pathology report assessing response. In this study, pCR (defined as no invasive or in situ disease) was determined based on the final surgical pathology report.
All patients underwent contrast-enhanced MRI on a 1.5 or 3.0 Tesla system (Discovery 750, GE Medical Systems, Waukesha, WI) with a dedicated 8- or 16-channel breast coil. Axial T1-weight fat-suppressed images were acquired pre-contrast and post-contrast after the intravenous administration of gadolinium-based contrast agent. Additional acquisition parameters include: TR/TE=7.9/4.3, flip angle=12° in-plane spatial resolution=1.1×1.1 mm, thickness=1.1 mm, temporal resolution=~120 seconds, axial orientation.
Two study radiologists performed single slice segmentation of the index breast cancer on the fat-saturated T1-weighted first post-contrast sequence from the pre-NAC MRI. All tumors were volumetrically segmented using a previously reported 3D tumor segmentation method [4]. Algorithm generated segmentations for all analyzed tumors were visually validated and corrected by a radiologist (EJS).
Based on these segmentations, a 3D ROI from the first post-contrast sequence was extracted that encased the tumor as well as surrounding breast tissue (see Fig 1). In axial, coronal and sagittal planes, 33 percent of slices – those containing the largest tumor cross-sectional areas – were resized to 64 x 64 and used for subsequent analysis. On average, 24 slices per tumor were extracted. Data augmentation was performed prior to training, including image translation, rotation, and magnification.
A CNN was designed using Python with Keras Toolbox and TensorFlow backend, and was run on a computer server using a NVIDIA GTX 1080ti GPU. The network architecture, displayed in Fig. 2, is a simplified version of VGG16,6 and includes several convolutional layers (3x3 filter size) with rectified linear unit (ReLU) activation, max pooling layers (2x2), fully connected layers, and a softmax activation yielding a binary output. The network was trained using the stochastic gradient descent optimizer to minimize binary cross entropy loss. Batch normalization was implemented after each convolutional layer, and dropout of 50% was utilized for regularization. Data was divided into 80 percent training, 10 percent validation, and 10 percent testing. For each subject, all images were assigned to either training, validation, or testing.
Results
Our CNN achieved a test set accuracy of 0.7 in identifying which tumors would exhibit a pathologic complete response after neoadjuvant chemotherapy.Discussion
Our results demonstrate the feasibility of training a CNN to predict pCR with moderate accuracy. Cancer treatment response is traditionally assessed only after treatment initiation. This work is part of a vanguard to make treatment response predictions prior to treatment delivery. Pre-treatment predictions could ultimately be used to determine which patients need which therapy when, and which patients can avoid certain treatments altogether. The major limitation of our study was the small sample size. Optimizing CNN performance requires large datasets. In future work, we will increase the number of patient cases to improve upon our model results.Conclusion
CNNs using pre-NAC breast MRI data can be trained to predict which patients will achieve post-NAC pathologic complete response with moderate accuracy. Future work with larger patient datasets will improve CNN performance.Acknowledgements
No acknowledgement found.References
1. Yee D, DeMichele A, Isaacs C, et al: Pathological complete response predicts event-free and distant disease-free survival in the I-SPY 2 trial. 2017 San Antonio Breast Cancer Symposium.
2. van la Parra RF, Kuerer HM. Selective elimination of breast cancer surgery in exceptional responders: historical perspective and current trials. Breast Cancer Res. 2016;18(1):28.
3. Weber JJ, Jochelson MS, et al. MRI and prediction of pathologic complete response in the breast and axilla after neoadjuvant chemotherapy for breast cancer. J Am Coll Surg. 2017 Dec;225(6):740-746.
4. Le Cun, Y, et al. Deep Learning. Nature. 2015; 521(7553):436-444.
5. Veeraraghavan H, Dashevsky BZ, Onishi N, et al. Appearance Constrained Semi-Automatic Segmentation from DCE-MRI is Reproducible and Feasible for Breast Cancer Radiomics: A Feasibility Study. Sci Rep. 2018;8(1):4838.
6. Simonyan, K. & Zisserman, A. Very deep convolutional networks for
large-scale image recognition. In Proc. International Conference on
Learning Representationshttp://arxiv.org/abs/1409.1556 (2014).
Figures