0285
Can Machine-Learning-based Radiomics of Whole Tumor on MR Multiparametric Maps Predict the Ki-67 index of Breast Cancer?1Radiology, Fudan University Shanghai Cancer Center, Shanghai, China, 2Radiology, Longhua Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai, China, 3MR Application Development, Siemens Shenzhen Magnetic Resonance, Shenzhen, China, Shenzhen, China, 4MR Application Predevelopment, Siemens Healthcare, Erlangen, Germany
Synopsis
There
has recently been increased interest in quantitative MR parameters for
assessing tumor proliferation. A total of 134 consecutive patients with
pathologically-proven invasive ductal carcinoma were retrospectively evaluated.
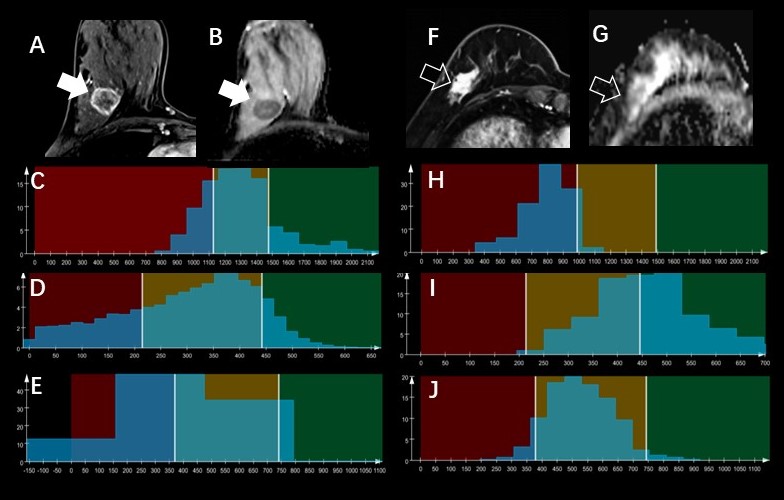
We extracted the whole-tumor histogram and textural features from an ADC map
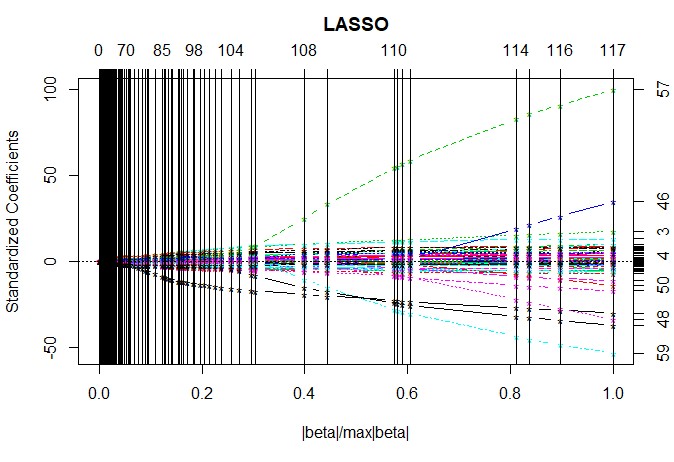
and DCE-MRI semi-quantitative maps. The LASSO for feature
selection and the KNN algorithm for classification were performed.
Classifications performed between Ki-67-positive and Ki-67-negative groups
resulted in an accuracy of 75.4% using three texture features, whereas
classification with only the entropy of ADC yielded an accuracy of 74.6%.
Introduction
Recent studies have shown that patients with a lower Ki67 index (less than 14%) more often undergo a complete pathological response (pCR) [1, 2]. Magnetic resonance (MR) image texture analysis–based radiomics have the potential to identify the Ki-67 status of breast cancer [3]. However, to our knowledge, no study has performed the texture analysis using both DCE and DWI images for predicting the Ki-67 status of breast cancer. The purpose of our study was to determine the feasibility of whole-tumor histogram and texture analysis, with the machine learning method, for identifying the Ki-67 status of invasive ductal carcinoma using quantitative ADC and DCE semiquantitative maps.Methods
This retrospective study included 134 patients with pathologically-confirmed invasive ductal carcinoma. All the MRI examinations were performed on a 3T scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany). The DWI sequence was executed using a fat-suppressed, single-shot, echo-planar imaging (EPI) sequence with the following parameters: TR/TE = 3000/54 ms; field of view = 340 x 340 mm2; matrix = 220 x 220; slice thickness = 6 mm; b-values = 0, 400, and 800 s/mm2; number of averages = 3, 4, and 5, respectively; parallel acquisition (GRAPPA) with acceleration factor of 3; and acquisition time = 2:09 min. DCE-MRI was obtained using a fat-suppressed T1-weighted 3D fast spoiled gradient-echo sequence (VIBE) before and five times continuously after contrast agent injection. The scan parameters were as follows: TR/TE = 4.5/1.6 ms; field of view = 340 x 340 mm2; flip angle = 10°; matrix = 384 x 384; slice thickness = 1.5 mm; GRAPPA acceleration factor = 3 and duration = 60 s for each phase. Whole-tumor histogram and textural features were extracted from the quantitative ADC map and DCE semi-quantitative maps (wash-in, washout, TTP, MIP, PEI) by using a prototype software (MR Multiparametric Analysis; Siemens Healthcare, Erlangen, Germany). The histogram features included mean, standard deviation, median, percentiles (5th, 95th), skewness, excess kurtosis and difference entropy. The textural features included difference variance, contrast, and entropy. A total of 66 features for all six maps were extracted to characterize the detected lesion regions. The least absolute shrinkage and selection operator (LASSO) algorithm was used for feature selection. k-nearest neighbor (KNN) classification was performed with k = 3, and internal validation was calculated using a 10-fold classification regime for the machine-learning-based classification by Weka (version 3.8.1, University of Waikato; Hamilton, New Zealand). The accuracy of classifications was assessed using the percentage of correctly classified data.Results
For lesions with a high Ki-67 index (more than 14%) versus lesions with a low Ki-67 (less than 14%), the entropy feature of the ADC map, skewness of the wash-in map, and difference variance of the PEI map were selected by the LASSO-based feature selection method (Fig.1). The accuracy for classification was 75.4% using three texture features and KNN-based machine learning. Notably, the accuracy for only the entropy feature of the ADC map was 74.6%.Discussion and Conclusion
The machine-learning-based radiomics of the whole tumor on ADC and DCE-related maps provides a non-invasive analytical approach for identifying the Ki-67 status of breast cancer. In our study, the best individual feature for prediction of Ki67 status was the entropy of ADC, which measures the image heterogeneity, reflecting the randomness of the difference in neighboring voxel gray levels. A possible explanation is that the entropy of ADC reflects the microenvironment of tumor structures, such as tumor cellularity, water content, the amount of fibrous stroma, and cell membrane integrity (4). The whole-tumor histogram and textural analysis based on the quantitative ADC map and DCE semi-quantitative maps might have potential to serve as a more convenient and noninvasive biomarker for the prediction of Ki-67 proliferation status.Acknowledgements
No.References
1. Fasching PA, Heusinger K, Haeberle L, et al. Ki67, chemotherapy response, and prognosis in breast cancer patients receiving neoadjuvant treatment. Bmc Cancer. 2011;11.
2. Kontzoglou K, Palla V, Karaolanis G, et al. Correlation between Ki67 and Breast Cancer Prognosis. Oncology-Basel. 2013;84(4):219-25.
3. Lee SH, Cho N, Kim SJ, et al. Correlation between high resolution dynamic MR features and prognostic factors in breast cancer. Korean J Radiol. 2008;9(1):10-8.
4. Koh DM, Collins DJ. Diffusion-weighted MRI in the body: applications and challenges in oncology. AJR Am J Roentgenol. 2007;188(6):1622-35.
Figures