0283
Pre-surgical evaluation of residual cancer by breast MRI after neoadjuvant systemic treatment: DWI-based algorism1Department of Diagnostic Imaging and Nuclear Medicine, Kyoto University graduate school of medicine, Kyoto, Japan, 2Kobe City Medical Center General Hospital, Kobe, Japan, 3Department of Pathology, Kyoto University Hospital, Kyoto, Japan, 4Department of Breast Surgery, Kyoto University Hospital, Kyoto, Japan
Synopsis
We aimed to re-evaluate DWI of pre-surgical MRI as a clue to diagnose pCR or non-pCR. DCE-MRI including kinetic information were also evaluated for comparison. DWI-based evaluation of residual disease in pre-surgical MRI demonstrate excellent diagnostic performance. On the other hand, residual disease is difficult to evaluate based on kinetic information. DWI-based evaluation of residual disease is a useful approach in pre-surgical evaluation of breast cancer following neoadjuvant systemic treatment.
Purpose
When the cancer shrinks and even disappears (pathological complete response: pCR) after preoperative neoajuvant systemic treatment (NST), surgery may be omitted. Breast MRI is used in evaluating residual cancer. However, accurate diagnosis of pCR is difficult due to various enhancement pattern after treatment (e.g. overdiagnosis by enhanced inflammatory reaction). Our preliminary analysis suggested that the accuracy of diagnosing pCR on MRI can be improved using DWI in addition to conventional dynamic contrast enhanced (DCE) MRI. This led to the hypothesis that pre-surgical evaluation based on DWI performs better than DCE-based diagnosis. This study aimed to re-evaluate DWI of pre-surgical MRI as a clue to diagnose pCR or non-pCR. DCE-MRI including kinetic information were also evaluated for comparison.Methods
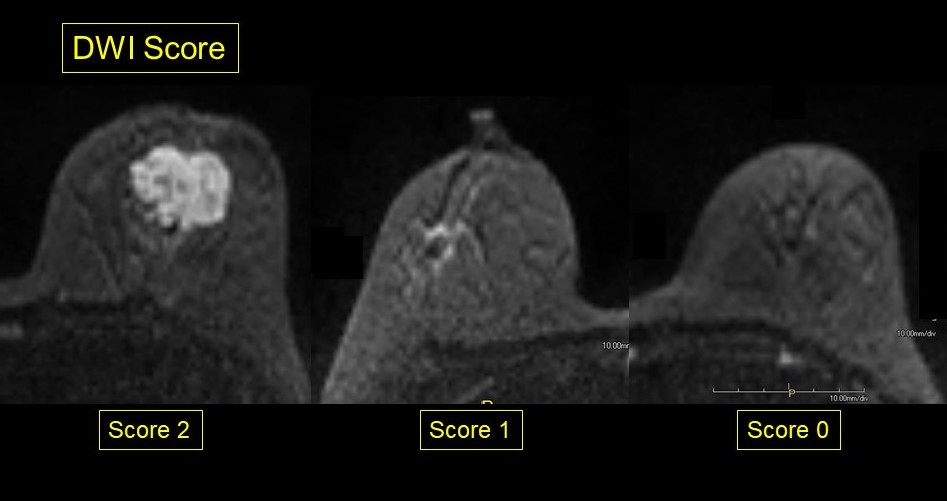
Patients who underwent pre-surgical MRI evaluation after NST in our hospital between 2014 and 2017 were searched through our hospital database. Those whose therapeutic grade was pathologically evaluated were included. MRI protocol: sequence: T1WI, T2WI, DWI (b=0, 1000 sec/mm2,) , Dynamic MRI (pre, 1-2, 5-6 min post-contrast), MRI was performed on Prisma /Trio Tim 3.0 Tesla scanner (Siemens AG, Erlangen, Germany) with 18 or 16 channel dedicated breast coils. Detailed parameters of DWI and Dynamic protocol are as follows: diffusion-weighted images (DWI) (axial single-shot EPI; TR/TE, 7000/62 ms; FOV, 330 × 160 mm: matrix, 166 × 80; thickness, 3.0 mm; NEX, 3), T1-weighted DCE images (axial VIBE with fat suppression; TR/TE, 3.70/1.36 ms; flip angle, 15°; FOV, 330 × 330 mm; matrix, 384 × 346; thickness, 1.0 mm). Their pre-surgical MRIs were retrospectively evaluated by two radiologists with 20 and 3 years’ experience of breast MRI. Initially, DWI of the target lesion was evaluated and categorized as 3-point scale (2: obvious high signal intensity, 1: small (<10mm) focus of high – intermediate signal intensity, 0: no abnormal signal). Then DCE MRI was evaluated including kinetic curve analysis by one of the radiologists. These results were compared to the post-surgical pathological evaluation in particular pCR or non-pCR. pCR was defined as no invasive carcinoma (in situ lesion allowed).Results
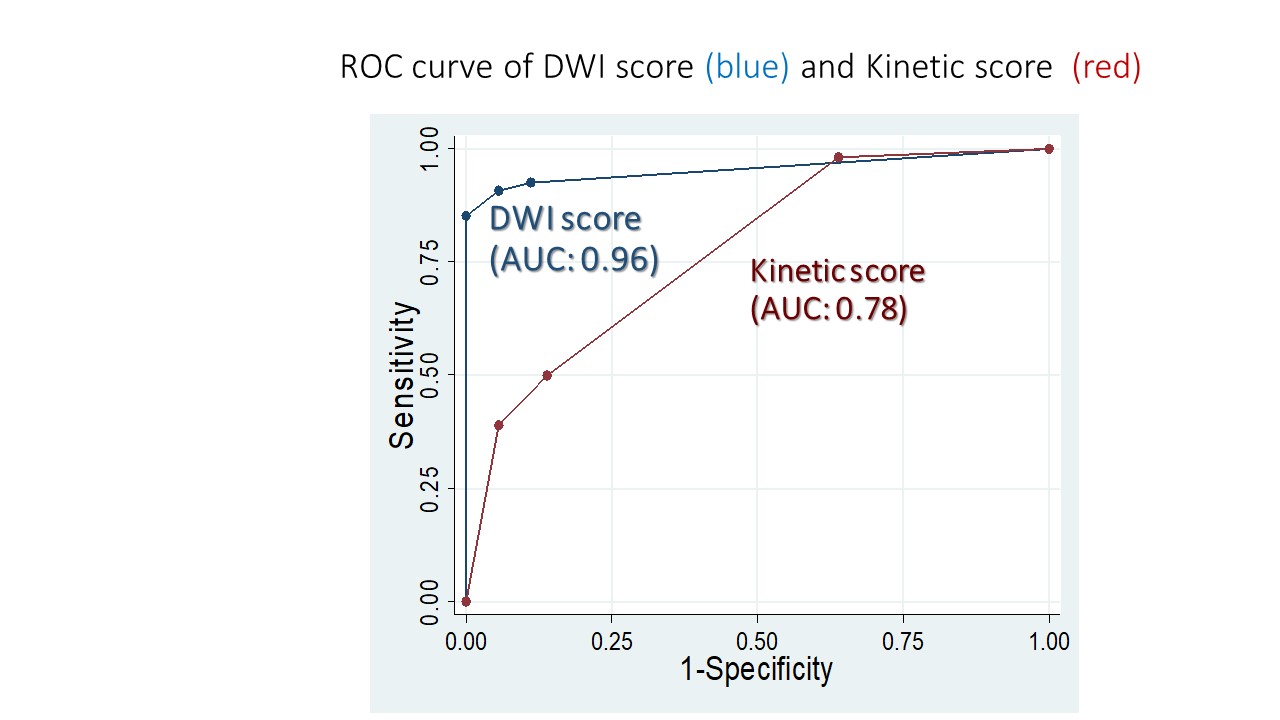
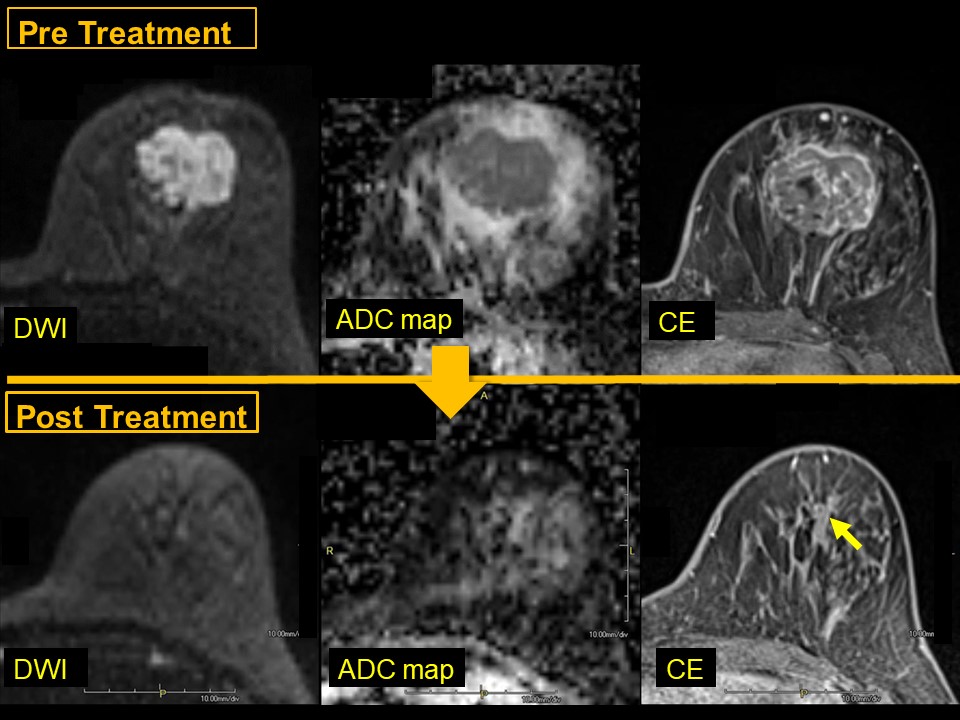
In total 95 patients were identified and their MRI were retrospectively reviewed. Among them, 40 % (38/95) of cases achieved pCR while 60% (58/95) were categorized as non-pCR on post-operative pathology evaluation. DWI score: the score of the two readers agreed on 91 lesions (96%) with kappa value of 0.93, suggesting excellent agreement. The mean score of the two readers were used for analysis. The number of patients scored as DWI 2,1, 0.5, 0 were 47, 7, 4 and 37. DWI score was strongly associated with residual disease. ROC analysis showed area under the ROC of 0.96 (95% Confidence interval: 0.92-0.99: figure 2). A cut-off value of score 1 or above resulted in sensitivity of 91% and specificity of 95%. The number of patients scored as kinetic 3,2,1 and 0 were 23, 9, 44 and 14 (5 patients were excluded due to lack of post contrast images or poor image quality). Area under the ROC of kinetic score was 0.78 (95% Confidence interval: 0.69-0.86: figure 2). False negative cases include two patients with invasive lobular carcinoma (one patient's MRI was shown in Case 2).Disucussion
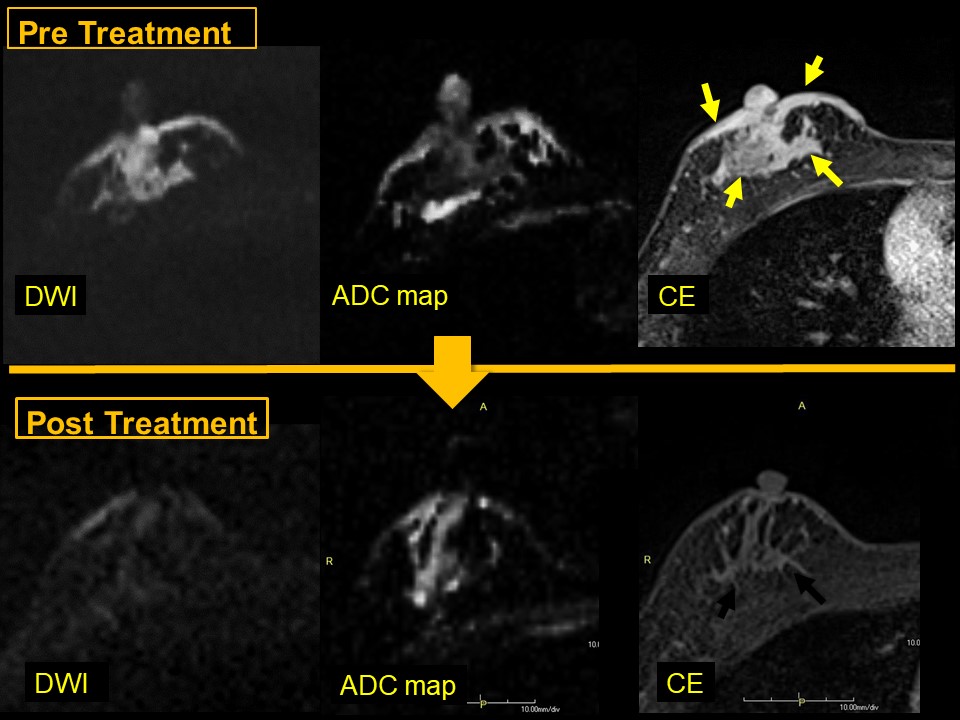
DWI-based evaluation of residual disease in pre-surgical MRI demonstrate excellent diagnostic performance, avoiding over-estimation of the enhanced fibrous tissues. On the other hand, residual disease is difficult to evaluate based on kinetic information. Possible reason of excellent performance in DWI score may be its association with the amount of cancer cells. Scar or fibrosis tended to be enhanced but to show lower signal on DWI at the end of the treatment. Our preliminary analysis indicated that overestimation may be reduced by careful examination based on DWI.Conclusion
DWI-based evaluation of residual disease is a useful approach in pre-surgical evaluation of breast cancer following neoadjuvant systemic treatment.
Acknowledgements
No acknowledgement found.References
1)Savannah C. Partridge, PhD, et al. Radiology 2018; 00: 1-11.
2) Savannah C. Partridge, PhD and Elizabeth S. McDonald, MD, PhD, et al. Magn Reson Imaging Clin N Am. 2013 August ; 21(3): 601–624. doi:10.1016/j.mric.2013.04.007.
3) Shangang Liu, et al. J. Magn Reson Imaging 2015; 42:779-787.
4) Wei Chu, et al. Oncotarget. 2017 Dec 11;9(6):7088-7100.
5) Madoka Iwase, et al. Breast Cancer, 2018 Apr4.doi:10.1007/s12282-018-0856-6.
6) Seigo nakamura, Mitsutomi Ishiyama, et al. Breast Cancer 14:123-130,2007.
Figures
Case 1: 40 years old woman who underwnt neoajuvant systemic treatment (NST) for grade 3 HR-/HER2+ disease. The post-treatment DWI score was 0 (no abnormal signal). She had no residual disease at surgery (pCR).