0282
Breast lesion classification accuracy using intravoxel incoherent motion diffusion modelling is improved by incorporating all parameters and informative Bayesian priors1Institute for Circulation and Medical Imaging, Norwegian University of Science and Technology (NTNU), Trondheim, Norway, 2Department of Radiology and Nuclear Medicine, St Olavs Hospital, Trondheim, Norway, 3Department of Physics, Norwegian University of Science and Technology (NTNU), Trondheim, Norway, 4Department of Radiology and Nuclear Medicine, St Olavs University Hospital, Trondheim, Norway
Synopsis
Strategies for intravoxel incoherent motion (IVIM) diffusion imaging acquisition and analysis are often framed in terms of curve-matching, whereas for breast lesions, classification accuracy against histopathologic assessment is a true metric of functional imaging performance. In this study, we show that IVIM diffusion modelling is best able to discriminate breast lesions (23 benign, 29 malignant) when using all parameters, and when derived from Bayesian methods employing either Gaussian shrinkage or local homogeneity priors, with ROC AUC values increasing from 0.83 (D, conventional least-squares) to 0.92 (D+f+D*, shrinkage prior).
Introduction
Accurate classification of breast lesions is important for disease management, and diffusion-weighted imaging (DWI) can provide functional characterization. Tissue microcapillary perfusion contributes to non-monoexponential signal attenuation in DWI data. The intravoxel incoherent motion (IVIM) model [1] attempts to characterize diffusion signal attenuation as biexponential, using a slow diffusion coefficient (D), a pseudodiffusion fraction (f), and a fast pseudodiffusion coefficient (D*). Analysis using this model is not trivial, however; conventional least-squares estimation of the pseudodiffusion parameters is highly sensitive to noise, especially in lightly perfused tissue such as the breast, and hence a raft of alternative estimators has been proposed [2]. In this work, we focus on the clinical utility of IVIM in breast lesion classification by assessing the performance of five different estimators on data acquired from breast cancer patients and comparing the associated receiver operator characteristic (ROC) curves.Methods
MRI data was acquired from 51 patients; 23 benign and 28 malignant tumours, classified by tissue histopathology (resected mass or biopsy) or radiological history. Images were acquired using a 3T Siemens Skyra (Erlangen, Germany) equipped with a 16-channel breast coil: twice-refocused spin-echo EPI; fat-suppressed (n=17 FatSat, n=34 SPAIR); TE/TR=86/9000ms; 90x90 matrix; 2x2mm in-plane resolution; 2.5mm slices; 60 slices; GRAPPA factor 2; 13 b-values (0, 10, 20, 30, 40, 50, 70, 90, 120, 150, 200, 400, 700s.mm-2); six (n=18) or three (n=33) directions; distortion-corrected [3]. Whole-lesion ROIs were drawn by a basic scientist advised by a breast radiologist, with reference to DCE images; largest cross-section slices were used to compare fitting methods.
IVIM parameters were estimated for every pixel in every ROI using five approaches:
LSQ – Standard nonlinear least squares (trust-region-reflective algorithm).
SEG – Segmented partially-linearized least squares (two-step fit to high/low b-value data).
BUP – Bayesian inference with a minimally-informative uniform prior [4] and a Markov chain Monte Carlo (MCMC) implementation (estimates from posterior mode).
BSP – Bayesian inference with a Gaussian “shrinkage” prior [5], which assumes each parameter is approximately Gaussian distributed over the entire ROI (MCMC implementation; estimates from posterior mean).
FBM – Bayesian inference with a spatial homogeneity “smoothing” prior [6], optimized using the fusion bootstrap moves approach based on minimum graph cuts.
Parameter estimates were constrained in all approaches: f [5x10-4, 0.5]; D [4.5x10-5, 3x10-3] mm2s-1; D* [3.4x10-4, 0.3] mm2s-1. Differences in parameter estimates between approaches were assessed using Kruskal-Wallis, Mann-Whitney, and correlation tests. Estimator precision was assessed using the coefficient of variation (CV) across each ROI (patient-averaged). The ability to differentiate between benign and malignant lesions was assessed using area under the curve (AUC) for ROC curves. All analysis was performed using MATLAB (Mathworks).
Results and Discussion
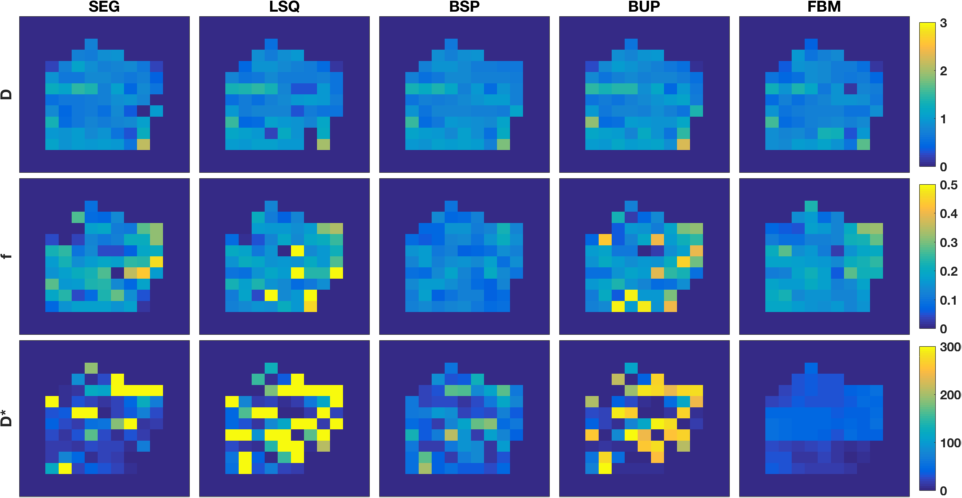
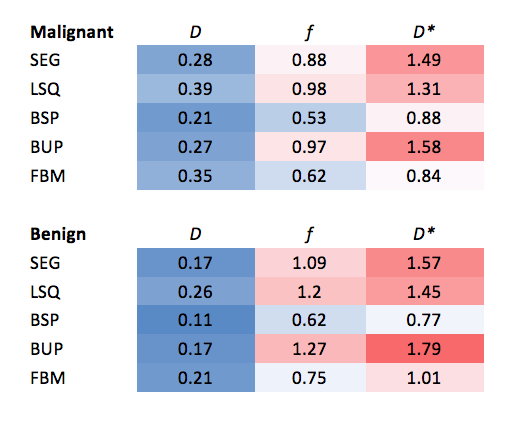
Figure 1 displays IVIM parameter maps obtained by each approach for one malignant example lesion; maps for D are found to be very similar for all approaches, whereas increased variability and outlier frequency are observed in maps for f and particularly D* using LSQ, SEG, and BUP. BSP and especially FBM generally resulted in lower variability. CV analysis (Table 1) supported these trends in estimator precision across all patients for both lesion types.
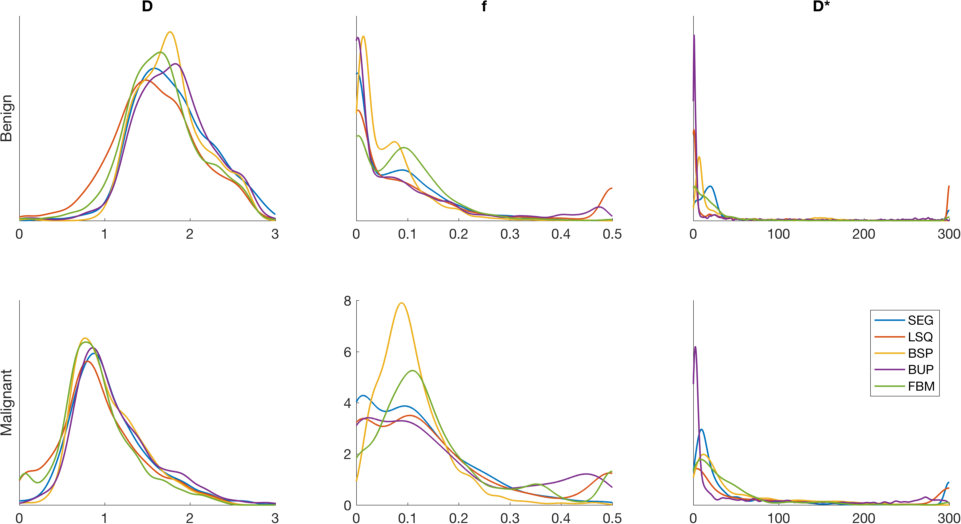
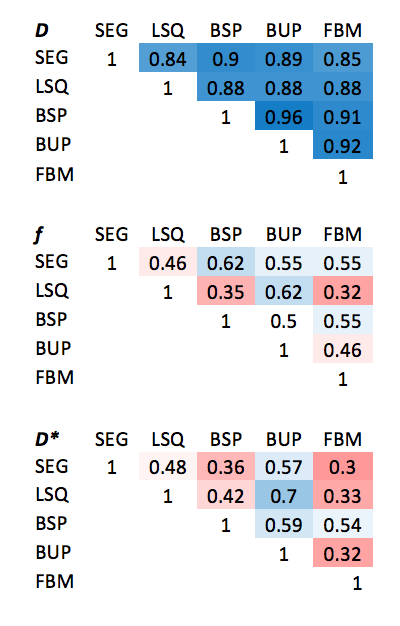
Figure 2 displays histograms of parameter estimates across all voxels of every patient for each approach and lesion type. All approaches confirmed that malignant lesions are characterized by higher f and lower D than benign lesions. While the majority of histograms were found to be statistically significantly different due to the large datasets involved, estimates for D showed strong correlation (Table 2) between methods (0.84-0.96), whereas f and D* were generally only weakly correlated between methods (0.3-0.7).
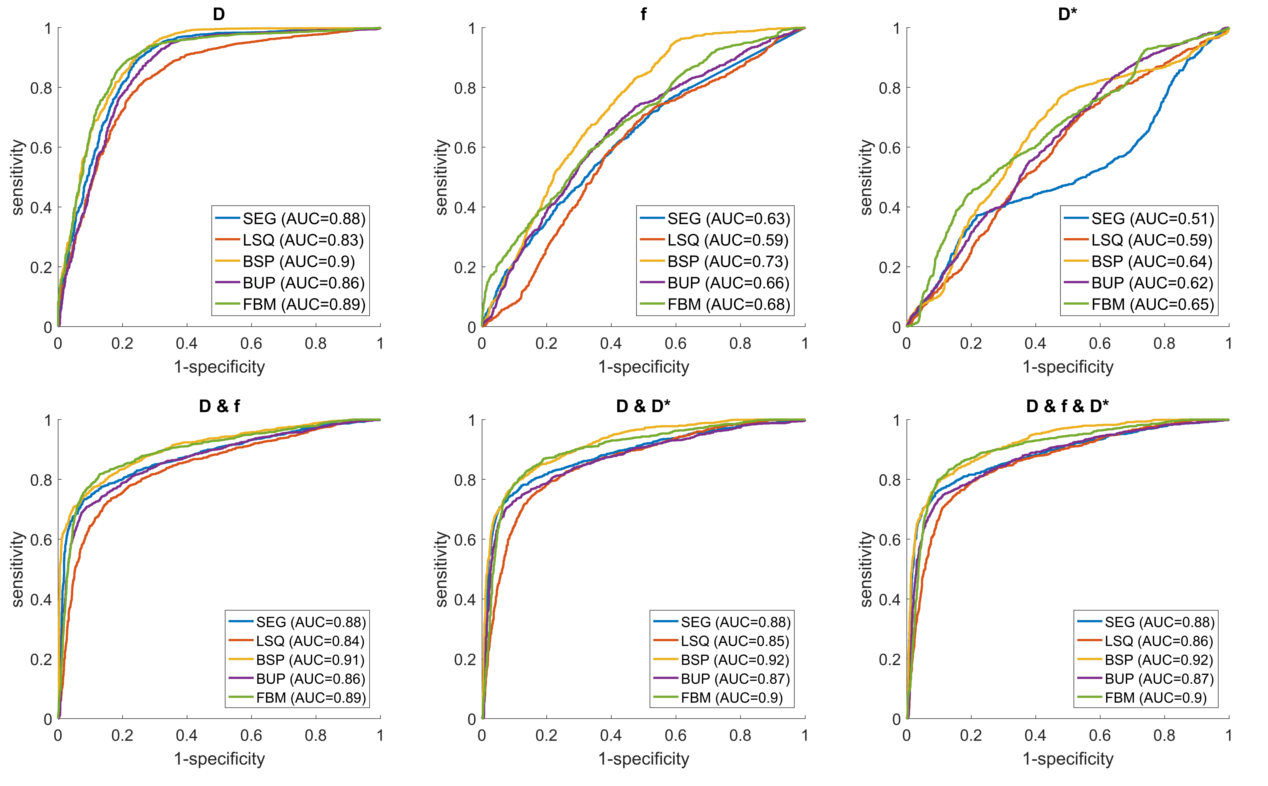
Figure 3 displays ROC curves for the differentiation of malignant and benign lesions using individual IVIM parameter estimates, or combinations thereof, obtained by each approach. As expected, D was by far the most powerful distinguishing single parameter; inclusion of f and/or D* provided slight improvement in AUC across all methods (max. +0.03). BSP and FBM algorithms provided consistently the highest AUC (up to 0.92), whereas LSQ typically provided the lowest. SEG estimates for D and f in combination, obtained using data at only 4 of the b-values, provided a competitively high AUC of 0.88.
Conclusion
Bayesian estimation of IVIM parameters in breast tumours using global shrinkage or local smoothing priors provides clear improvements in both precision and the ability to differentiate between benign and malignant lesions beyond conventional fitting methods. Inclusion of f and D* confers a small additional advantage over D alone in all fitting methods (except SEG), however this benefit comes at the cost of increased scan time, and therefore should be evaluated in context when implementing clinical IVIM protocols.Acknowledgements
We acknowledge support from the liaison Committee between the Central Norway Regional Health Authority and the Norwegian University of Science and Technology. We are grateful to Matthew R. Orton for useful insight on the Gaussian shrinkage prior.References
1. Le Bihan D, Breton E, Lallemand D, et al. (1988) Separation of diffusion and perfusion in intravoxel incoherent motion MR imaging. Radiology 168:497–505.
2. While PT (2017) A Comparative Simulation Study of Bayesian Fitting Approaches to Intravoxel Incoherent Motion Modeling in Diffusion-Weighted MRI. Magn Reson Med 78:2373–2387.
3. Teruel JR, Fjøsne HE, Østlie A, et al. (2015) Inhomogeneous static magnetic field-induced distortion correction applied to diffusion weighted MRI of the breast at 3T. Magn Reson Med 74:1138–1144.
4. Gustafsson O, Montelius M, Starck G, Ljungberg M (2018) Impact of prior distributions and central tendency measures on Bayesian intravoxel incoherent motion model fitting. Magn Reson Med 79:1674–1683.
5. Orton MR, Collins DJ, Koh D, Leach MO (2014) Improved Intravoxel Incoherent Motion Analysis of DiffusionWeighted Imaging by Data Driven Bayesian Modeling. Magn Reson Med 71:411–420.
6. Freiman M, Perez-Rossello JM, Callahan MJ, et al. (2013) Reliable estimation of Incoherent Motion parametric maps from diffusion-weighted MRI using fusion bootstrap moves. Med Image Anal 17:325–36.
Figures