0279
Improved lesion conspicuity and confidence level through suppressed background parenchymal enhancement in ultrafast breast dynamic contrast enhanced MRI1Diagnostic Imaging and Nuclear Medicine, Graduate School of Medicine, Kyoto University, Kyoto, Japan, 2Siemens Healthcare GmbH. , Erlangen, Germany, 3Breast surgery, Graduate School of Medicine, Kyoto University, Kyoto, Japan
Synopsis
Ultrafast dynamic contrast enhanced (UF-DCE) MRI is known for its reduced background parenchymal enhancement (BPE), but the evidence is limited. We evaluated BPE, lesion conspicuity and confidence level of UF-DCE MRI compared with those of conventional DCE (C-DCE) MRI. BPE was reduced, and lesion conspicuity and confidence level were improved on UF-DCE MRI compared to C-DCE MRI, indicating another advantage of UF-DCE MRI when applied to younger women and for high-risk screening.
Introduction
Background parenchymal enhancement(BPE) can obscure enhancing breast lesions and interfere with MRI interpretation. Ultrafast dynamic contrast enhanced(UF-DCE) MRI is actively investigated due to its shorter scanning time1,2). Another benefit of UF-DCE can be its reduced BPE with easier lesion detection, but the evidence is limited3, 4). We aimed to evaluate BPE, lesion conspicuity and confidence level of UF-DCE MRI compared with those of conventional DCE(C-DCE) MRI.Methods
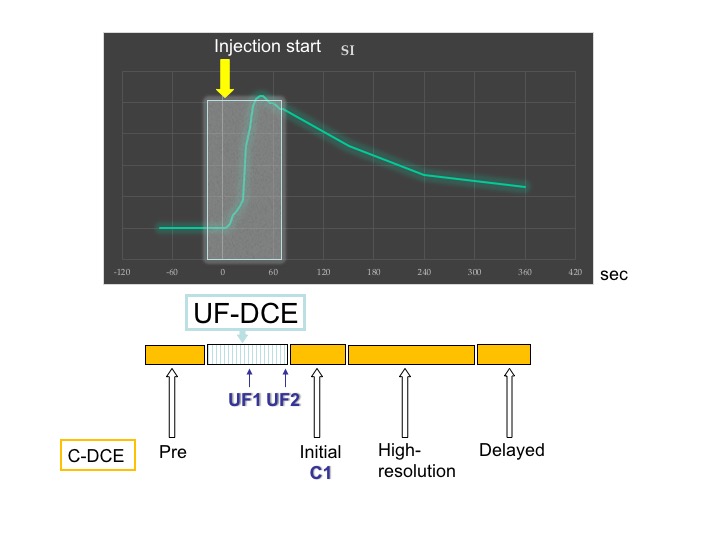
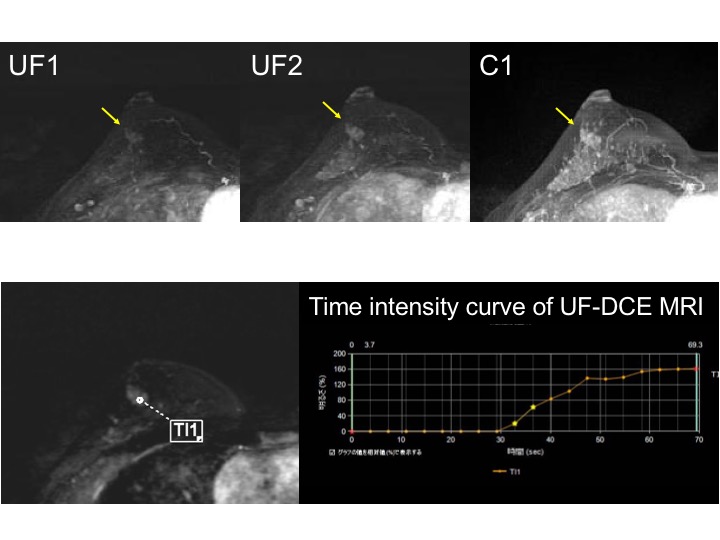
Study Population: Our study population consisted of consecutive female patients under 50 y.o. who underwent breast MRI with the UF-DCE protocol from April 2016 to May 2018 with histopathological diagnosis. One patient was excluded because of subtraction artifacts. A total of 32 females with 39 enhancing lesions(21 malignant and 18 benign) were included. MR Protocol: MR examinations were performed using a 3T scanner(MAGNETOM Prisma or Skyra, Siemens Healthcare, Erlangen, Germany) with a 18/16-channel dedicated bilateral breast coil. Gadobutrol(Gadovist, Bayer. Germany) was intravenously infused at a dose of 0.1ml/kg and at a rate of 2.0ml/sec, followed by 20ml of saline at the same rate. The DCE MR protocols were as follows: 1.pre phase; 2.UF-DCE MRI(15 sec before contrast injection-60 sec after contrast injection, 2 sec preparation time followed by 3.7 sec/frame×continuous 20 frames); 3.initial phase DCE MRI, 60-120 sec after contrast injection; 4.high spatial-resolution DCE MRI, 120-300 sec after contrast injection; 5.delayed phase DCE MRI, 300-360sec after contrast injection. UF-DCE MRI was acquired by a prototype based on the 3D gradient-echo VIBE sequence using a compressed sensing(CS) reconstruction(TR/TE 5.0/2.5ms, FA 15degrees, FOV 360 mm×360 mm, matrix 384×269, thickness 2.5 mm, CS acceleration=16.5, temporal resolution 3.7 sec/frame, 20 time frames). CS reconstruction was performed with 30 iterations, based on a separate retrospective evaluation of the convergence speed. Image Analysis: Using 12th and 20th frame(time point UF1 and UF2 respectively, see figure 1) images of UF-DCE MRI, we reconstructed 2 maximum intensity projection(MIP) images from subtracted images by subtraction from the 1st frame. Also using initial phase(time point C1) of C-DCE MRI, we reconstructed 1 MIP image from subtracted image by subtraction from the pre-phase image. These procedures were performed at a workstation(Aquarius NET Viewer; TeraRecon, Foster City, CA). Two independent radiologists evaluated BPE, lesion conspicuity and confidence level of these 3 MIP images in each case. BPE was graded as 1(minimal), 2(mild), 3(moderate) and 4(marked) based on the severity and matched to the BI-RADS 2013 lexicon. Lesion conspicuity was graded as 3(well visualized), 2(poorly visualized) and 1(non-visualized), meaning higher grade for better conspicuity. Confidence level was graded as 3(high), 2(middle) and 1(low), indicating higher grade for better diagnostic confidence. These grades were compared using Wilcoxon signed rank test with Bonferroni correction.Results
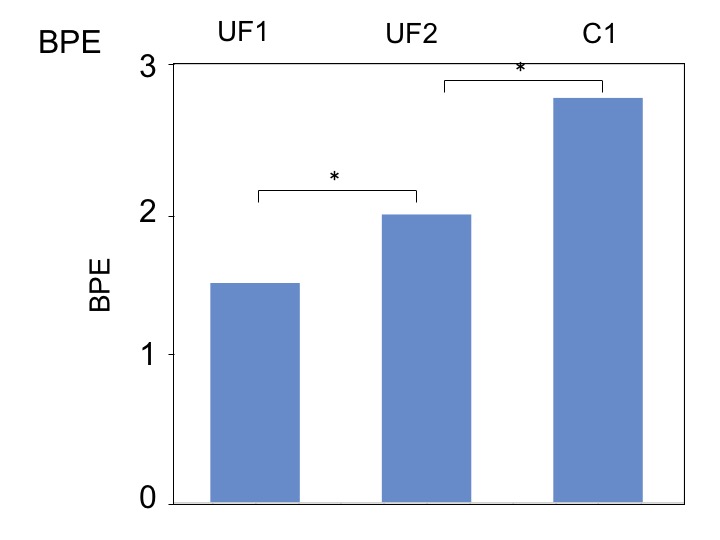
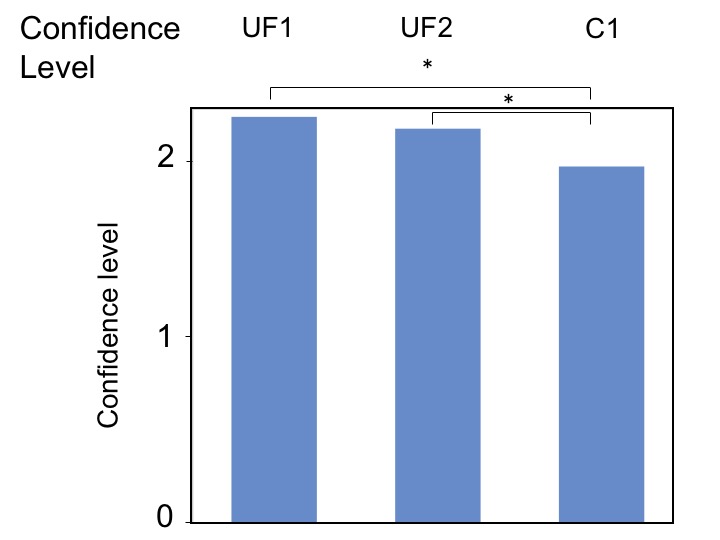
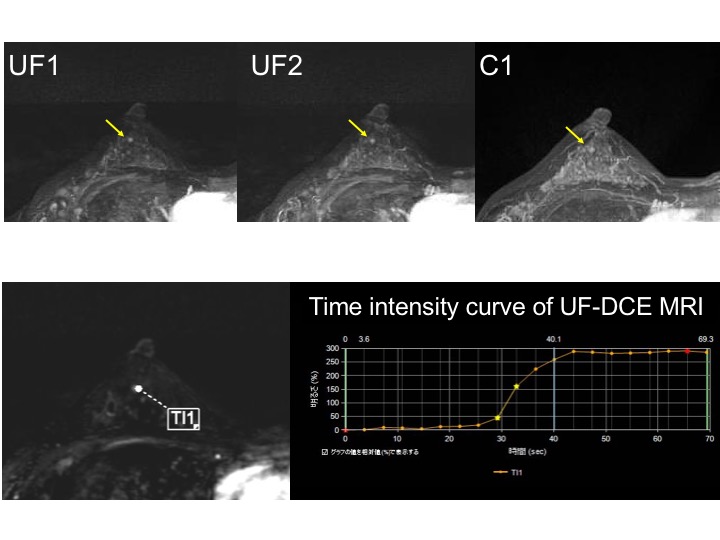
Good inter-rater agreement was obtained for all the evaluation items. Average grades of BPE were 1.50(UF1), 1.97(UF2) and 2.77(C1), showing less BPE at an earlier timing(figure 2). In terms of BPE, all the differences between each image were significant(p<0.05). Average grades of lesion conspicuity were 2.51(UF1), 2.49(UF2) and 2.29(C1), and those of confidence level were 2.21(UF1), 2.14(UF2) and 1.94(C1), suggesting better conspicuity and confidence level at an earlier phase(figure 3). Images obtained at UF1 and UF2 demonstrated significantly better confidence level(UF1 versus C1 p=0.026, UF2 versus C1 p=0.028). There are particular cases in which UF-DCE performed better in diagnosis. Two benign lesions(usual ductal hyperplasia(UDH) and tubular adenoma) with grade 4 BPE were not visualized on C1 but showed grade 3 conspicuity on UF1 and UF2 images(figure 4). Eight lesions including 5 malignant lesions showed better conspicuity or confidence level on UF1 and UF2 than on C1 image. Three benign lesions(FA, UDH and fibrocystic change) with grade 3-4 BPE had the highest conspicuity or confidence level on UF2 images(figure 5). On the other hand, 1 intradutal papilloma and 1 fibroadenoma(FA) were not visualized on any image. There was no lesion that was not visualized on UF-DCE MR images but visualized on C1 image.Discussion
The results of our study targeted at younger women(<50 y.o.) demonstrated that UF-DCE MRI showed less BPE, better lesion conspicuity and better diagnostic confidence compared with initial phase images. Some lesions could even be detected only on UF-DCE MRI, which may be due to its reduced BPE. Some benign lesions with low vascularity were best visualized on their 20th frame of UF-DCE MRI, which may be due to the best balance of their persistent enhancement and reduced BPE. The results indicate the advantage of UF-DCE MRI among younger population.Conclusion
Breast images with less BPE can be obtained using UF-DCE MRI in younger women, which lead to better lesion conspicuity and confidence level in some lesions. As a future prospect, UF-DCE MRI may be useful for speedy breast screening especially in younger women.Acknowledgements
The authors would like to thank Ms. Elisabeth Weiland from Siemens Healthcare GmbH. for the excellent support.References
1. Mann RM, et al. A novel approach to contrast-enhanced breast magnetic resonance imaging for screening: high-resolution ultrafast dynamic imaging. Invest Radiol, 2014. 49(9): p. 579-85.
2. Kuhl CK, S.S. Strobel K, et al. Abbreviated Breast Magnetic Resonance Imaging(MRI): First Postcontrast Subtracted Images and Maximum-Intensity Projection—A Novel Approach to Breast Cancer Screening With MRI. Journal of Clinical Oncology, 2014. 32(22).
3. Abe H, et al. Kinetic Analysis of Benign and Malignant Breast Lesions With Ultrafast Dynamic Contrast-Enhanced MRI: Comparison With Standard Kinetic Assessment. AJR Am J Roentgenol, 2016. 207(5): p. 1159-1166.
4. Goto M, et al. Diagnostic performance of initial enhancement analysis using ultra-fast dynamic contrast-enhanced MRI for breast lesions. Eur Radiol, 2018:1-11.
Figures