0265
Impact of attenuation correction on image-derived input function and cerebral blood flow quantification with simultaneous [15O]-water PET/MRI1Oslo University Hospital, Oslo, Norway, 2Radiology, Stanford Unversity, Stanford, CA, United States, 3GE Global Research, Bangalore, India, 4Neurosurgery, Tokyo Medical and Dental University, Tokyo, Japan
Synopsis
This study evaluated the impact of attenuation correction (AC) on image-derived input functions (IDIF) and kinetic modeling of cerebral blood flow (CBF) parameters for simultaneous [15O]-water PET/MRI in the brain. Atlas-based AC led to 4.3% underestimation of the IDIF peak and 8-18% overestimation of absolute CBF in different brain perfusion states. On the other hand, zero echo time (ZTE)-based AC provided reproducible quantification of absolute CBF, comparable to the deep learning AC reference that was trained on real CT images. Attenuation correction is an important consideration for IDIF calculation and parametric mapping with PET/MRI; and ZTE-based and deep learning-based AC provide suitable quantitative accuracy for [15O]-water studies.
Introduction
Considerable technical advances have improved and sought to harmonize attenuation correction (AC) for simultaneous PET/MRI in the brain1, but few studies have evaluated the impact of AC on PET kinetic modeling and parameter quantification. In particular, image-derived input function (IDIF) methods can reduce the invasiveness of quantitative PET studies by removing the need for arterial blood sampling2. However, brain IDIFs typically derive from large supplying arteries such as the internal carotids, which are located near the skull base and thus highly susceptible to attenuation effects of bone. This simultaneous PET/MRI study evaluates the effect of attenuation correction on IDIF, kinetic modeling of absolute cerebral blood flow (CBF) values, and measurement reproducibility with [15O]-water tracers.Methods
Acquisition: Simultaneous time-of-flight 3 Tesla PET/MRI (GE Healthcare Signa) was acquired in eight healthy volunteers (ages 22-66 years, 6 female). PET imaging of CBF was performed using manual injection of [15O]-water (833±148 MBq) before and after administration of Diamox, a vasodilator that augments CBF. Four volunteers underwent two successive scans at baseline to evaluate scan-rescan reproducibility.
Image reconstruction: Dynamic [15O]-water PET frames were reconstructed (30x1s, 10x3s, 12x5s, 6x10s) with three different AC methods:
- Atlas-based method3 using a two-point Dixon MRI;
- Zero echo time (ZTE)-based method4 that segments tissue on a ZTE MRI (nominal echo time of 0ms, 1.17mm in-plane resolution) and assigns continuous attenuation values to bone;
- Deep learning network that takes a single input channel (ZTE MRI) and outputs a pseudo-CT image that was trained on real CT images previously in a separate group of 50 patients5.
The deep learning AC method was considered the reference standard in this study because it has demonstrated visual and quantitative accuracy to CT, especially in bone, across multiple sites5.
CBF quantification: IDIFs were created for each AC method within the cervical arteries, correcting for spill-over effects with the true arterial volume (segmented on MR angiogram)2. All dynamic PET data were spatially normalized to the Montreal Neurological Institute (MNI) template in PMOD 3.5 using individual T1-weighted MRI, and time activity curves were extracted from pre-defined volumes of interest (brainstem, white matter, frontal, temporal, parietal, occipital, insula, cerebellum, central) previously shown to be influenced by AC6. Quantitative PET CBF (ml/100g/min) maps then were generated by kinetic modeling with a one-tissue compartment model to provide absolute baseline CBF, post-Diamox CBF, and cerebrovascular reactivity (% increase in CBF).
Statistics: Mixed effect models were used to evaluate CBF and cerebrovascular reactivity using AC type (deep learning, ZTE, atlas) as a fixed effect and subject as a random effect in R (3.4) software. Coefficients of variation were used to compare scan-rescan reproducibility and inter-subject variation of CBF between AC methods.
Results
The deep learning network produced high quality pseudo-CT images; ZTE- and deep learning-based attenuation maps preserved bone structures in the skull base and cervical spine that were not well defined on atlas-based attenuation maps (Figure 1). As a result, atlas-based AC underestimated the IDIF peak by 4.3% (P=0.003), and by as much as 20% in an individual subject, compared to ZTE- and deep learning AC (Figure 2).
Mixed effects regression (Figure 3) revealed that kinetic modeling with atlas-based AC led to overestimation of baseline CBF by 5.4 ml/100g/min (8.0%, P<0.0001) and of post-Diamox CBF by 15.5 ml/100g/min (18.4%, P=0.0001) compared to deep learning AC. Similarly, atlas-based AC led to overestimation of cerebrovascular reactivity by 19.8% (P=0.02). No statistical differences were observed in CBF or cerebrovascular reactivity between ZTE-based AC and the deep-learning AC reference.
In subjects with repeated acquisitions, scan-rescan coefficient of variation (CoV) of the baseline CBF measurements was low (~10%) and not different between the AC types (Figure 4). However, inter-subject CoV of baseline CBF was greater for atlas-based AC by 14.0% (P<0.0001), compared to ZTE- and deep learning AC methods.
Discussion and Conclusion
Atlas-based AC led to underestimation of IDIF peak values compared to ZTE- or deep learning-based approaches, likely because the IDIF curves derive from cervical arteries close to the skull base that were not well characterized on atlas-based AC maps. Underestimation of the IDIF peak directly impacted the kinetic modeling, leading to CBF overestimation from dynamic [15O]-water PET images reconstructed with atlas-based AC, in various brain perfusion states. Furthermore, the high inter-subject CoV of atlas-based CBF measurements suggests that atlas-based AC contributes additional subject-dependent variance unrelated to perfusion (a confounder). On the other hand, ZTE-based AC provided reproducible quantification of absolute CBF, comparable to the deep learning AC reference that was trained on real CT images. Attenuation correction is an important consideration for IDIF formation and parametric mapping with kinetic modeling for PET/MRI; and ZTE-based and deep learning-based AC provide suitable quantitative accuracy for [15O]-water studies.
Acknowledgements
GE Healthcare, NINDS 1K99NS102884References
- Ladefoged CN, Law I, Anazodo U, et al. "A multi-centre evaluation of eleven clinically feasible brain PET/MRI attenuation correction techniques using a large cohort of patients." Neuroimage 147 (2017): 346-359.
- Khalighi MM, Deller TW, Fan AP et al. "Image-derived input function estimation on a TOF-enabled PET/MR for cerebral blood flow mapping." Journal of Cerebral Blood Flow & Metabolism 38.1 (2018): 126-135.
- Sekine T, Buck A, Delso G, et al. Evaluation of atlas-based attenuation correction for integrated PET/MR in human brain: Application of a head atlas and comparison to true CT-based attenuation correction. J Nucl Med 57 (2016): 215-220.
- Delso G, Carl M, Wiesinger F, et al. Anatomic evaluation of 3-dimensional ultrashort-echo-time bone maps for PET/MR attenuation correction. J Nucl Med 55.5 (2014): 780-785.
- Kaushik S, Cozzini C, Bylund M, et al. Deep learning based pseudo-CT computation and its application for PET/MR attenuation correction and MR-guided radiation therapy planning. Proc Int Soc Magn Reson Med, Paris France (2018): 1253.
- Khalifé M, Fernandez B, Jaubert O, et al. Subject-specific bone attenuation correction for brain PET/MR: can ZTE-MRI substitute CT scan accurately? Physics in Medicine & Biology, 62.19 (2017): 7814.
Figures
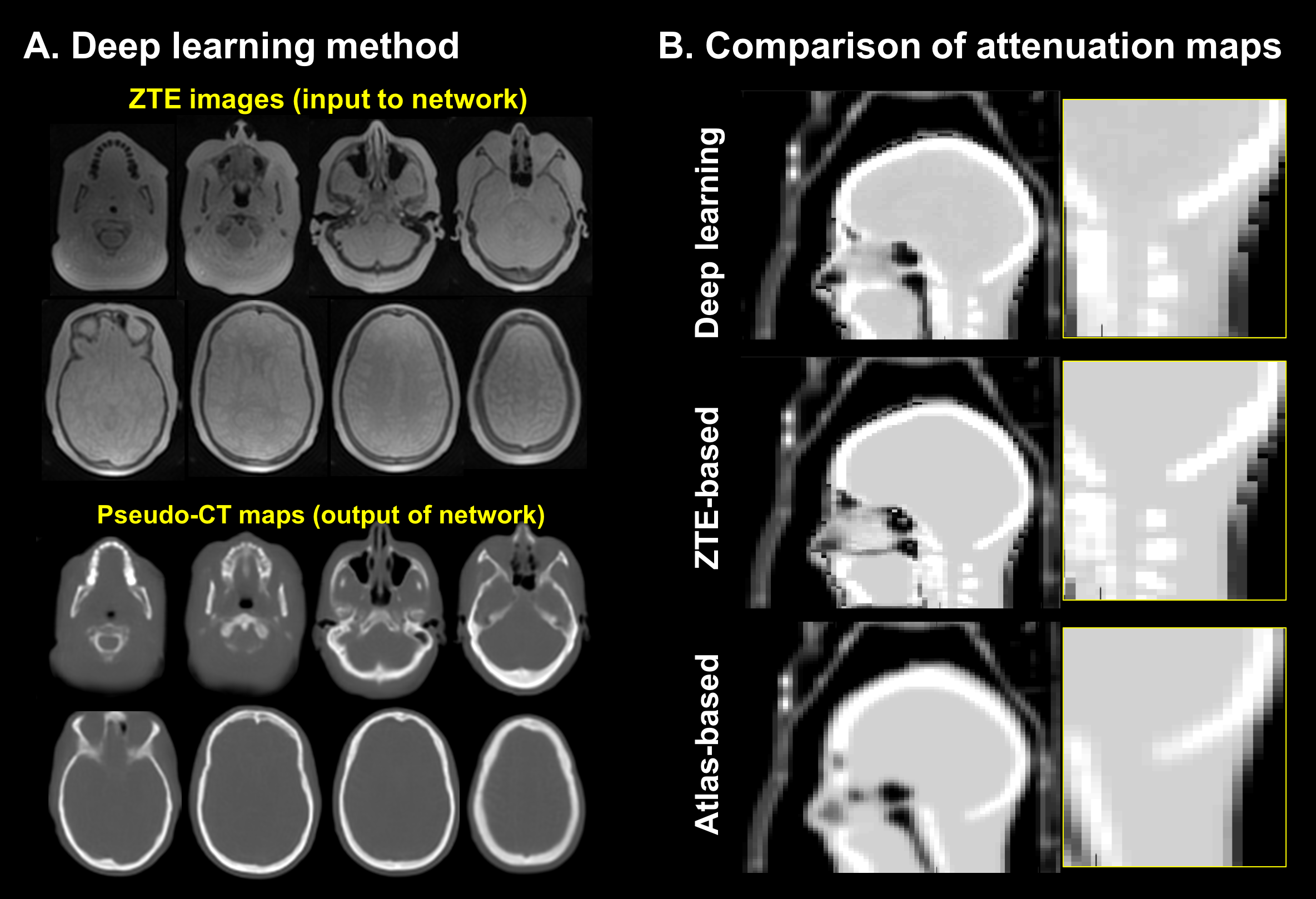
Figure 1. (a) Pseudo-CT images were synthesized from a deep learning network with a single channel input (ZTE images) previously trained on real CT images, and showed high fidelity to bone structures.
(b) Attenuation correction (AC) maps generated for the same volunteer from the deep learning method (the reference standard for this study), ZTE segmentation, and atlas-based approaches (based on two-point Dixon MRI). The ZTE- and deep learning-based AC maps depict skull base and cervical spine structures, which are not well-visualized and are quantitatively underestimated on the atlas-based AC map.
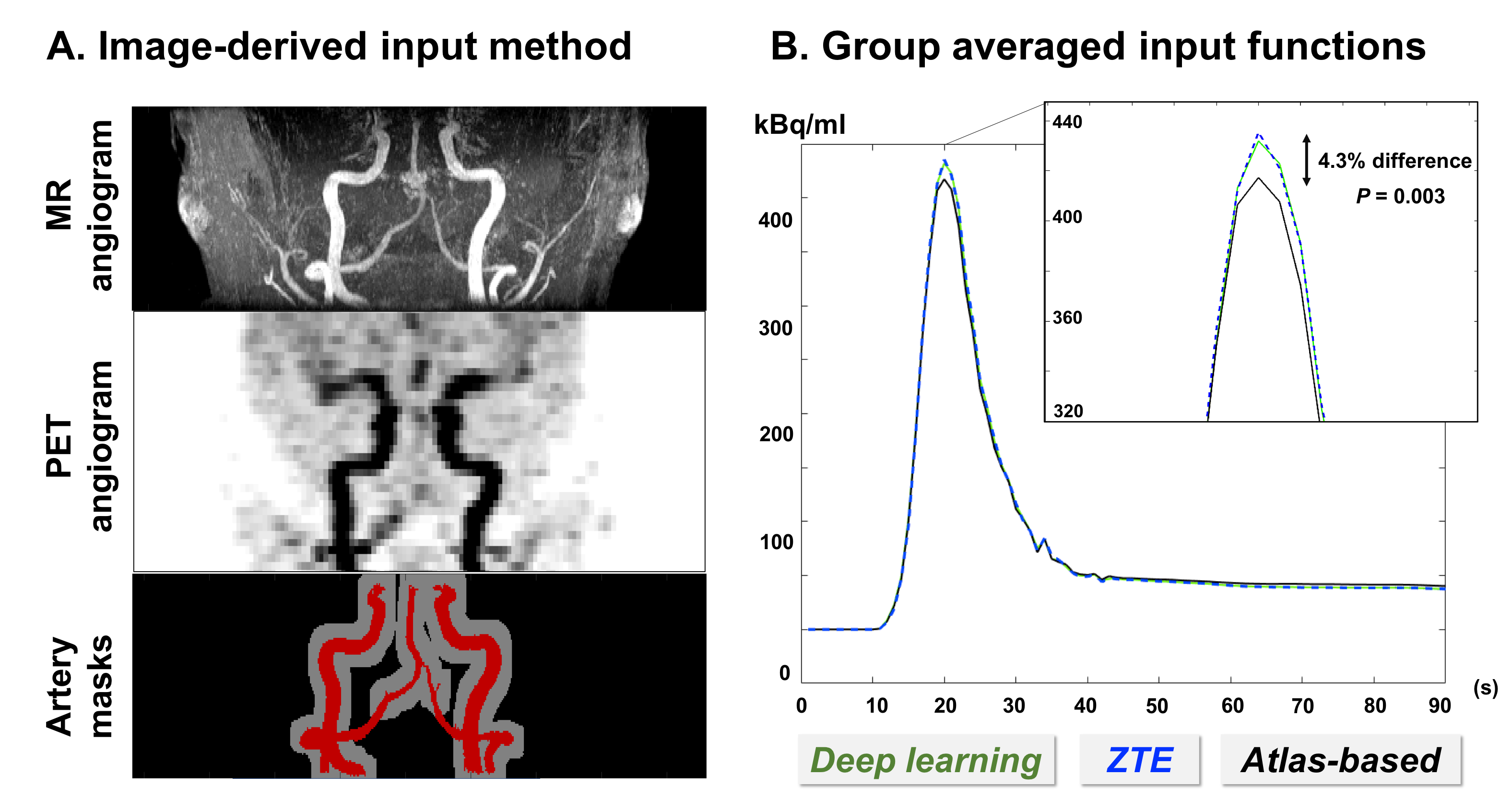
Figure 2. (a) Image-derived input functions (IDIFs) were generated from dynamic PET signal within cervical arteries and corrected based on high-resolution segmented artery volumes from MRI angiograms (red) and removing spill-in effect (gray)2. IDIFs were generated independently for deep-learning, ZTE-, and atlas-based attenuation correction (AC), using separate dynamic PET reconstructions for each AC type.
(b) Group averages of IDIFs from each AC type were generated by normalizing for radiotracer dose and performing temporal alignment to the injection time. Atlas-based IDIF underestimated the peak by 4.3% (P<0.003) on average, while ZTE-based IDIF was not different from deep-learning IDIF (our reference standard).
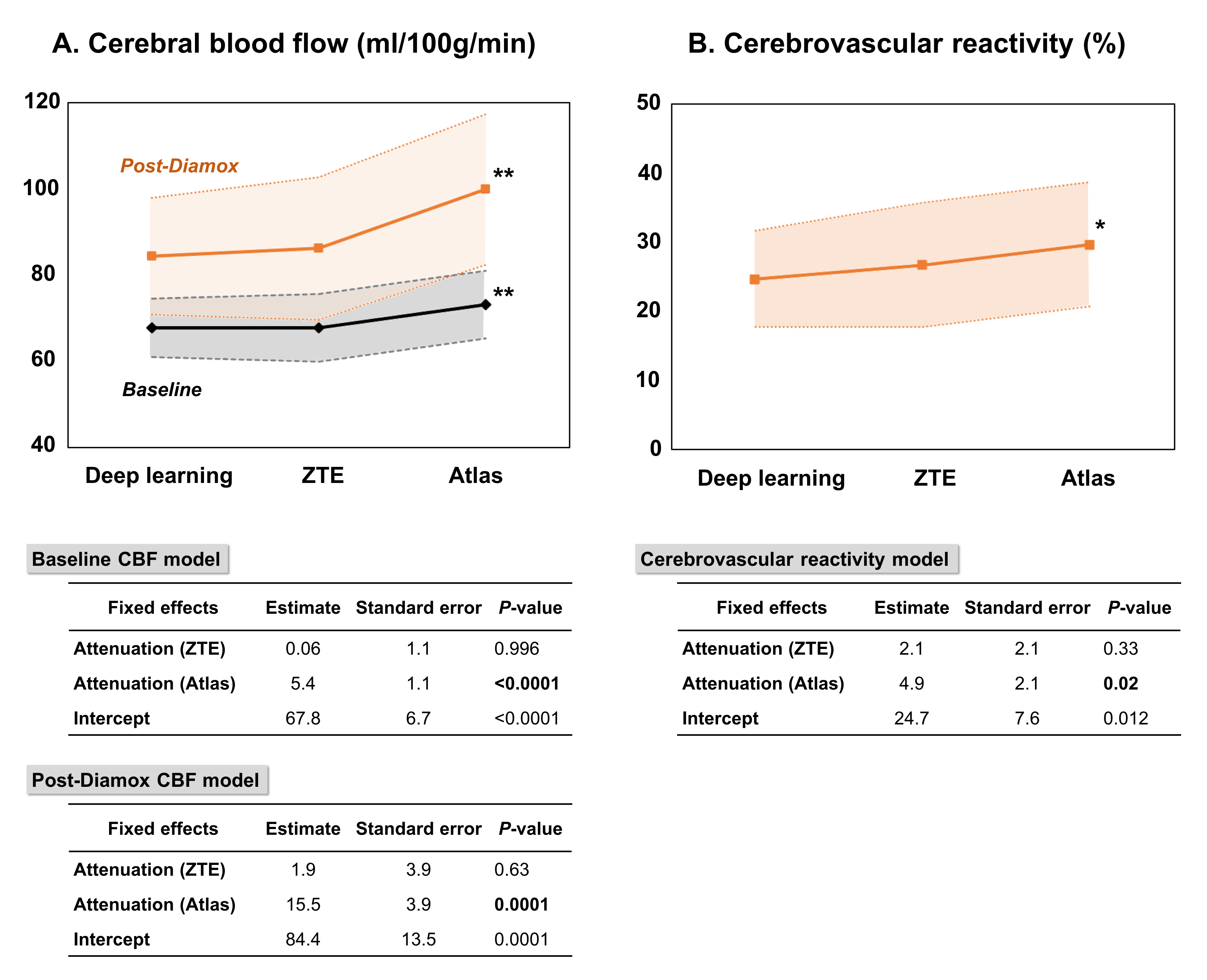
Figure 3. (a) Mixed effects regression evaluated the effect of attenuation correction type on cerebral blood flow (CBF) at baseline and after vasodilation with Diamox, while correcting for subject as a random effect. Graphs depict the model results and standard error, indicating that atlas-based AC overestimated CBF by 5.4 ml/100g/min (8.0%, P<0.0001) at baseline and overestimated CBF by 15.5 ml/100g/min (18.0%, P=0.0001) after Diamox. CBF values from ZTE-based AC were not different from the reference (deep learning AC).
(b) A similar mixed effects model showed that atlas-based AC also overestimated cerebrovascular reactivity (the % increase in CBF) by 19.8% (P=0.02).
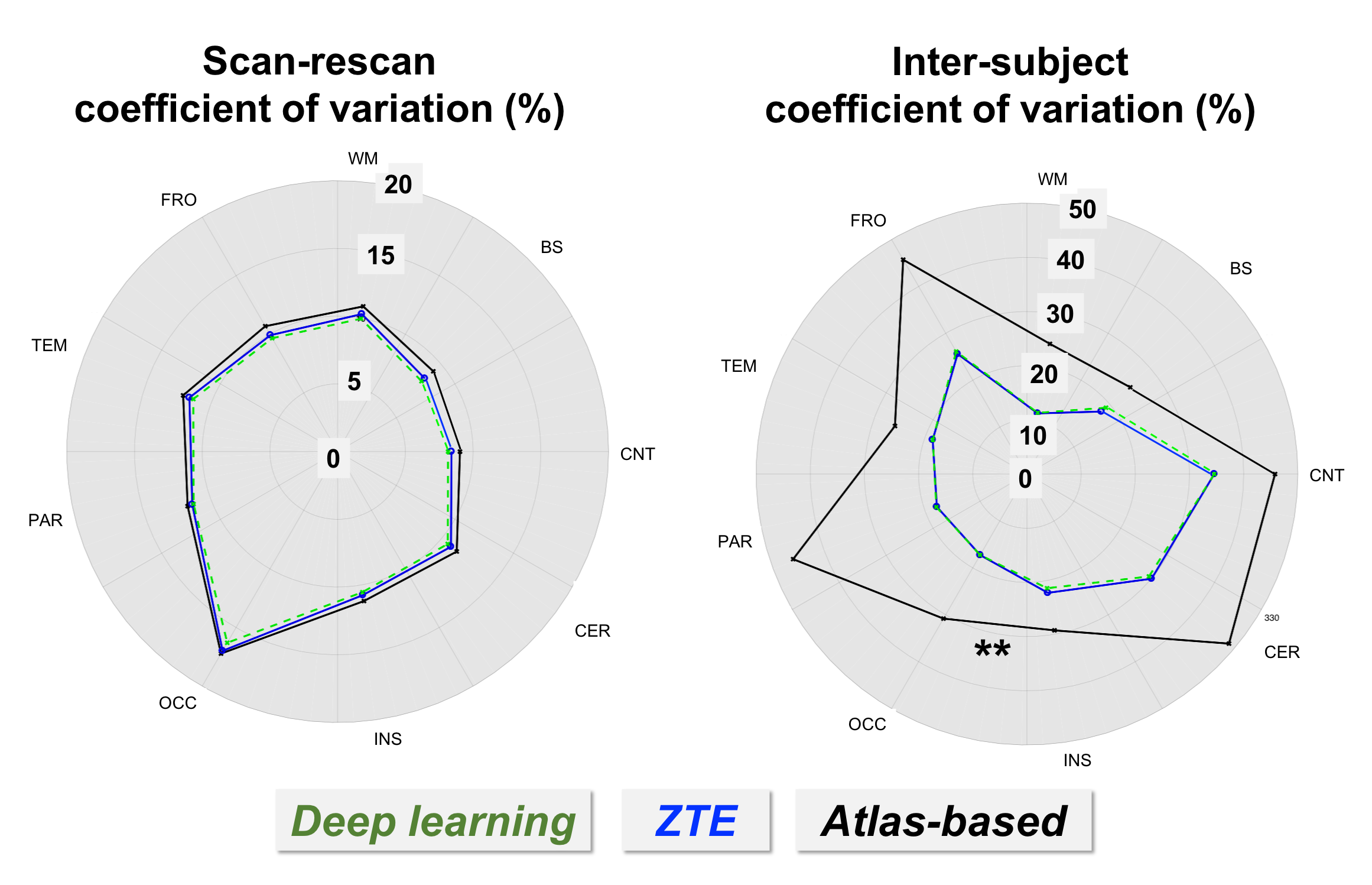
Figure 4. (a) Scan-rescan coefficient of variation (CoV, %) for cerebral blood flow (CBF) measurements at baseline. Scan-rescan CoV was calculated as the standard deviation of differences between the two scans, divided by the mean CBF across subjects. Each data point represents CoV for a region of interest. Scan-rescan reproducibility of CBF was not different across the attenuation correction methods (P=0.31).
(b) Inter-subject CoV was calculated as the standard deviation of CBF across volunteers, divided by the mean CBF. Inter-subject CoV was higher for atlas-based AC than for ZTE- or deep learning-based AC (P<0.0001).