0262
Fluorine MRI-Visible Mixed-Alginate Gradient Fluorocapsules for Image-Guided Diabetes Treatment1Radiology, The Johns Hopkins University School of Medicine, Baltimore, MD, United States, 2Pathology and Medical Biology, University of Groningen, Groningen, Netherlands, 3Oncology, The Johns Hopkins University School of Medicine, Baltimore, MD, United States, 4Biomedical Engineering, The Johns Hopkins University, Baltimore, MD, United States, 5Chemical and Biomolecular Engineering, The Johns Hopkins University, Baltimore, MD, United States
Synopsis
A promising treatment of auto-immune juvenile diabetes is transplantation of beta islet cells. Islets can be encapsulated inside semi-permeable microcapsules to protect them against the patients’ immune system. Low islet survival and the lack of means to monitor the implants are major issues. We employed mixed-alginate gradient (MAG) microcapsules that better support human islet viability compared to currently used microcapsules. By labeling the capsules with clinically used agent CS-1000, we created MAG fluorocapsules which appeared as hot spots in mice on 19F MRI. MAG fluorocapsules offer a drug-free means to treat diabetic patients long-term while enabling imaging of transplanted islets.
INTRODUCTION
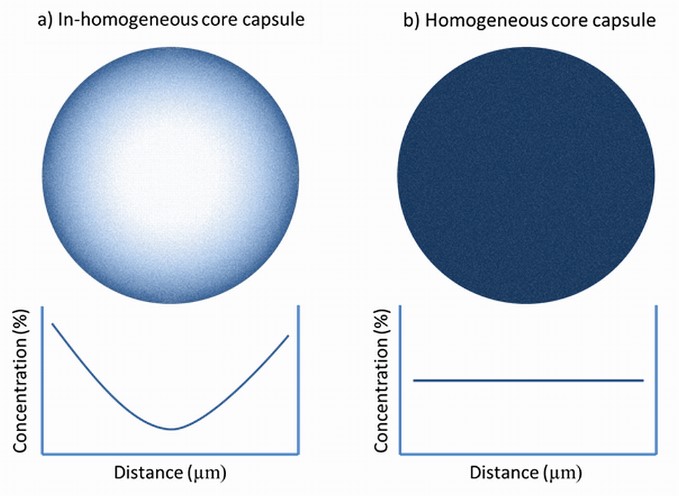
Replacement of the patient’s damaged beta islet cells by transplanted donor islets is a potential treatment to achieve long-term, moment-to-moment glucose regulation in type I juvenile diabetic patients. One strategy to avoid the use of toxic immunosuppressive drugs is to surround the islets with thin layers of porous gel, i.e. encapsulate them inside gel microcapsules. The pore sizes of the gel are engineered such that small molecules (nutrients, oxygen, glucose and insulin) can diffuse in and out of the microcapsules, while large entities (cells and proteins of the immune system) are physically blocked from approaching and destroying the islets inside the microcapsules. Despite promising preclinical studies, clinical trials of encapsulated islets have lacked long-term efficacy1-4. Persistent challenges include low or short-term islet survival in vivo and the lack of means to elucidate the fate of implants after transplantation. Unlike macro-sized scaffolds, microcapsules can be infused into the patients using a minimally-invasive surgery. However, the only currently available means to monitor transplanted encapsulated islets are assays of blood samples, such as the assay of c-peptide secreted by the islets. These assays can only report on the implants after the islets are dead or stop producing insulin when it is too late to apply interventional treatment. To address these issues, we employed the newest generation of immunoprotective microcapsules called mixed-alginate gradient (MAG) or in-homogeneous core capsules (Fig. 1a). MAG capsules have a liquid core5 and therefore may offer a higher diffusion rate of oxygen and nutrients inside the microcapsule compared to currently used homogeneous core capsule (Fig. 1b) that have a dense gel core. We embedded the 19F tracer CS-1000 into MAG microcapsules to create a novel type of microcapsules, called MAG fluorocapsules, that can be visualized by 19F MRI.
METHODS
MAG and homogenous core fluorocapsules were synthesized using a homemade electrostatic generator. We first encapsulated human islets inside MAG microcapsules and homogeneous core microcapsules without CS-1000 to investigate if MAG microcapsules can better support islets than their homogeneous core counterpart. The viability of islets was assayed using Propidium Iodide (dead cells) and Newport Green (live cells) staining. Varying amounts of CS-1000 were co-encapsulated in the microcapsules to optimize the MRI sensitivity, mechanical strength, and morphology of the fluorocapsules. To determine the number of encapsulated 19F atoms, MAG fluorocapsules were ruptured by 0.5 M EDTA at pH=8.0 and then measured by a 400 MHz Varian NMR. MAG fluorocapsules (without islets) were transplanted IP (300 fluorocapsules) or SC (50 fluorocapsules) to C57BL/6 mice. MRI of mice was performed at 17.6T by a vertical Bruker scanner using a dual-tunable 19F/1H birdcage resonator. A capillary tube containing undiluted CS-1000 was placed on the mouse as a reference. A RARE sequence was used for 1H and 19F MRI of IP and SC implants. The following parameters were used for 1H MRI of IP implants: TR/TE = 1000/31 ms, FOV = 2.28 X 2.29 cm, matrix = 128 x 64, slice thickness = 2 mm, 8 signal averages. 19F MRI of IP implant: TR/TE = 1000/5.8 ms, 512 signal averages and the same geometry with 1H scan. 1H MRI of SC implant: TR/TE = 2267/32 ms, FOV = 2.78 X 2.59 cm, matrix = 32 X 32, slice thickness = 2 mm, 64 signal averages. 19F MRI of SC implant: TR/TE = 1000/5.8 ms, 512 signal averages and the same geometry with 1H scan.RESULTS
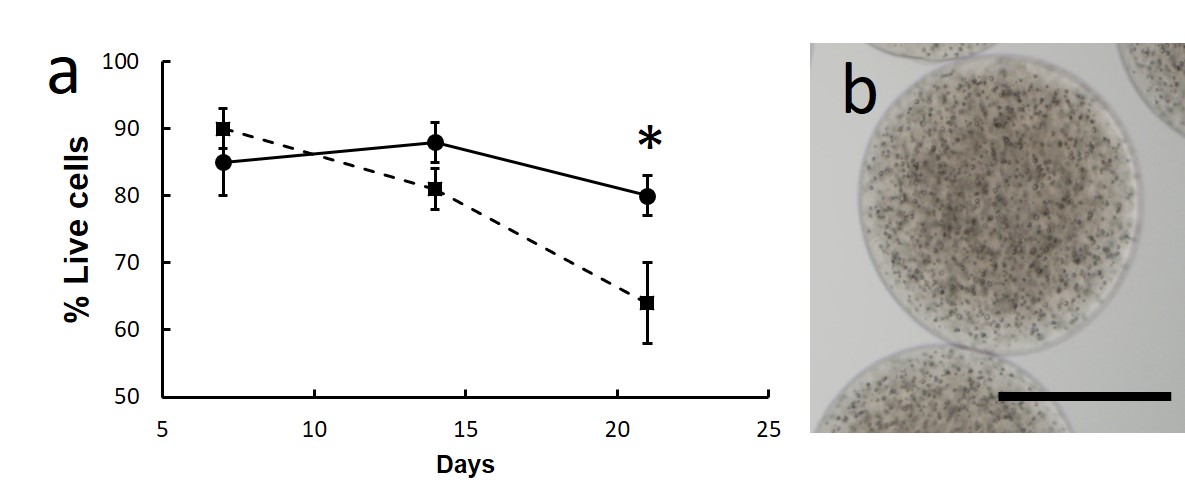
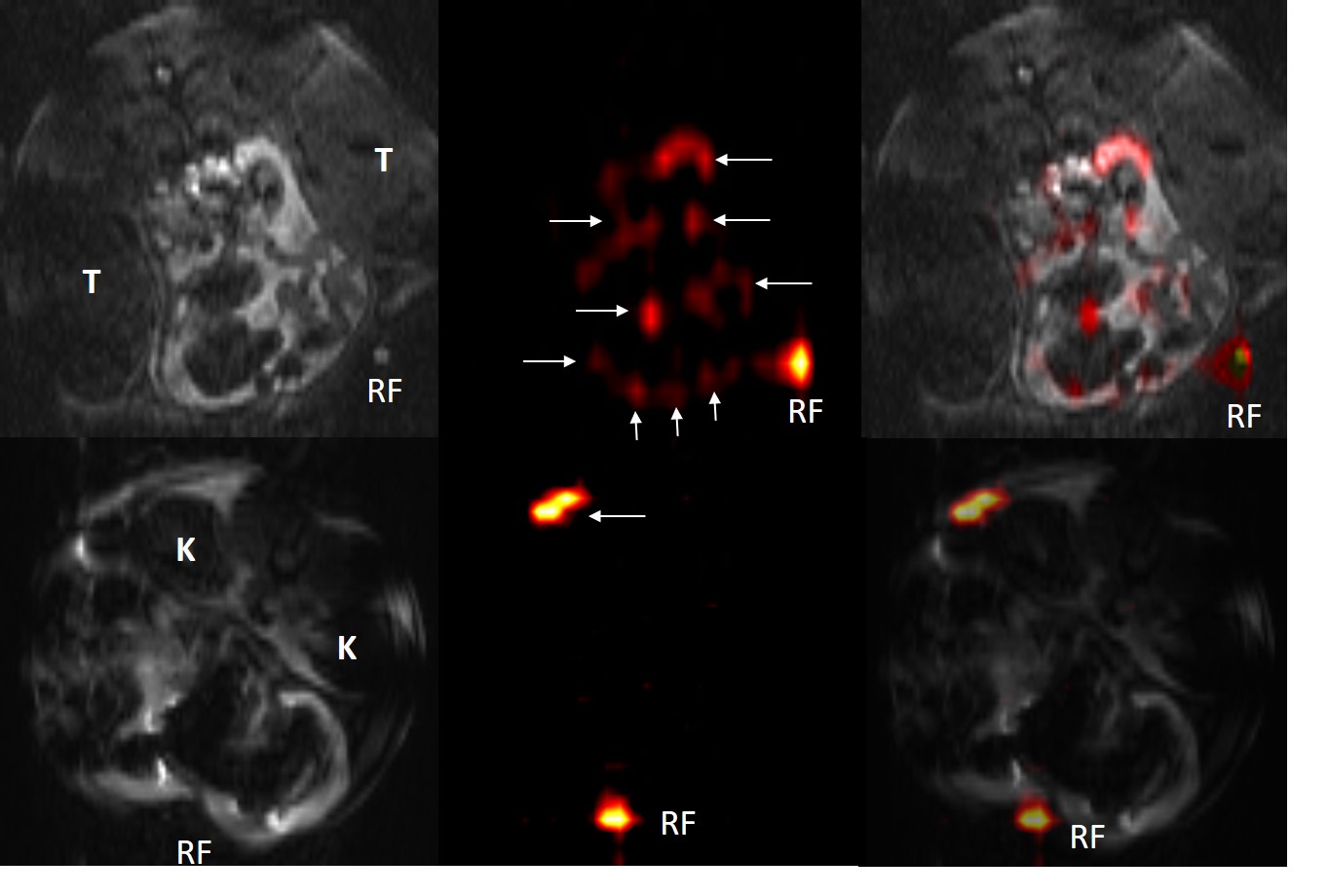
The viability of encapsulated human islets inside MAG microcapsules (without CS-1000) was ~25% higher than that of islets inside homogeneous core capsules (Fig. 2a). We have successfully synthesized MAG fluorocapsules (Fig. 2b), containing 4-6 X 1016 19F atoms per fluorocapsule, which appeared as hot spots on 19F MRI when IP or SC transplanted to mice (Fig. 3).DISCUSSION
MAG microcapsules are superior compared to homogeneous core microcapsules in supporting the viability of human islets in vitro. In addition, 19F MRI capability of MAG fluorocapsules may enable physicians to visually confirm implantation at the correct target site and to non-invasively monitor the dispersion of fluorocapsules after surgery without the complication of background artifacts as typically encountered in 1H MRI.CONCLUSION
MAG fluorocapsules potentially offer a drug-free means to replace damaged islets in diabetic patients while enabling image-guided transplantation and non-invasive follow-ups after transplantation.Acknowledgements
This work was supported by grant number R01 DK106972 from the National Institute of Diabetes and Digestive and Kidney Diseases at the National Institutes of Health.References
1. Vaithilingam, V., S. Bal, and B.E. Tuch, Encapsulated Islet Transplantation: Where Do We Stand? Rev Diabet Stud, 2017. 14(1): p. 51-78.
2. Strand, B.L., A.E. Coron, and G. Skjak-Braek, Current and Future Perspectives on Alginate Encapsulated Pancreatic Islet. Stem Cells Transl Med, 2017. 6(4): p. 1053-1058.
3. Barkai, U., A. Rotem, and P. de Vos, Survival of encapsulated islets: More than a membrane story. World J Transplant, 2016. 6(1): p. 69-90.
4. Desai, T. and L.D. Shea, Advances in islet encapsulation technologies. Nat Rev Drug Discov, 2017. 16(5): p. 367.
5. Morch, Y.A., et al., Effect of Ca2+, Ba2+, and Sr2+ on alginate microbeads. Biomacromolecules, 2006. 7(5): p. 1471-80.
Figures