0261
Fluorine-19 MR at 21.1 Tesla for Enhanced Detection of Brain InflammationSonia Waiczies1, Jens Rosenberg2, Paula Ramos Delgado1, Ludger Starke1, Joao dos Santos Periquito 1, Christian Prinz1, Jason M. Millward1, Andre Kuehne3, Helmar Waiczies3, Andreas Pohlmann1, and Thoralf Niendorf1
1Max Delbrueck Center for Molecular Medicine in the Helmholtz Association, Berlin, Germany, 2The National High Magnetic Field Laboratory, Florida State University, Tallahassee, FL, United States, 3MRI TOOLs GmbH, Berlin, Germany
Synopsis
Fluorine-19 (19F) MR methods are invaluable for several applications including detection of brain inflammation but suffer from inherently low signal-to noise ratio (SNR). A magnetic field increase from 9.4 to 21.1 Tesla was studied as strategy for increasing signal sensitivity. As a result of an SNR increase, inflammation regions undetected at 9.4T were revealed at 21.1T. Although the SNR gain at 21.1T does not reach that achieved with a cryogenic quadrature RF surface probe (19F-CRP) at 9.4T, increased sensitivity was observed throughout the whole field of view at 21.1T, from ventral to dorsal head regions.
Introduction
Fluorine-19 (19F) Magnetic Resonance (MR) methods have been applied in a multitude of biomedical research applications, including detection of inflammatory cells in vivo using 19F nanoparticles1-6. Although the absence of background signal is an advantage, the low abundance of 19F nuclei in vivo poses a major sensitivity challenge for MR detection. We reported on sensitivity gains achieved using a cryogenic quadrature RF probe (19F-CRP)7. Another way to improve signal sensitivity is to increase the strength of the static magnetic field (B0)8, a strategy actively pursued for clinical application9. Here we studied sensitivity gains when moving from 9.4 to 21.1T to leverage for enhanced detection of brain inflammation in experimental autoimmune encephalomyelitis (EAE).Methods
Experiments were carried out on 9.4T and 21.1T small animal MR systems. Two volume coils and the 19F-CRP were used at 9.4T (1H: f=400 MHz, 19F: f=376 MHz) and one volume coil at 21.1T (1H: f=900 MHz, 19F: f=844.9 MHz). SNR was measured on perfluoro-15-crown-5-ether (PFCE) using 2D-FLASH (TE=4.2ms, TR=14-5000ms, FA=5°-90°, FOV=[32×32]mm2, matrix=256×256, NA=6, TA=0.5–43min). Using MATLAB® (Mathworks, Natick, USA), SNR was calculated by dividing magnitude image signal (Sm) by background standard deviation (σm), compensating for non-Gaussian distribution10. Animal experiments were carried out in accordance with local animal welfare guidelines: EAE was induced in SJL/J mice, PFCE NPs administered daily for five days, and tissue prepared for ex vivo MRI7. 3D-RARE brain 19F MRI: TR=800ms, TE=4.9ms, FOV=30×20×20mm, NEX=256, matrix=90×60×60, ETL=15, TA=3h24m46s. FLASH brain 1H MRI: TR=150ms, TE=7.5ms, FOV=30×20×20mm, matrix=600×400×400, NEX=2, TA=3h20m.Results
When studying SNR changes over the relaxation period for PFCE, T1 for PFCE decreased with increasing B0: T1|9.4T=778ms (Fig.1A) and T1|21.1T=409ms (Fig.1B). SNReff was highest at TR=20ms and FA=13° at 9.4T: SNReff =96/SQRTmin (Fig.1C) and TR=20ms and FA=18° at 21.1T: SNReff=701/SQRTmin (Fig.1D). At TR=20ms and FA=13°, SNReff=668/SQRTmin for 21.1T. Thus the gain in SNReff for 21.1T compared to 9.4T is 7-7.3, depending on the conditions used. Since higher B0 resulted in lower T1 values, we distinguished between B0 and T1 influencing factors by comparing SNReff at 9.4T (Fig.2A) with SNReff at 21.1T modelled for T1|9.4T=778 ms (Fig.2B). The B0 effect on SNReff gain was 5.3 (SNReff max|21.1T=505/SQRTmin and SNReff max|9.4T=96/SQRTmin) while the T1 shortening effect was 1.3. Both factors result in the SNReff profile shown in Fig.2D for 21.1T. We recently reported on the advantages of using a 19F-CRP7. Here we studied the sensitivity gain achieved with the 19F-CRP compared to a RT coil, both at 9.4T, using the same MR acquisition methods and 19F sample as above. We used two NMR tubes in order to study the SNR gain at regions distal and proximal to the 19F-CRP surface (Fig.3). From the 3D-fit obtained for both RT coil (Fig.3A,C) and 19F-CRP (Fig.3B,D), the highest SNReff values calculated for the RT coil were 268/SQRTmin (upper-ROI) and 278/SQRTmin (lower-ROI) and for the 19F CRP these were 2762/SQRTmin (upper-ROI, closest to surface) and 652/SQRTmin (lower-ROI, furthest from surface). Thus the gain in SNReff for the 19F CRP compared to the RT coil is 10.3 for the upper ROI and 1.4 for the lower ROI. 19F MRI at 21.1T revealed greater detection of inflammation in brain and lymph nodes (Fig.4A) and decreased T1 values in spleen (Fig.4B) of EAE mice when compared to 9.4T.Discussion
An increase in B0 resulted in increased SNR efficiency, partially due to a T1 effect but mainly due to the B0 effect, as expected11-13. As a result of the SNR increase, inflammatory regions in brain and lymph nodes not detected at 9.4T were revealed at 21.1T. Although the SNR gain at 21.1T is not as high as that achieved with the 19F-CRP, increased sensitivity is expected throughout the whole field of view, given the uniform spatial signal distribution of the volume resonators used. This is not the case for the 19F-CRP (Fig.3B vs. 3D), which as a transceive surface RF coil does not achieve a spatially-uniform excitation7.Acknowledgements
This work was supported by the State of Florida (NSF Cooperative Agreement DMR-1644779), the NHMFL User Collaborations Grant Program travel funding and the Deutsche Forschungsgemeinschaft (DFG WA2804, DFG PO1869).References
- Flögel, U., et al. In vivo monitoring of inflammation after cardiac and cerebral ischemia by fluorine magnetic resonance imaging. Circulation 118, 140-148 (2008).
- Ahrens, E.T., Young, W.B., Xu, H. & Pusateri, L.K. Rapid quantification of inflammation in tissue samples using perfluorocarbon emulsion and fluorine-19 nuclear magnetic resonance. Biotechniques 50, 229-234 (2011).
- Flogel, U., et al. Selective activation of adenosine A2A receptors on immune cells by a CD73-dependent prodrug suppresses joint inflammation in experimental rheumatoid arthritis. Sci Transl Med 4, 146ra108 (2012).
- Ahrens, E.T. & Zhong, J. In vivo MRI cell tracking using perfluorocarbon probes and fluorine-19 detection. NMR Biomed 26, 860-871 (2013).
- Waiczies, H., et al. Visualizing brain inflammation with a shingled-leg radio-frequency head probe for 19F/1H MRI. Scientific reports 3, 1280 (2013).
- Jacoby, C., et al. Probing different perfluorocarbons for in vivo inflammation imaging by 19F MRI: image reconstruction, biological half-lives and sensitivity. NMR Biomed 27, 261-271 (2014).
- Waiczies, S., et al. Enhanced Fluorine-19 MRI Sensitivity using a Cryogenic Radiofrequency Probe: Technical Developments and Ex Vivo Demonstration in a Mouse Model of Neuroinflammation. Scientific reports 7, 9808 (2017). Ladd, M.E. The quest for higher sensitivity in MRI through higher magnetic fields. Zeitschrift für Medizinische Physik 28, 1-3 (2018).
- Niendorf, T., Barth, M., Kober, F. & Trattnig, S. From ultrahigh to extreme field magnetic resonance: where physics, biology and medicine meet. Magnetic Resonance Materials in Physics, Biology and Medicine 29, 309-311 (2016).
- NEMA. Determination of signal-to-noise ratio (SNR) in diagnostic magnetic resonance imaging. National Electrical Manufacturers Association Standards Publication MS, 1-2008 (2008).
- Hoult, D.I. & Richards, R.E. The signal-to-noise ratio of the nuclear magnetic resonance experiment. J.Magn Reson.(1969) 24, 71-85 (1976). Hoult, D.I. & Lauterbur, P.C. Sensitivity of the Zeugmatographic Experiment Involving Human Samples. Journal of Magnetic Resonance 34, 425-433 (1979).
- Pohmann, R., Speck, O. & Scheffler, K. Signal-to-noise ratio and MR tissue parameters in human brain imaging at 3, 7, and 9.4 tesla using current receive coil arrays. Magnetic Resonance in Medicine 75, 801-809 (2016).
Figures
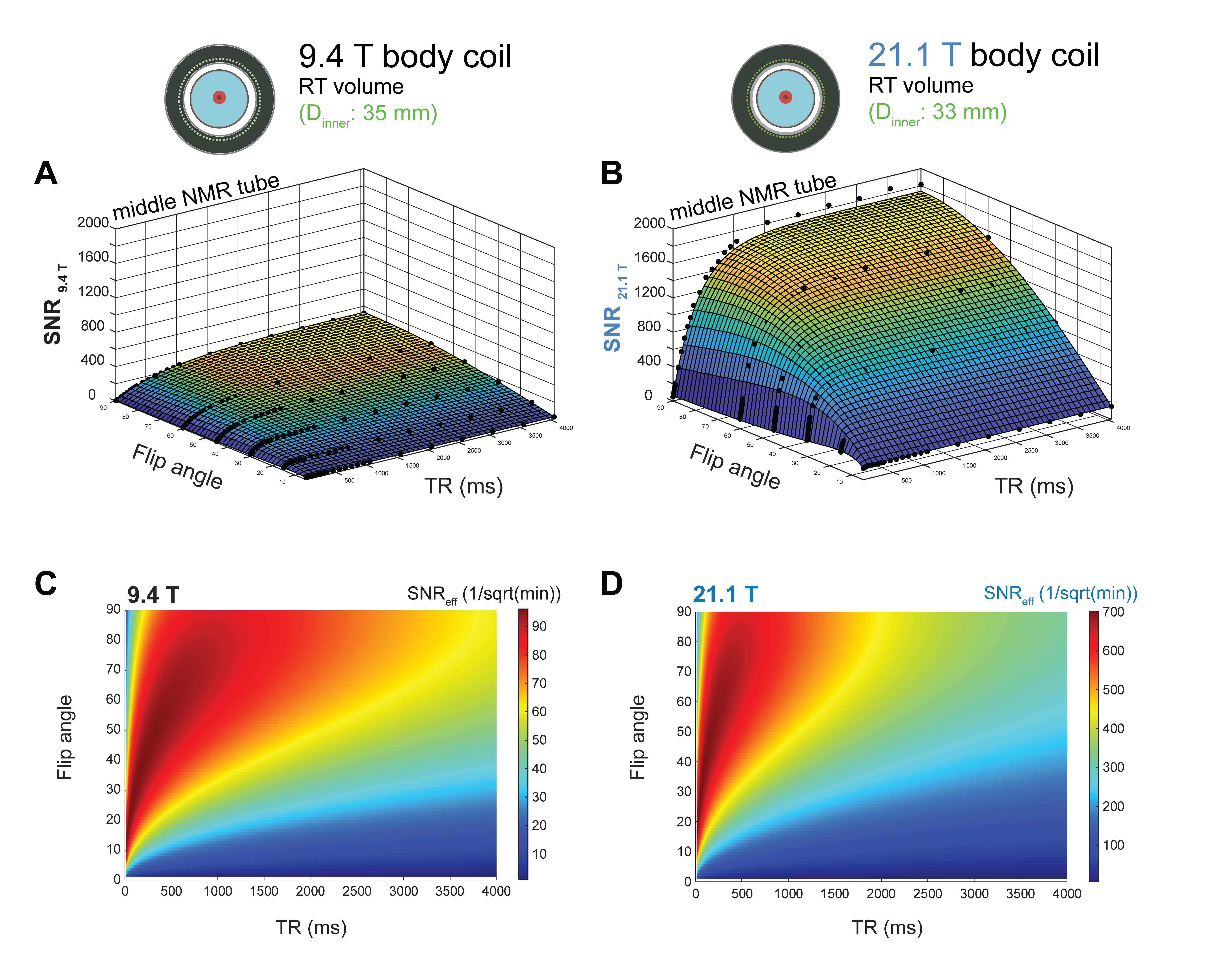
Figure 1. Comparison of SNR between 9.4 and 21.1 Tesla for PFCE using 2D-FLASH. Upper panel, left: 19F/1H RF coil at 9.4T (32 legs, widthleg=1mm,
lengthleg=33mm lengthcoil=39mm, Øinner=18.4mm, Øshield=58mm), right: 19F/1H RF coil at 21.1T (8 rungs, lengthcoil=54.5mm,
Øinner=33mm), holding one NMR tube within a 15-ml
tube. SNR measurements at TR=14ms-4000ms and FA=5°-90°
for both 9.4 Tesla (A) and 21.1 Tesla (B). 2-D data fitting resulted in T1|9.4T=778
ms and T1|21.1T=409 ms. SNR efficiency (SNReff) was calculated for all values at 9.4T (C) and
21.1T (D). SNReff is the
SNR achievable in a fixed amount of time and was calculated by dividing SNR by
SQRT(NA×TR).

Figure 2. SNR
efficiency changes between 21.1T and 9.4T B0 strengths for PFCE as a
result of B0 and T1 effects. The B0
factor on SNR efficiency at 21.1T was calculated to be 5.25 after modelling
SNR/SQRTt to keep T1 between both magnetic fields constant (T1|21.1T
= T1|9.4T = 788 ms). The T1 factor on SNR efficiency at
21.1T was calculated to be 1.3.

Figure 3. Comparison of SNR between RT 19F RF coil versus the 19F-CRP, both operated at 9.4T using same sample and sequence as above. Upper panel, left: linear 19F/1H RT RF coil for 9.4 Tesla (32 legs, widthleg=1mm, lengthleg=33mm, lengthcoil=39mm, Øinner=18.4mm, Øshield=58mm), right: quadrature transceive 19F cryogenic quadrature RF surface probe for 9.4 Tesla (2 coil elements: [f×z]:[16×20]mm2, total [27×20]mm2), both coils hold two NMR tubes. SNR measurements at TR=14ms-5000ms and FA=5°-90° were calculated for upper NMR tube for RT head coil (A) and 19F-CRP (B) and for lower NMR tube for RT head coil (C) and 19F-CRP (D).

Figure 4. Comparing regions of inflammation at different field strengths in an ex vivo EAE mouse brain and lymphatic organs. Upper panel, left: linear 19F/1H RF coil for 9.4 Tesla, right: linear 19F/1H birdcage RF coil for 21.1 Tesla, both with an ex vivo mouse sample in 15-ml tube. 19F and 1H MR images were acquired at (A) 9.4T and (B) 21.1T using 3D-RARE for 19F MRI (methods). 19F T1maps for PFCE in spleen were acquired at (C) 9.4T and (D) 21.1T using RARE-VTR: 9TRs=50-12000ms, TE=6.9 ms, ETL=4, FOV=[20×30]mm2, matrix=44×64, slice-thickness=3.6 mm, NA=128, TA=15h50m.