0251
Quantitative Susceptibility Mapping: In Vivo Biomarkers for Cerebral Cavernous Malformations Related Epilepsy1Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 2China National Clinical Research Center for Neurological Diseases, Beijing, China, 3Department of Neurosurgery, Peking University International Hospital, Beijing, China, 4Department of Neuroradiology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 5GE Healthcare, China, Beijing, China
Synopsis
Hemosiderin deposits surrounding the cerebral cavernous malformations (CCMs) had been proposed to be associated with the pathogenesis of CCM-related epilepsy (CRE). An increased perilesional and extralesional iron deposition were found in CCMs with epilepsy through susceptibility maps of quantitative susceptibility mapping (QSM). To investigate novel biomarkers for the in vivo and longitudinal evaluation of CCM lesions with epilepsy, this study was to explore the iron quantity in CCMs patients with CRE using quantitative susceptibility mapping.
Introduction
Patients with cerebral cavernous malformation (CCM) -related epilepsy (CRE) could not always achieve seizure freedom after surgical resection of the lesion, suggesting an inadequate treatment of the epileptogenic zone. Iron deposition within cerebral cavernous malformations had been postulated to play an important role in CRE. To demonstrate the relationship between hemosiderin deposits surrounding the CCMs with the pathogenesis of CRE, quantitative susceptibility mapping (QSM), considered to be the suitable imaging technique to in vivo detection of brain iron deposition, was employed to analyze the iron quantity in CCM patients with epilepsy.Methods
Twenty-five patients harboring supratentorial CCM without surgery or radiation were identified in 38 patients with CCMs undergoing QSM between September 2017 and July 2018 in our institution. Imaging was conducted on a 3T MR system (GE Healthcare) with an 8-channel head coil. Parameters of QSM gradient echo images: TR/16TEs = 41.6/3.2 - 45.00 ms, voxel = 0.9 × 0.9 × 2.0 mm3, Max slices = 926, no gaps, average = 1, flip angle = 12°, bandwidth = 62.50 Hz/pixel, FOV = 320 × 320 mm2, matrix = 256 × 256, acquisition time = 7 min, 59 sec. The magnetic susceptibility measurements were performed on the susceptibility map co-registered with structural images. The regions of interest (ROIs) were manually drawn on CCM leison, perilesional T2 hypointensity rim, and extralesional brain with increased susceptibility (>0.10 ppm, parts per million) on QSM (Fig.1). The distance between perilesional T2 hypointensity rim and margin of extralesional brain with increased susceptibility was measured in each slice of lesions (Fig.1). The mean susceptibility of CCM leison, perilesional T2 hypointensity rim, and extralesional brain with increased susceptibility and mean distance of different slices of lesions were further compared among patients with or without CRE by t test and two-way ANOVA.Results
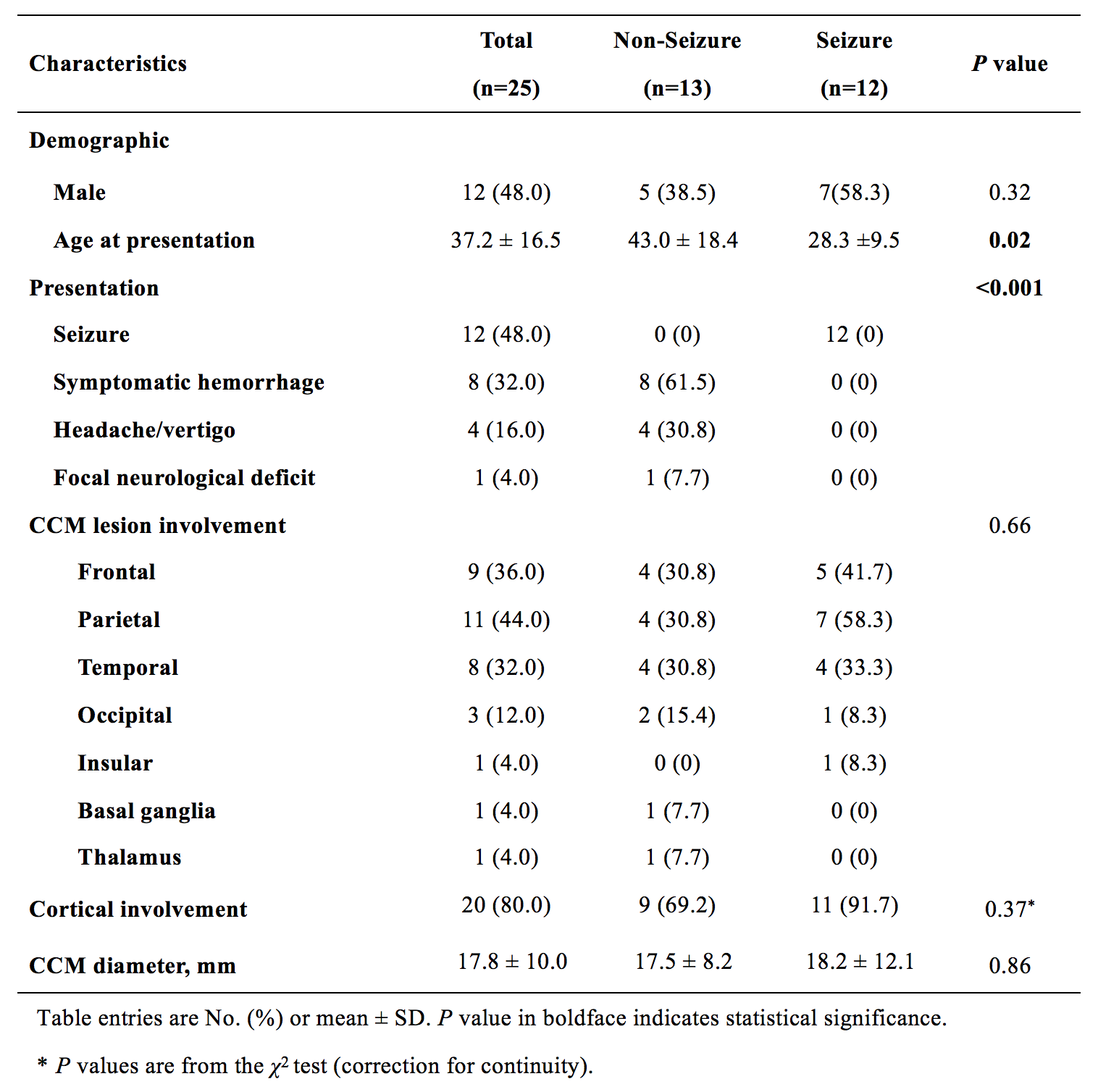
CRE was observed in thirteen patients (48.0%, 12/25) (Table 1). The CCM lesions with epilepsy exhibited higher mean susceptibility in perilesional T2 hypointensity rim (0.64±0.14 ppm) than those without (0.45±0.14 ppm, P=0.003) (Fig.2B). An extralesional brain area surrounding CCM lesions exhibited increased mean susceptibility, compared with remote cortex (seizure group: 0.34±0.14 ppm versus 0.05±0.006 ppm, P<0.0001; non-seizure group: 0.27±0.04 ppm versus 0.05±0.006 ppm, P<0.0001) (Fig. 2D). The distance between T2 hypointensity rim and extralesional brain with increased susceptibility was significantly longer in patients with CCM related-epilepsy (4.17 ± 0.37 mm versus 2.55 ± 0.35mm, P=0.01) (Fig.2C). And there was a trend toward higher susceptibility within this abnormal extralesional brain area in patients with epilepsy (0.34±0.14 ppm versus 0.27±0.04 ppm, P=0.13).Discussion
Patients with CCM-related epilepsy (CRE) who undergo surgical resection achieve postoperative seizure freedom in only about 70% of cases1,2. This is frequently due to insufficient efforts made to adequately define and resect the epileptogenic zone4. Although hemosiderin deposits surrounding the CCM has been proposed to be involved in the pathogenesis of CRE, there was scarce evidence supporting a correlation between the presence or size of the hemosiderin rim and epilepsy3. QSM has been shown to provide reliable information on CCM related to lesional iron deposition5. Our preliminary data of QSM in CCM suggested a generally increased iron deposition surrounding CCM lesions with or without epilepsy. However, a higher QSM of hemosiderin rim and longer diameter of the extralesional iron deposition were observed in CRE, suggesting that the quantity and area of hemosiderin deposits were more likely to be associated with CRE, rather than the presence of hemosiderin rim. In addition, our study might provide evidence for extended resection in patients with CRE. Currently, the extension of excision including the surrounding gliosis and hemosiderin fringe remains subject to controversy regarding the outcome of seizure control, and the intraoperative resection extent of hemosiderin rim was usually based on a subject judgment or image guide under routine structural MRI. Our data suggested that future studies of QSM might be promising to develop intraoperative tools for surgical resection or perioperative biomarkers for CRE control. Admittedly, it was not feasible to illuminate the specific QSM features of CCM with distinct epilepsy duration and lobar location, with the present sample size. Therefore, further analysis in larger study population would individualize our current findings.Conclusions
QSM revealed increased perilesional and extralesional iron deposition in CCMs with epilepsy. These novel biomarkers might improve the in vivo and longitudinal evaluation of CCM lesions with epilepsy.Acknowledgements
This study was supported by grants to Dr. Li Ma from National Natural Science Foundation of China (H0906 81801140).References
1. Dammann P, Wrede K, Jabbarli R, Neuschulte S, Menzler K, Zhu Y, et al: Outcome after conservative management or surgical treatment for new-onset epilepsy in cerebral cavernous malformation. J Neurosurg 126:1303-1311, 2017.2. Englot DJ, Han SJ, Lawton MT, Chang EF: Predictors of seizure freedom in the surgical treatment of supratentorial cavernous malformations. J Neurosurg 115:1169-1174, 2011.
3. Menzler K, Chen X, Thiel P, Iwinska-Zelder J, Miller D, Reuss A, et al: Epileptogenicity of cavernomas depends on (archi-) cortical localization. Neurosurgery 67:918-924, 2010.
4. Rosenow F, Alonso-Vanegas MA, Baumgartner C, Blumcke I, Carreno M, Gizewski ER, et al: Cavernoma-related epilepsy: review and recommendations for management--report of the Surgical Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia 54:2025-2035, 2013.
5. Tan H, Liu T, Wu Y, Thacker J, Shenkar R, Mikati AG, et al: Evaluation of iron content in human cerebral cavernous malformation using quantitative susceptibility mapping. Invest Radiol 49:498-504, 2014
Figures
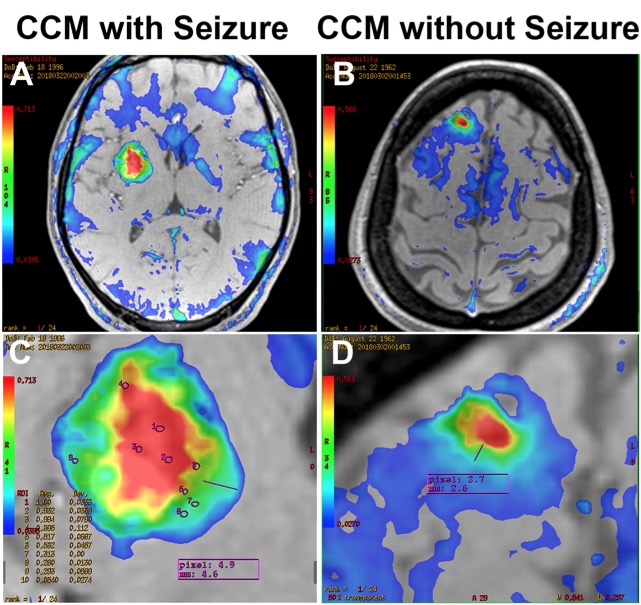
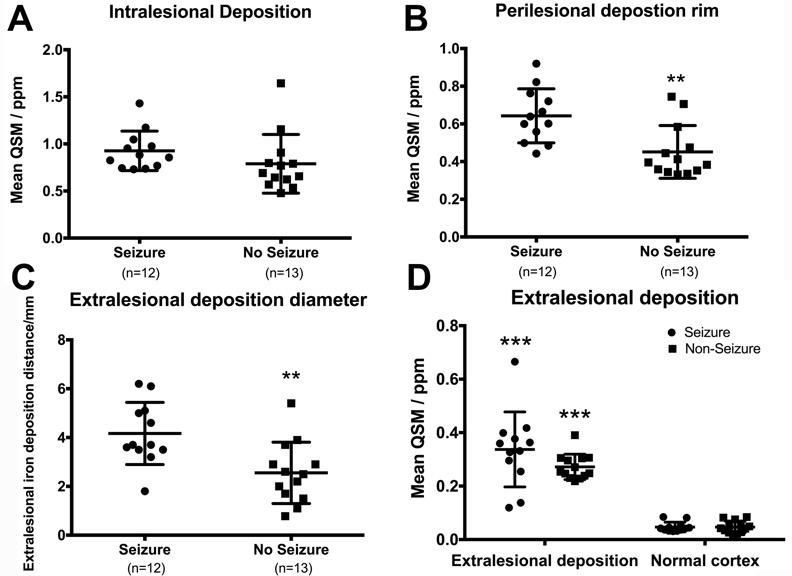
Figure.2 Comparision of magnetic susceptibility of A. CCM lesion, B. perilesional
T2 hypointensity rim, and C. the distance between
T2 hypointensity rim and extralesional brain with increased susceptibility
between CCM with and without epilepsy and comparision of D. extralesional
deposition between CCM and remote
cortex.
(**, <0.01, ***, <0.001).