0249
The UK7T Network’s Harmonized Neuroimaging Protocols1Wellcome Centre for Integrative Neuroimaging, FMRIB, NDCN, University of Oxford, Oxford, United Kingdom, 2Sir Peter Mansfield Imaging Centre, School of Physics and Astronomy, University of Nottingham, Nottingham, United Kingdom, 3Cardiff University Brain Research Imaging Centre, School of Psychology, Cardiff University, Cardiff, United Kingdom, 4Wolfson Brain Imaging Centre, Department of Clinical Neurosciences, University of Cambridge, Cambridge, United Kingdom, 5Imaging Centre of Excellence, University of Glasgow, Glasgow, United Kingdom
Synopsis
The UK7T Network is a consortium of 7-tesla-MRI capable sites in the United Kingdom, operating with three different scanner models, manufactured by two MR vendors. The Network has established a harmonized set of anatomical and functional MRI protocols for standardized neuroimaging across currently available human 7T scanners.
Here we make these harmonized protocols available to the community, along with example data, and describe the need for manual calibration to achieve harmonization across sites.
Introduction
The UK7T Network is a consortium of 7-tesla-MRI sites in the United Kingdom. The Network has established a harmonized set MRI protocols for standardized neuroimaging across sites.
The five Network sites use three different scanner models, manufactured by two vendors. Default protocols, sequence structure, image reconstruction and scanner adjustments consequently initially varied. An initial study was conducted to identify these differences and subsequently to test harmonized protocols.1
Here we make these harmonized protocols available to the community, along with example data. The Network’s optimized set of protocols are now being validated in a “travelling heads” study.2
Methods
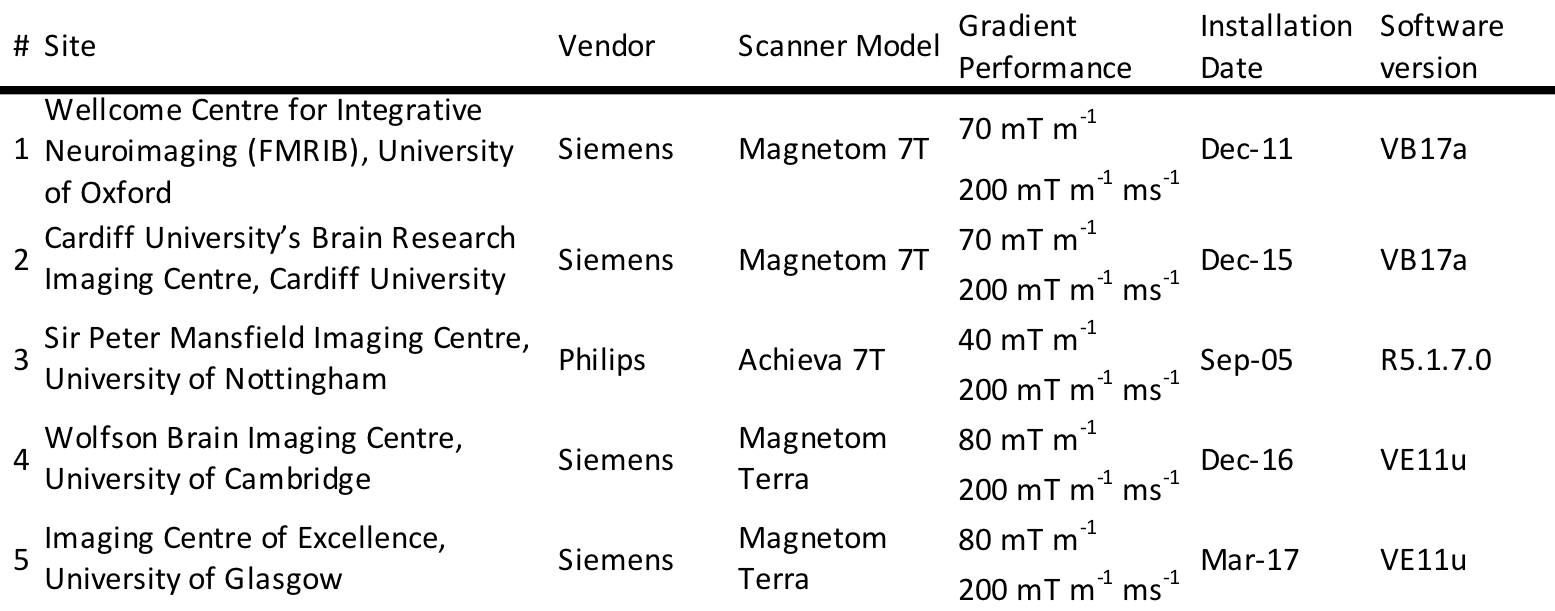
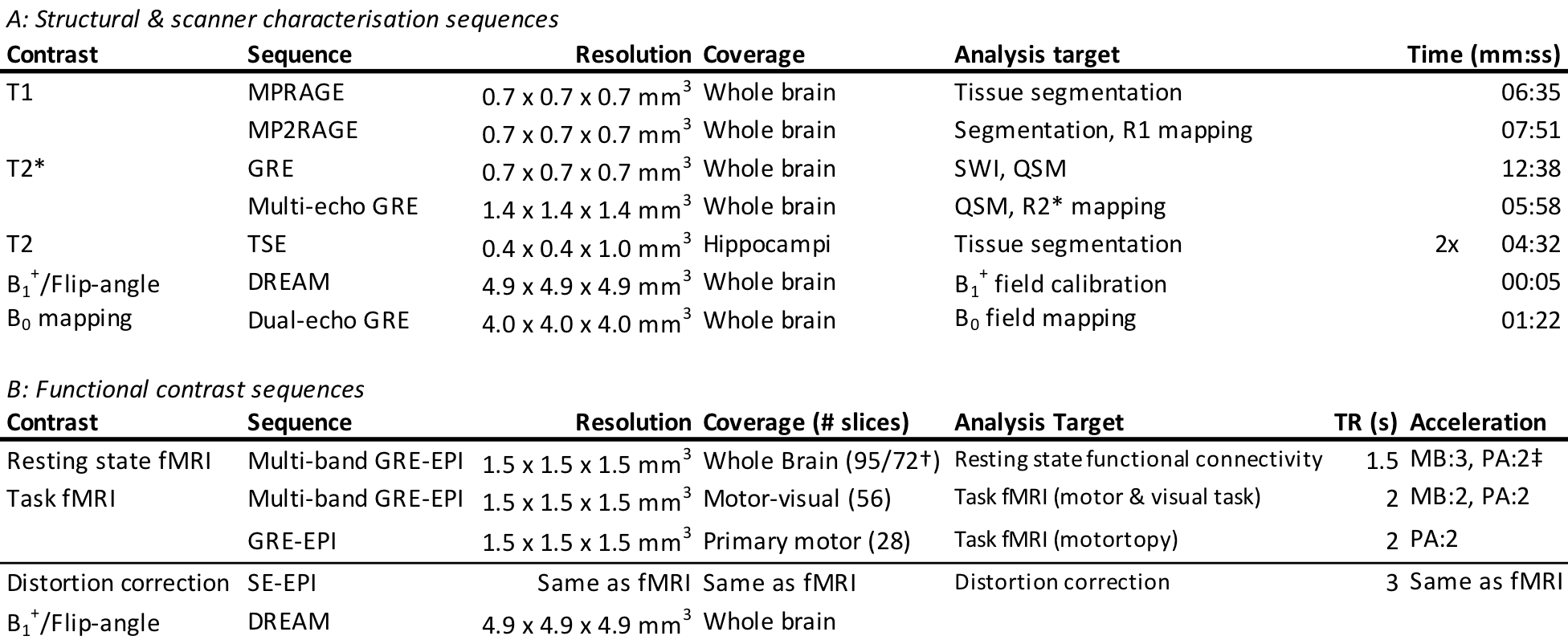
Protocols were harmonized across five UK-based 7T scanners. The hardware specification is given in Table 1. Harmonization was focussed on well-established structural and functional neuroimaging sequences.3 Protocols for T1, T2 and T2* weighted imaging were included for structural assessment. Functional imaging protocols utilised gradient echo EPI sequences. Scanner calibration sequences were harmonised for manual calibration. Sequence choice was guided by availability, established use cases, and ability to make required modifications.
Three aspects of the pulse sequences were harmonized: the sequence program, the sequence parameters and preparation radio-frequency pulses. Where possible, the same sequence program was used. Across scanners core sequence parameters were set to be equal. This includes resolution, orientation, timings (TR, TE, TI and echo-spacing), bandwidth, flip-angle, fat-saturation scheme and flow-compensation. Key radiofrequency pulses were matched exactly e.g. the inversion pulse in the MP(2)RAGE sequences.4
No attempt was made to harmonize the parallel acceleration techniques (SENSE on Philips, GRAPPA on Siemens).5,6 Gradient waveforms were not matched precisely.
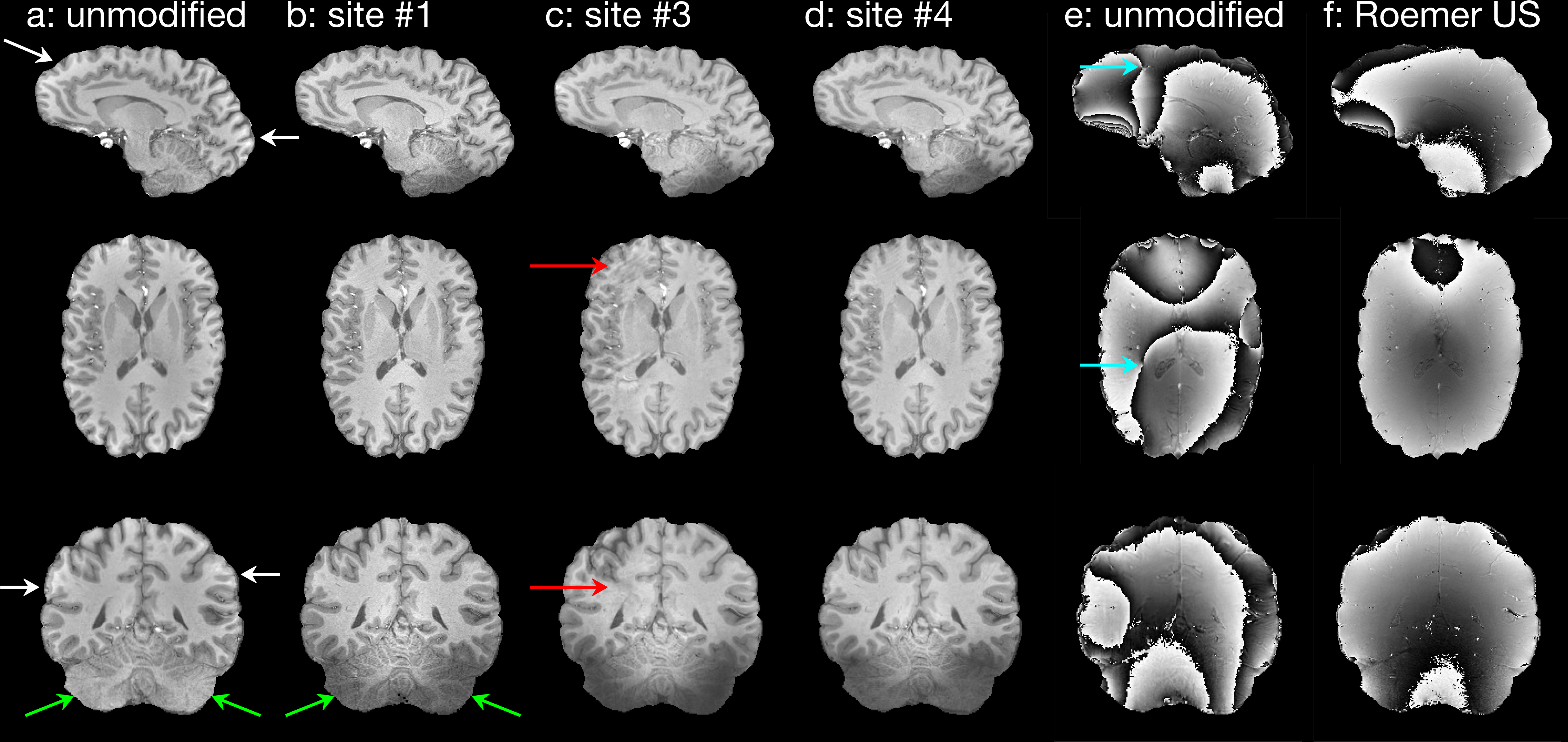
The vendor’s own, or sequence-specific reconstruction was used. For meaningful phase imaging on Siemens systems and to match the Philips SENSE coil combination, a Roemer coil combination algorithm was implemented on the Siemens systems.7
The sequences were run on the same subject (male, 28 years, 82 kg) at all network sites.
The transmit RF calibration was manually harmonized. After the vendor’s calibration, a 3D DREAM sequence measured voxel-wise flip-angles in the subject’s brain.8,9 A whole-brain mean flip-angle was then estimated and used to adjust the transmit calibration before acquiring the rest of the protocol.10
For structural sequences the vendor’s own automatic B0-shimming process was used, iteratively for functional sequences. There was an additional requirement for manual adjustment of shim settings at Sites 4 & 5 (Table 1). The harmonized system calibration of B1+ and B0 was assessed by whole brain dual-echo GE and DREAM in three subjects (male, 31±4 years, 78±7 kg).
Results
The harmonized sequences are listed, and associated parameters are summarised in Table 2. The full sequence parameters and information on any modifications made to the vendor’s default sequences can be found at Ref. 11. The DICOM and NIfTI format data are made available at Ref. 11.
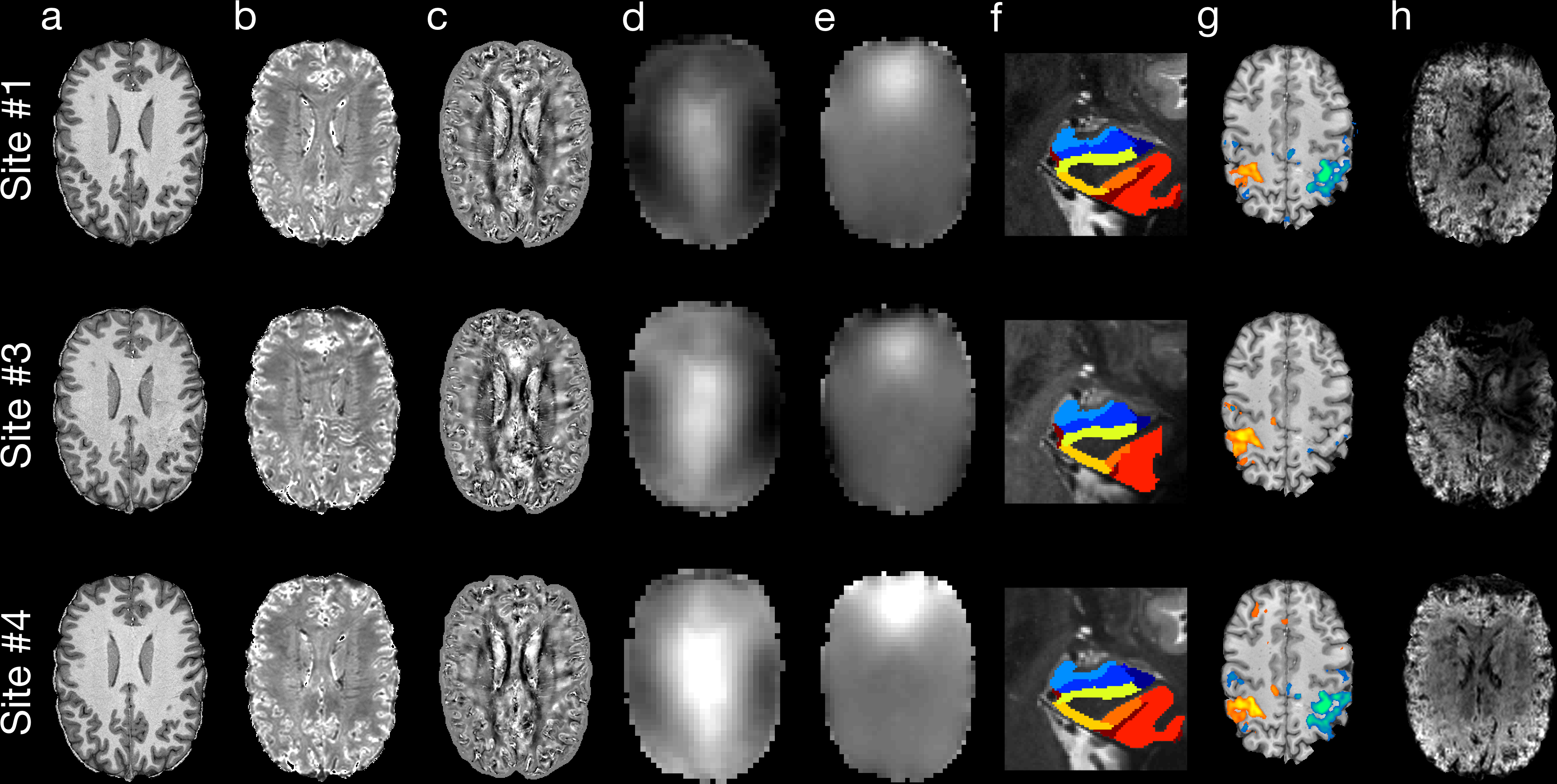
Figure 1 shows results produced using the standard and harmonized MPRAGE sequences. Figure 2 shows the images collected on the single subject from each model of scanner in the Network using the harmonized protocols.
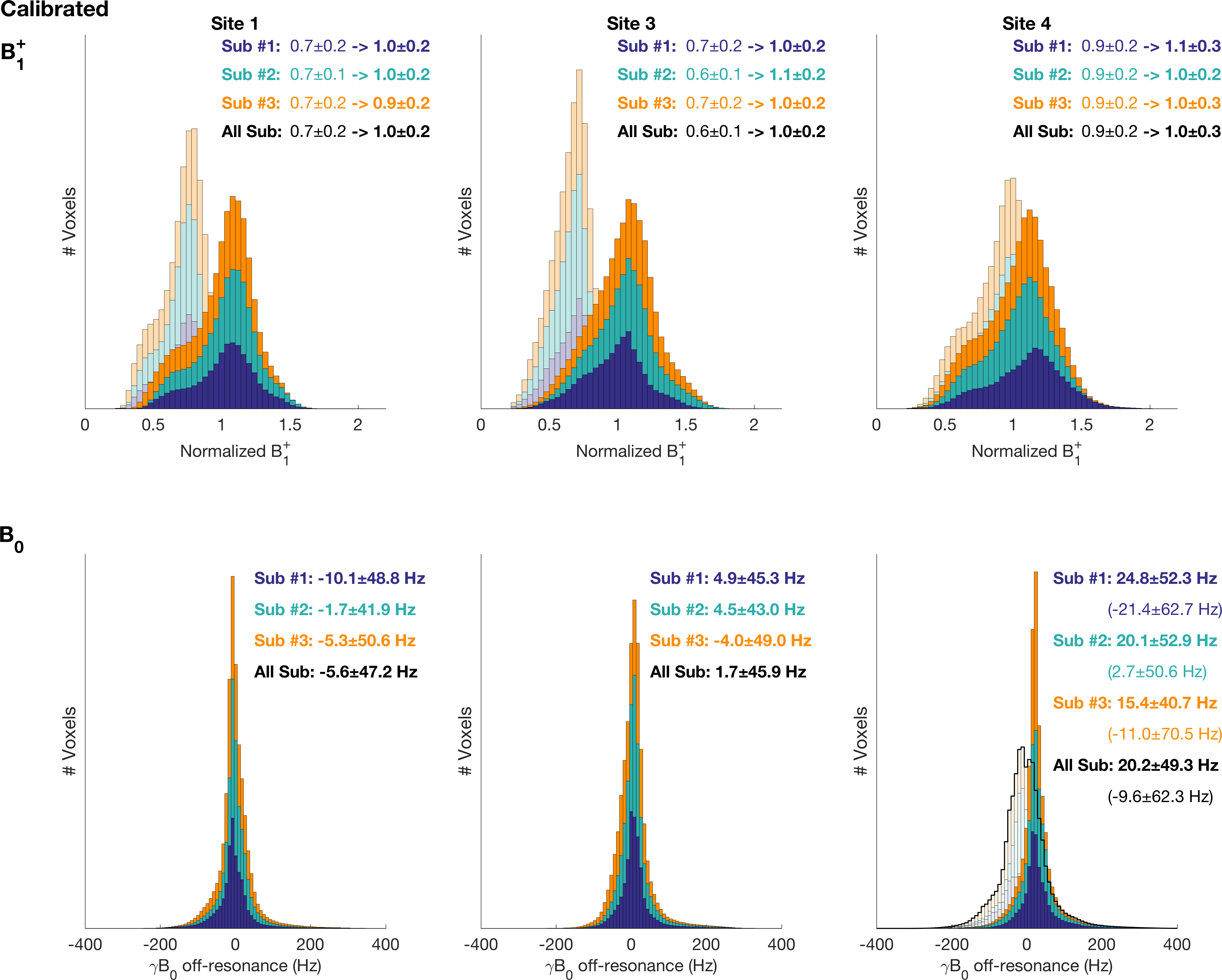
Figure 3 shows the whole-brain distributions of B1+ and B0 measured from three subjects on each model of scanner. The additional transmit calibration was more successful than the vendor’s own at whole-brain calibration (mean of target flip-angle = 0.73 vs. 1.00). Equivalent B0-shimming performance is seen across all models if manual shimming is performed at Site 4 & 5 (B0 standard deviation range: 45.9 -49.3 Hz).
Discussion
These protocols have been implemented to ensure that the UK7T Network’s scanners are able to acquire comparable high-quality data, allowing the possibility of multi-centre patient studies in the future. As the network covers many currently available models of human 7T scanner, the protocols and example data are released for use at other 7T-capable sites.
The efficacy of this harmonization effort is being assessed in an ongoing multi-centre “travelling-heads” study. Data acquisition, comprising scanning the same ten subjects at each site, including repetitions at a designated home site, is complete.
Whilst pulse sequence and reconstruction code were modified for harmonization, it was not feasible to harmonize RF and gradient waveforms and timings precisely, nor all aspects of reconstruction. Complex sequences, such as multi-band EPI were used unmodified on compatible platforms, with just parameters matched. Increasing harmonization increases implementation complexity and results in compromise towards the worst-performing system.
Conclusion
Neuroimaging pulse sequences have been harmonized for the 7T field strength across three different models of scanners from two vendors. The protocols have been made publicly available alongside example datasets from a single subject on each of the UK’s 7T scanners. Manual scanner calibration is essential for harmonized use of different models and sites.Acknowledgements
The UK7T Network and this work was funded by the UK's Medical Research Council (MRC). [MR/N008537/1]. The Wellcome Centre for Integrative Neuroimaging is supported by core funding from the Wellcome Trust (203139/Z/16/Z). CTR is funded by a Sir Henry Dale Fellowship from the Welcome Trust and the Royal Society [098436/Z/12/B].
We thank David Porter for supporting the UK7T Network in using the scanner and facilities at ICE, University of Glasgow.
References
1. Clarke WT, Mougin O, Driver ID, Rua C, Morgan AT, Clare S, Francis S, Wise R, Carpenter A, Muir K, Bowtell RW. The UK7T Network – optimized design of a multi-site, multi-vendor travelling heads study. Proc Intl Soc Mag Reson Med 26 2018:317.
2. Voelker MN, Kraff O, Brenner D, Wollrab A, Weinberger O, Berger MC, Robinson S, Bogner W, Wiggins C, Trampel R, Stocker T, Niendorf T, Quick HH, Norris DG, Ladd ME, Speck O. The traveling heads: multicenter brain imaging at 7 Tesla. MAGMA 2016;29(3):399-415.
3. Trattnig S, Bogner W, Gruber S, Szomolanyi P, Juras V, Robinson S, Zbyn S, Haneder S. Clinical applications at ultrahigh field (7 T). Where does it make the difference? NMR Biomed 2016;29(9):1316-1334.
4. Hurley AC, Al-Radaideh A, Bai L, Aickelin U, Coxon R, Glover P, Gowland PA. Tailored RF pulse for magnetization inversion at ultrahigh field. Magn Reson Med 2010;63(1):51-58.
5. Griswold MA, Jakob PM, Heidemann RM, Nittka M, Jellus V, Wang J, Kiefer B, Haase A. Generalized autocalibrating partially parallel acquisitions (GRAPPA). Magn Reson Med 2002;47(6):1202-1210.
6. Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE: sensitivity encoding for fast MRI. Magn Reson Med 1999;42(5):952-962.
7. Roemer PB, Edelstein WA, Hayes CE, Souza SP, Mueller OM. The NMR phased array. Magn Reson Med 1990;16(2):192-225.
8. Brenner D, Tse DHY, Pracht ED, Feiweier T, Stirnberg R, Stöcker T. 3DREAM – A Three-Dimensional Variant of the DREAM Sequence. 2014; Milan, Italy. p 1455.
9. Nehrke K, Bornert P. DREAM--a novel approach for robust, ultrafast, multislice B(1) mapping. Magn Reson Med 2012;68(5):1517-1526.
10. Clarke WT, Mougin O, Driver ID, Rua C, Francis S, Wise R, Carpenter A, Muir K, Bowtell RW, Clare S. Variability of B1+ and B0 fields in the human brain at 7T. Proc Intl Soc Mag Reson Med 26 2018:4199.
11. Clarke WT. UK7T Network harmonized neuroimaging protocols. University of Oxford; 2018. https://ora.ox.ac.uk/objects/uuid:55ca977f-62df-4cbf-b300-2dc893e36647
12. Yushkevich PA, Pluta JB, Wang H, Xie L, Ding SL, Gertje EC, Mancuso L, Kliot D, Das SR, Wolk DA. Automated volumetry and regional thickness analysis of hippocampal subfields and medial temporal cortical structures in mild cognitive impairment. Hum Brain Mapp 2015;36(1):258-287.
Figures