0244
The developing Human Connectome Project (dHCP): fetal acquisition protocol1Centre for the Developing Brain, School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2Biomedical Engineering Department, King's College London, London, United Kingdom, 3FMRIB, Oxford University, Oxford, United Kingdom
Synopsis
The
developing Human Connectome Project seeks to map connectivity in the human
brain based on structural, functional and diffusion MRI data acquired from over
1000 subjects (neonatal and fetal). A dedicated acquisition protocol has
been developed to efficiently image fetal brain in utero. We describe here the methods and parameters being used
alongside initial pre-processing steps. The acquisition protocol has been tuned
to complement the neonatal data already collected while adapting to the
difficult challenges of imaging the fetal brain in utero. It has been
deployed to image over 145 fetuses to date with a success rate of ~90%.
Introduction
The developing Human Connectome Project (dHCP)1 aims to collect data in over 1000 subjects to create a 4D map of structural and functional connectivity in the human brain from ~20 to 44 weeks gestational age (GA). Neonatal data has already been collected from over 700 subjects and fetal data collection is now underway. We present the dHCP fetal imaging protocol, which has been developed to balance the desire to align closely with the neonatal acquisition, while also addressing the significant added challenges of scanning the fetal brain in utero.Methods
To match the neonates, all data is acquired on a Philips Achieva 3T system (R3.2.2). Subjects are scanned supine using a 32-channel cardiac coil. Sequences were extensively tested and optimised with (local enhanced) safety constraints relevant to in utero scanning paramount; namely, restricting SAR (<50%), PNS (<60%) and acoustic noise (<110dBA).
The fetal exam is divided into two ~30 minute sessions: collection of structural T2w and function (fMRI), then structural T1w and diffusion (dMRI) data. Fetal MRI at 3T presents many challenges, particularly in relation to field inhomogeneity, consequently all modalities utilised localised image-based static field (B0) shimming2, RF shimming and, for functional and diffusion acquisitions, local power scaling. In addition, SENSE and single-band fMRI and dMRI references, dual-TE B0 and DREAM3 B1 maps are collected in both session for calibration purposes.
2D snapshot multi-slice acquisitions are used for all modalities in order to freeze maternal induced motion and spontaneous fetal movements. Parameter values are listed in Table 1.
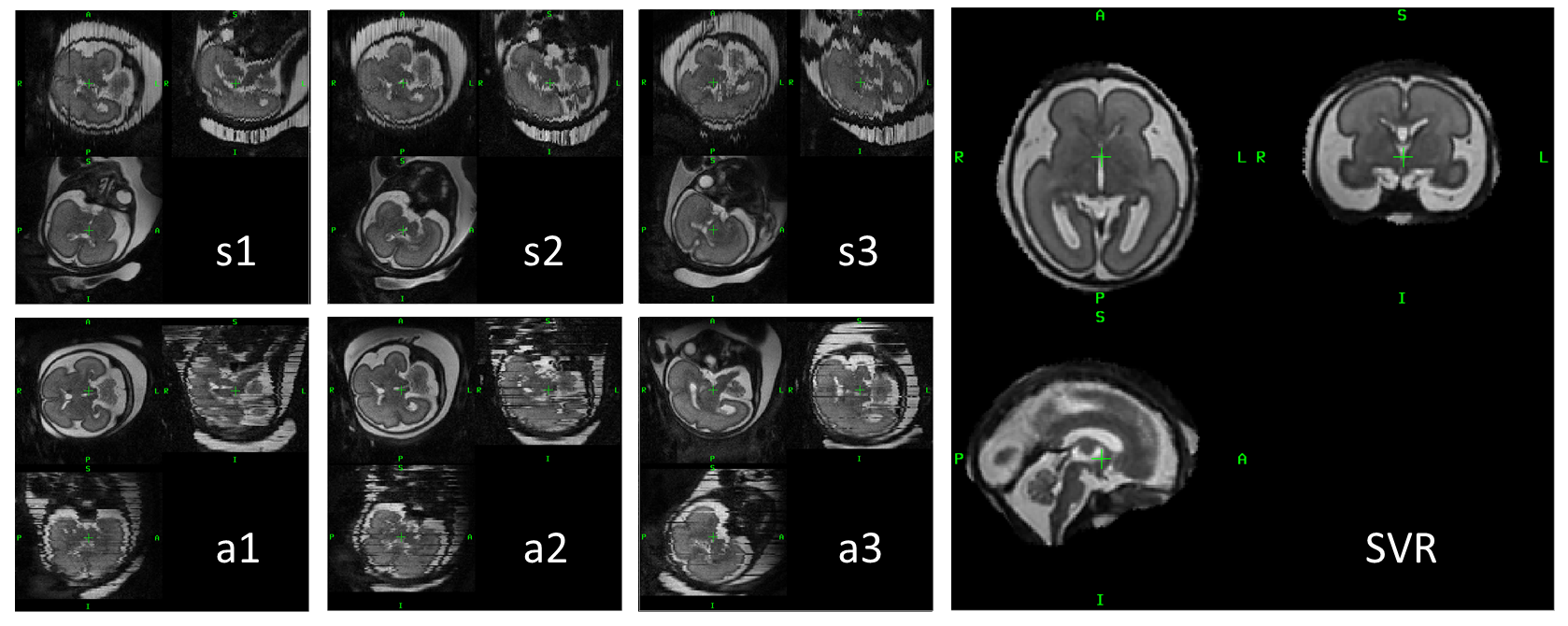
Structural T2w data is acquired from 6 uniquely oriented stacks centred to the fetal brain using a zoomed multiband (MB) single-shot TSE sequence, with a MB tip-back preparation pulse for increased SNR efficiency4.
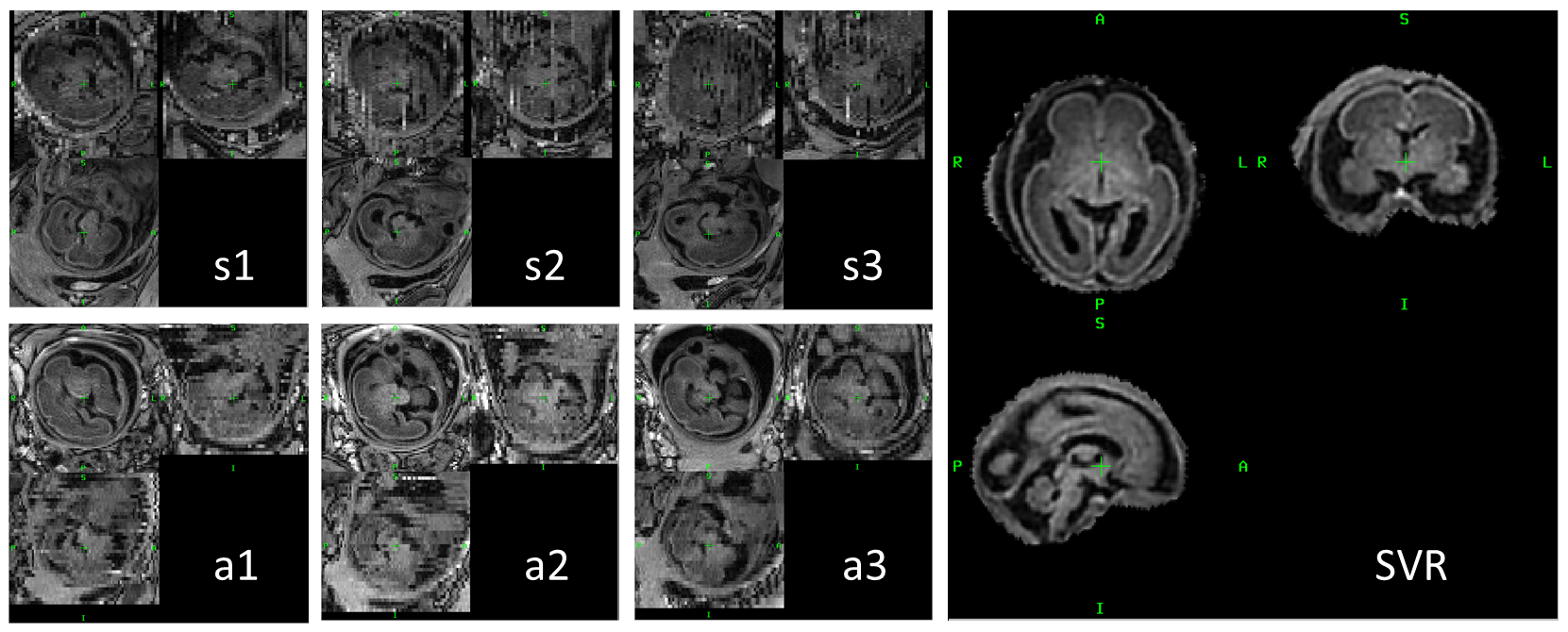
Structural T1w data is collected from 8 stacks at 6 unique views (2 with repeated dynamics) using an inversion-recovery acquisition with interleaved wide-slab preparation pulses to provide increased motion tolerance with optimised contrast5. For the dHCP we have switched to a balanced-SSFP readout, rather than SPGR, to further improve SNR.
Each anatomical dataset is reconstructed to an isotropic 3D volume using slice-to-volume reconstruction (SVR), with automatic rejection of corrupted data6,7.
Functional data collecting 350 volumes utilises MB3 slice acceleration with a SENSE reconstruction8. No in-plane acceleration is used since extended TE benefits the MB-unfolding due to fast decay of maternal tissues in the extended field-of-view, alongside potential enhanced BOLD contrast.
Diffusion data consisting of 141 volumes (15 b=0 s/mm2, 46 b=400 s/mm2, and 80 b=1000 s/mm2, designed using a data-driven method9) is acquired using a spin- and field-echo (SAFE) sequence.
Both
fMRI and dMRI suffer time varying EPI distortion due to B0
disturbance from maternal breathing. The inherent phase of the slice data, for
dMRI combining the spin-echo and field-echo phase information, is used to
estimate dynamic B0 field variation, undistorting the images
shot-by-shot, prior to motion correction10.
Results and discussion
145 subjects (GA range: 21-38 weeks) have been scanned to date, with data completion rates of 94%, 89%, 90% and 91% for T2, T1, fMRI and dMRI, respectively. Work is currently underway to evaluate data quality, initial assessment of T2 reconstructed volume quality rated 80% as 3 or above (0-4 scale).
In figures 1-2 native structural acquired slice stacks are shown in different unique imaging planes (labelled s1-3 and a1-3). The orthogonal views show how data can be miss-aligned due to fetal motion, but a consistent 3D volume is still generated from all data using SVR.
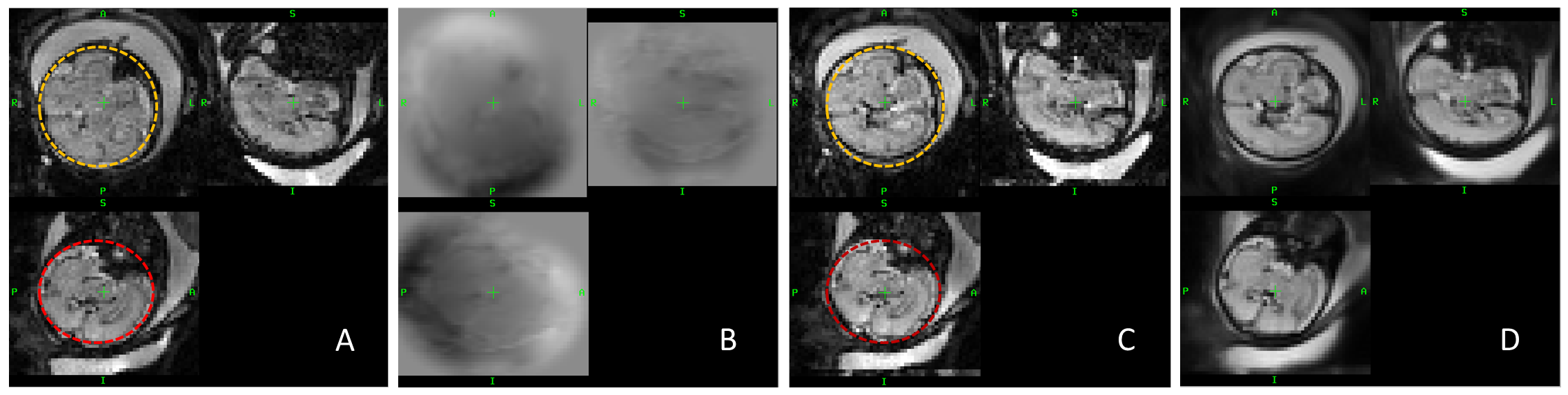
Functional data (Figure 4) is acquired at comparable resolution to neonatal data but limited MB acceleration due to added constraints of maternal field-of-view and coil geometries. As the fetal brain is in a more favourable B0 environment, due to lack of air-interfaces, combining localised higher-order shimming and dynamic distortion correction, has produced reliable results in the majority of subjects.
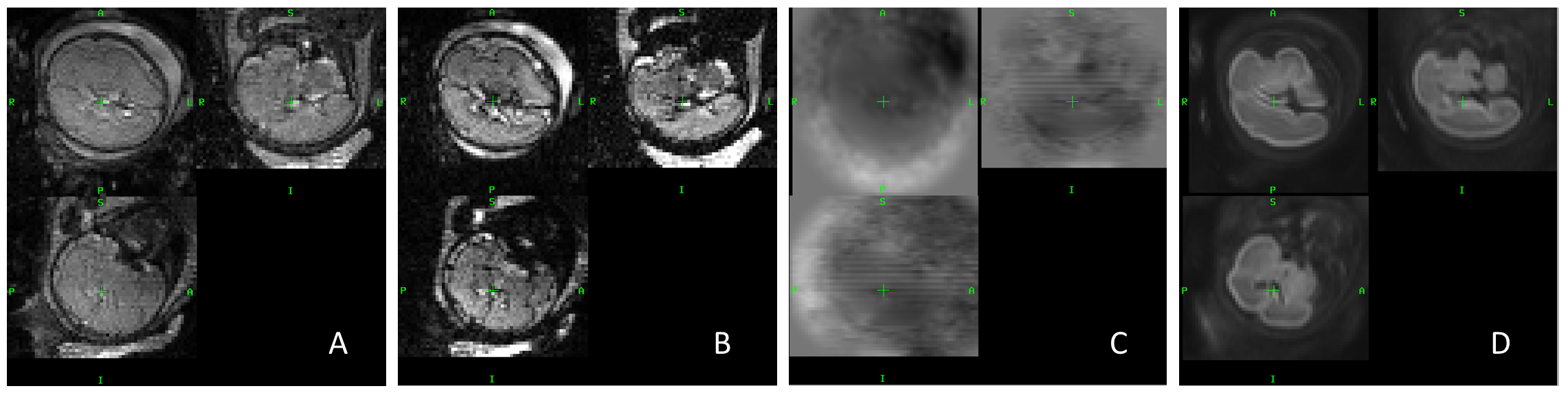
Diffusion
data (Figure 5) traded off MB for in-plane acceleration to shorten TE so
minimising distortion and SNR loss to T2 decay. Conversely, due to
the long T1 times in the fetal brain there is an increased SNR
penalty from extreme shortening of TR, so collection of the second
gradient-echo used for dynamic distortion correction was not a significant time
penalty.
Conclusion
The dHCP fetal protocol has developed from extensive method and parameter testing, to balance the needs of collecting data aligned to the neonatal acquisition, while also being constrained by the significant challenges of fetal motion and increased safety considerations. This data along with the neonatal cohort will be made freely available once acquisition is complete.Acknowledgements
This work received funding from the European Research Council under the European Union’s Seventh Framework Programme (FP7/20072013)/ERC grant agreement no. 319456 (dHCP project), and was supported by the Wellcome EPSRC Centre for Medical Engineering at Kings College London (WT 203148/Z/16/Z), MRC strategic grant MR/K006355/1 and by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.References
1. The developing Human Connectome Project (dHCP). www.developingconnectome.org.
2.
Gaspar AS, Nunes
RG, Ferrazzi G, Hughes EJ, Hutter J, Malik SJ, McCabe L, Baruteau KP, Rutherford
MA, Hajnal JV, Price AN. Optimizing maternal fat suppression with constrained
image‐based shimming in
fetal MR. MRM 2018: 10.1002/mrm.27375.
3. Nehrke K, Börnert P. DREAM—A Novel Approach for Robust, Ultrafast, Multislice B1 Mapping. MRM. 2012;68:1517–26.
4. Price AN, Cordero-Grande L, Malik SJ, and Hajnal JV. “Multiband zoom TSE Imaging: increasing efficiency with multiband tip-back pulses”. Proc. Intl. Soc. Mag. Reson. Med. 26 (2018) 0062.
5. Ferrazzi G, Price AN, Teixeira RPAG, Cordero-Grande L, Hutter J, Gomes A, Padormo F, Hughes E, Schneider T, Rutherford M, Kuklisova Murgasova M, Hajnal JV. An efficient sequence for fetal brain imaging at 3T with enhanced T1 contrast and motion robustness. MRM, 2017. 10.1002/mrm.27012
6. Jiang S, Xue H, Glover A, Rutherford M, Rueckert D, Hajnal JV. MRI of moving subjects using multislice snapshot images with volume reconstruction (SVR): application to fetal, neonatal, and adult brain studies. IEEE TMI. 2007; 26(7):967–980.
7. Kuklisova-Murgasova M, Quaghebeur G, Rutherford MA, Hajnal JV, Schnabel JA. Reconstruction of fetal brain MRI with intensity matching and complete outlier removal. Med Image Anal. 2012:16(8) 1550-1564.
8. Zhu K, Dougherty RF, Wu H, Middione MJ, Takahashi AM, Zhang T, Pauly JM, Kerr AB. Hybrid-Space SENSE Reconstruction for Simultaneous Multi-Slice MRI. IEEE Trans Med Imag. 2016. 35(8):1824-1836.
9. Tournier J-D, Hughes E, Tusor N, Sotiropoulos SN, Jbabdi S, Andersson J, Rueckert D, Edwards AD, Hajnal JV. Data-driven optimisation of multi-shell HARDI. Proc. Intl. Soc. Mag. Reson. Med. 23 (2015) 2897.
10. Cordero-Grande L, Price AN, Ferrazzi G, Hutter J, Christiaens D, Hughes E, Hajnal JV. Spin And Field Echo (SAFE) dynamic field correction in 3T fetal EPI. Proc. Intl. Soc. Mag. Reson. Med. 26 (2018) O208.
11.
Christiaens D, Cordero-Grande L, Pietsch M,
Hutter J, Edwards AD, Deprez M, Hajnal JV, Tournier J-D. Multi-shell SHARD
reconstruction from scattered slice diffusion MRI data in the neonatal brain.
ISMRM 2018; 26:O464.
Figures
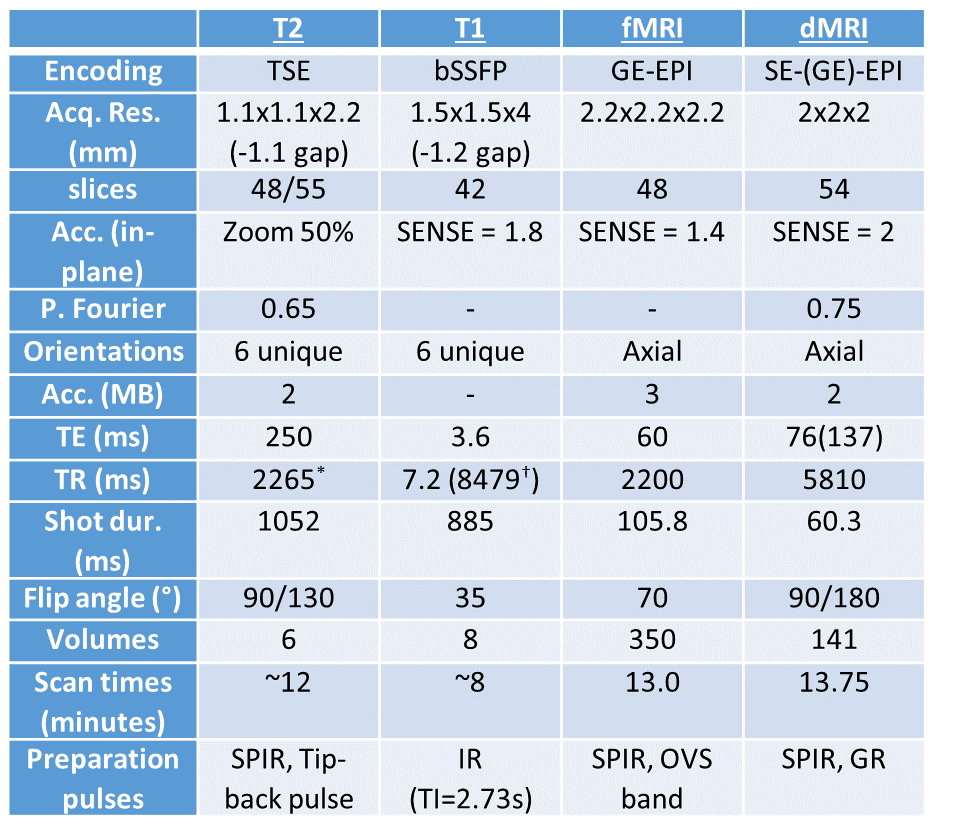
Table 1: Native acquisition parameters for core fetal dHCP protocol.
*Minimum TR, increase possible with certain RF shims. †Slice package duration (effective TR for slab selective IR pulse).
SPIR: spectrally-selective inversion recovery (fat-sat), OVS: outer volume suppression, GR: gradient reversal (of refocus slice selection) PO: power optimisation.