0228
Towards robust free-breathing cardiac DTI1MRC/UCT Medical Imaging Research Unit, University of Cape Town, Cape Town, South Africa, 2Cape Universities Body Imaging Centre (CUBIC-UCT), University of Cape Town, Cape Town, South Africa, 3Oxford Centre for Clinical Magnetic Resonance Research (OCMR), University of Oxford, Oxford, United Kingdom, 4Department of Medicine, University of Cape Town, Cape Town, South Africa, 5Hatter Institute for Cardiovascular Research in Africa, University of Cape Town, Cape Town, South Africa
Synopsis
A prospective respiratory motion correction control system, capable of performing of slice tracking, was implemented in a spin echo diffusion weighted sequence to perform free-breathing acquisitions. The performance of the motion correction control system was compared against common respiratory motion compensation techniques, namely breath-holds, respiratory gating, and standard slice tracking. The values of all the free-breathing techniques varied from the breath-hold data, however, the motion correction control system produced very consistent results. The slice tracking methods were able to significantly reduce the acquisition time (by 50%), compared to the respiratory gating technique.
Introduction
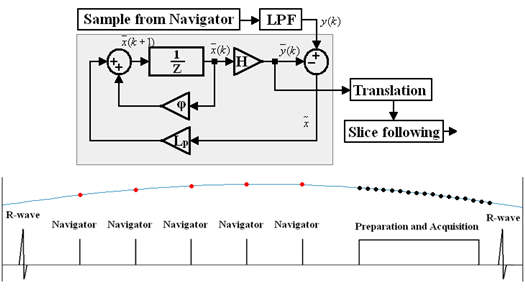
Previously a prospective respiratory motion correction control system was used to perform in vivo slice tracking of the heart1. The control system is based on an adaptive Kalman
filter and can update the slice position throughout the imaging segment by using samples from multiple respiratory navigators to perform slice tracking2 (see Figure 1). Cardiovascular diffusion tensor imaging (cDTI) is an emerging technique that may have clinical utility in assessing and quantifying microstructural changes in the heart3,4. Its utility has been hampered by long scan times particularly due to multiple, long breath-holds. These breath-holds may present a significant challenge to patients3. The ability to perform cDTI acquisitions under free-breathing conditions may improve its clinical utility, allowing more diffusion directions and more accurate quantitation. Common free-breathing techniques used are respiratory gating with an acceptance window5 (long scan times due to reduced respiratory efficiency); and navigator slice tracking which updates the slice position once prior to the imaging segment6 (slice position becomes progressively outdated). The motion correction control system was implemented and tested in a second-order motion compensated spin echo (M2SE) diffusion sequence.Methods
Four healthy volunteers were scanned in a 3-Tesla Prisma (Siemens, Erlangen, Germany). Four DTI datasets were acquired using the M2SE sequence coupled with four respiratory compensation techniques: multiple breath-holds, standard respiratory gating with a ±5 mm acceptance window (gated), standard respiratory navigators with slice tracking, and a modified respiratory navigated sequence with the prospective motion correction control system to perform slice tracking. Four different b-values with 6 diffusion directions were collected: $$$\small{350\text{,}\:{}450\text{,}\:{}550}$$$, and $$$\small{650\:{}\text{s/mm}^2}$$$. All acquisitions were repeated eight times. The sequence parameters used were: TR/TE $$$\small{1000/60\:{}\text{ms}}$$$; matrix size $$$\small{128\times{}48}$$$; interpolated pixel spacing $$$\small{1.4\times{}1.4\:{}\textrm{mm}^2}$$$; slice thickness $$$\small{8\:{}\textrm{mm}}$$$; bandwidth $$$\small{2440\:{}\textrm{Hz/pixel}}$$$; GRAPPA $$$\small{2}$$$. Cine images were used to position the slice in the middle region of the heart and to optimise the trigger delay so that end-systole occurred during the readout. Each exam was initially performed under breath-hold conditions, with 24 breath-holds of approximately 8 seconds each, and then free-breathing for the remainder of the exam. For the standard gated, standard slice tracking and control system slice tracking sequences, all b-values and repetitions were collected in one continuous scan. The acquisition time of the gated sequence was 7-12 minutes (mean: 10 minutes) with a respiratory efficiency of 40-80% (mean: 60%), while the acquisition time of both slice tracking sequences were 3-6 minutes (mean: 5 minutes) and had 100% respiratory efficiency.
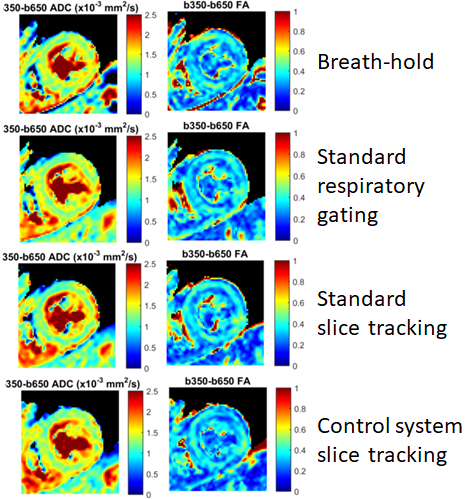
An in-house MATLAB post-processing tool was used to analyse the images7. Images were heart-rate corrected for T1 recovery during the varying R-R intervals except for the gated images because of uncertainty over the tissue location in-between acceptance windows. Images were then registered together using simple, rigid transformations. The apparent diffusion coefficient (ADC) and fractional anisotropy (FA) were calculated, using $$$\small{b_{ref}=350\,{}\text{s/mm}^2}$$$ as the reference b-value to reduce perfusion effects (Figure 2). These results were compared using a linear mixed model to account for multiple measurements per subject; inter-subject variability was quantified using the standard deviations.
Results
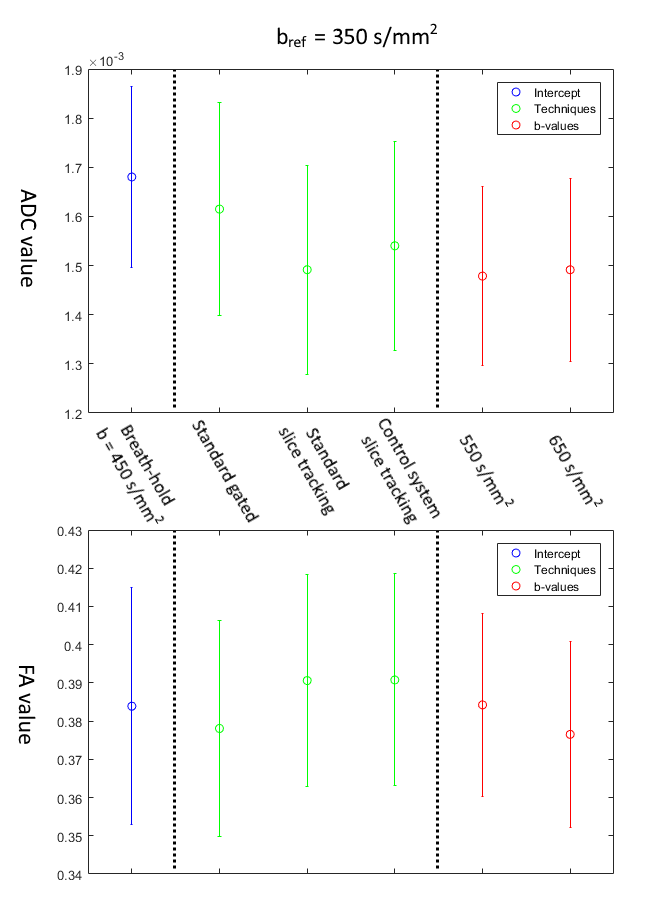
Figure 3 shows the results of the linear mixed-effect model. No significant differences were found in the $$$\small{b_{ref}=350\,{}\textrm{s/mm}^2}$$$ datasets in either the ADC or FA values.
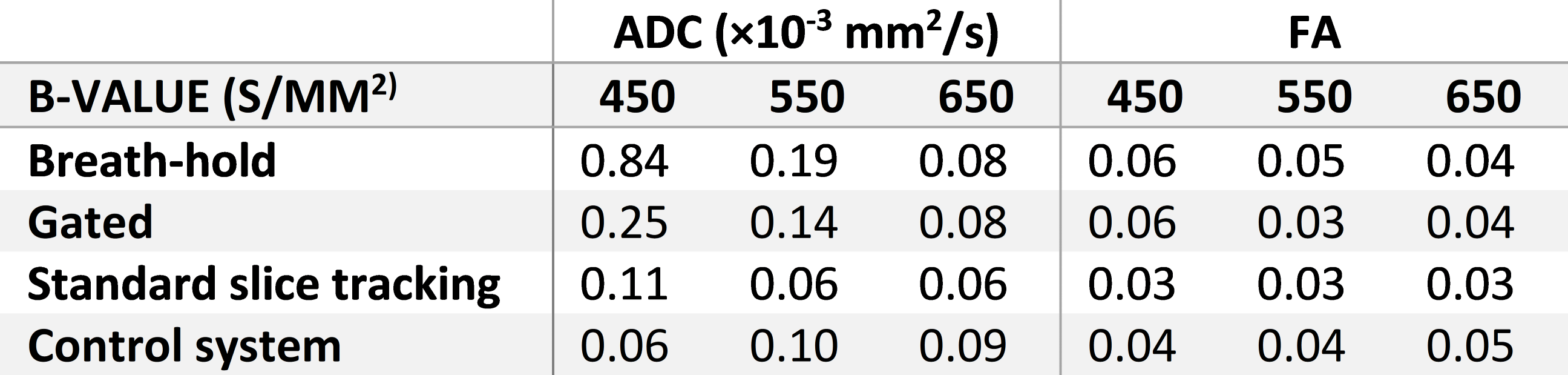
The inter-subject variability (Figure 4) was low for both reference b-values, meaning all the techniques produced a narrow range of results. However, both the standard slice tracking and the control system slice tracking sequences had lower variation in ADC values than the breath-hold and gated techniques.
Discussion
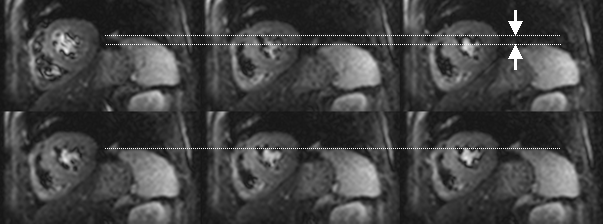
Both the standard and control system techniques were able to satisfactorily track the position of the slice during free-breathing (Figure 5).
The linear mixed-effect model showed that there was good agreement between all respiratory compensation techniques and b-values.
While all the techniques produced a narrow range of ADC and FA values, both navigated techniques had low inter-subject variation indicating the ability of the control system navigated sequence to give consistent results across subjects.
Conclusion
The prospective respiratory motion correction control system performed comparably to other free-breathing techniques as well as breath-holding, giving similarly consistent results. The slice tracking techniques were able to reduce the length of the acquisition by 50% due to the 100% respiratory efficiency. The prospective respiratory motion correction control system may be useful in improving the viability of cDTI in a clinical setting by allowing acquisitions to take place under free-breathing conditions.Acknowledgements
NRF/RCUK Newton Fund collaboration between the University of Oxford and the University of Cape Town
NRF/DST South African Research Chairs Initiative
E.M. Tunnicliffe is funded by the NIHR Oxford Biomedical Research Centre
A.T. Hess acknowledges support from the British Heart Foundation Oxford Centre of Research Excellence
References
1. Jermy, S. G., Alhamud, A., Burger, I. H., et al. Implementation of a control system for prospective respiratory motion correction during Cardiovascular MR imaging. Proc. ISMRM 26, 2018. (#4112)
2. Burger, I. H., Keegan, J., Meintjes, E. M., et al. Prospective diaphragm position prediction for Cardiac MR using multiple navigators. Proc ISMRM-ESMRMB 18, 2010. (#5013)
3. Mekkaoui, C., Reese, T. G., Jackowski, M. P., et al. (2017). Diffusion MRI in the heart. NMR in Biomedicine. 30(3).
4. Ferreira, P. F., Kilner, P. J., McGill, L. A., et al. (2014). In vivo cardiovascular magnetic resonance diffusion tensor imaging shows evidence of abnormal myocardial laminar orientations and mobility in hypertrophic cardiomyopathy. Journal of Cardiovascular Magnetic Resonance. 16(1):87.
5. Stoeck, C.T., von Deuster, C., Genet, M., et al. (2015). Second order motion compensated spin-echo diffusion tensor imaging of the human heart. Journal of Cardiovascular Magnetic Resonance. 17(Suppl 1):1–3.
6. Moulin, K., Croisille, P., Feiweier, T., et al. (2016). In vivo free-breathing DTI and IVIM of the whole human heart using a real-time slice-followed SE-EPI navigator-based sequence: A reproducibility study in healthy volunteers. Magnetic Resonance in Medicine. 76(1):70–82.
7. Tunnicliffe, E. M., Scott, A. D., Ferreira, P., et al. (2014). Intercentre reproducibility of cardiac apparent diffusion coefficient and fractional anisotropy in healthy volunteers. Journal of Cardiovascular Magnetic Resonance. 16(1):31.
Figures