0198
The effects of neoadjuvant chemotherapy on axillary lymph node volume and compacity in breast cancer patients: an MRI study1Stony Brook University, Stony Brook, NY, United States
Synopsis
Axillary lymph node involvement in breast cancer is associated with higher risk of distant metastasis and recurrence. This study evaluated whether MRI can be used to longitudinally monitor effects of neoadjuvant chemotherapy on axillary lymph nodes in situ. Nodal volume and compacity were analyzed with respect to treatment responders and non-responders. Comparisons with unaffected nodes were made. Neoadjuvant chemotherapy significantly reduced nodal volume of the affected nodes in both responders and non-responders. Nodal volumes of the responders normalized whereas those of the partial-responders did not normalize completely. This approach may prove useful for monitoring cancer treatment effects on nodal morphology.
Introduction
Breast tumor volume is monitored in assessment of response to neoadjuvant chemotherapy (NAC) [1]. Longitudinal monitoring of axillary lymph nodes (aLN) is more challenging, but remains important for prognosis and treatment planning. Methods of aLN interrogation include palpation, ultrasound, FDG-PET, sentinel biopsy and dissection. Palpation and ultrasound are limited to larger, superficial aLNs and is non-quantitative. FDG-PET imaging involves injection of radionuclide. aLN biopsy and dissection are invasive. Reliable non-invasive imaging approach enabling longitudinal monitoring on all aLNs in situ would be useful.
The goal of this study was evaluation of MRI for longitudinal monitoring of aLN NAC-related effects in breast cancer patients. aLN volume and compacity were analyzed with respect to treatment response. Comparisons with unaffected nodes were made.
Methods
143 locally advanced breast cancer patients pre- and post-NAC were studied. aLNs were manually segmented on first post-contrast (~2.5 minutes) 1.5 T MR T1-weighted image with high resolution (<1mm in-plane, <2.5 mm slice thickness). Results of average axilla and largest node per patient were similar so only average aLN values are reported. The number of nodes (sample sizes) ranged from 62 to 80 per group (see Table). LifexSoft was used to obtain volume and shape features. Compacity was defined as Area3/2/Volume. Comparisons were made between contralateral (normal) nodes, ipsilateral non-responders and responders. Responder was defined as having no residual invasive nodal disease after NAC. Two-tailed t-test with unequal variance tested for significant difference between groups (p-value<0.05=significant).Results
Figure 1 shows representative MRI of ipsilateral and contralateral aLNs for a complete responder and non-responder. The ipsilateral aLNs showed marked differences in both size and shape after NAC. The size of the ipsilateral aLN was reduced and the margin of the nodes became more uniform.
VOLUME: Figure 2 and Table 1 shows aLN volume pre- and post-NAC of contralateral unaffected and ipsilateral nodes. NAC markedly reduced the ipsilateral nodal volumes in non-responders (2.58±3.29 mL vs 0.77±0.83 mL, p<0.00001) and responders (2.33±4.56 mL vs 0.45±0.37 mL, p<0.001). Responder nodes were also significantly smaller than non-responder nodes post-NAC (p<0.003). Additionally, non-responder nodes remained significantly larger than contralateral nodes post-NAC (p<0.05) whereas responder nodes normalized when compared to the contralateral nodes (p>0.05).
Pre-NAC, volume standard deviations of contralateral nodes were large (~60% of mean), suggesting large inter-subject variability in node sizes. Standard deviations of ipsilateral affected nodes pre-NAC were even larger (~130% of mean), suggesting even larger inter-subject variability. Post-NAC, the volume standard deviations normalized significantly.
SHAPE: Figure 3 and Table 2 shows the results of nodal compacity pre- and post-NAC of contralateral unaffected and ipsilateral nodes. NAC reduced ipsilateral nodal compacity in non-responders (1.18±0.77 to 1.16±0.47, p<10-8) and responders (1.17±0.77 vs 1.04±0.34, p<10-8). Post-NAC compacity of ipsilateral nodes between responder and non-responder showed a trend toward significance (p=0.09), with responders having average compacity closer to contralateral normal nodes.
Pre-NAC, standard deviation of compacity for ipsilateral nodes is 2.5 times higher than contralateral nodes, suggesting large inter-subject variability in shape of affected nodes. Post-NAC, standard deviations of ipsilateral node became smaller, suggesting normalization.
Discussion
MRI is the modality of choice for monitoring tumor response to NAC with tumor size and shape changes correlated to pathological response [2]. aLNs are modulated by NAC but common methods of assessment (palpation and ultrasound) are non-quantitative and limited to relatively large surface nodes. Changes in nodal morphology detected by ultrasound after NAC is correlated with higher pathological complete response rate [3]. MRI can measure 3D volume of aLNs, is sensitive to detect changes and has potential to distinguish responders and non-responders to NAC [4]. The current spatial resolution is 0.00098 mL per voxel; some aLNs are small (~0.05 mL or 55 voxels) and cannot be quantified reliably and/or hilum cannot be visualized at current resolution. Future studies will need to increase spatial resolution to detect small nodes.
When comparing aLN volume and compacity, aLN volume is better in distinguishing between responders and non-responders, although further study is needed. In other studies, compacity differentiated benign and malignant breast lesions [5] and aLNs [6]. More sophisticated approaches (texture analysis/optimized MRI sequences) should be explored to investigate normalization of shape and size features.
Conclusions
MRI can be used to longitudinally and non-invasively monitor the effects of neoadjuvant chemotherapy on aLNs volume and shape in situ in breast cancer patients. Neoadjuvant chemotherapy significantly reduced nodal volume of the affected nodes in both responders and non-responders. Nodal volumes of the responders normalized completely, whereas partial-responders or non-responders did not. This approach may prove useful for monitoring cancer treatment effects on aLN morphology.Acknowledgements
No acknowledgement found.References
[1] Hylton NM et al. Neoadjuvant Chemotherapy for Breast Cancer: Functional Tumor Volume by MR Imaging Predicts Recurrence-free Survival-Results from the ACRIN 6657/CALGB 150007 I-SPY 1 TRIAL. Radiology. 2016 Apr;279(1):44-55. doi: 10.1148/radiol.2015150013. Epub 2015 Dec 1.
[2] Fan M et al. Radiomic analysis of DCE-MRI for prediction of response to neoadjuvant chemotherapy in breast cancer patients. Eur J Radiol. 2017 Sep;94:140-147. doi: 10.1016/j.ejrad.2017.06.019. Epub 2017 Jun 28.
[3] Alvarado R et al. The role for sentinel lymph node dissection after neoadjuvant chemotherapy in patients who present with node-positive breast cancer. Ann Surg Oncol. 2012 Oct;19(10):3177-84. doi: 10.1245/s10434-012-2484-2. Epub 2012 Jul 7.
[4] Maxwell F et al. Diagnostic strategy for the assessment of axillary lymph node status in breast cancer. Diagn Interv Imaging. 2015 Oct;96(10):1089-101. doi: 10.1016/j.diii.2015.07.007. Epub 2015 Sep 12.
[5] Nie K et al. Quantitative analysis of lesion morphology and texture features for diagnostic prediction in breast MRI. Acad Radiol. 2008 Dec;15(12):1513-25. doi: 10.1016/j.acra.2008.06.005.
[6] Fusco R et al. Use of Quantitative Morphological and Functional Features for Assessment of Axillary Lymph Node in Breast Dynamic Contrast-Enhanced Magnetic Resonance Imaging. Biomed Res Int. 2018 May 30;2018:2610801. doi: 10.1155/2018/2610801. eCollection 2018.
Figures
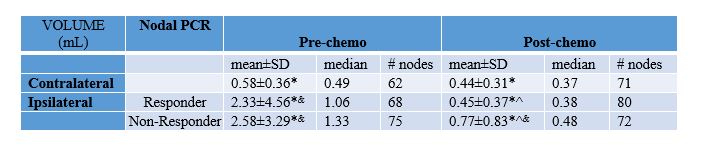
Table 1. Pre and post-NAC average aLN volumes of contralateral, ipsilateral non-responders and ipsilateral responder.
* significantly different between pre- and post-chemo
& significantly different from contralateral at that time point
^ significantly different between responders and non-responders
NAC: neoadjuvant chemotherapy, aLN: axillary lymph node, PCR: pathological complete response

Table 2. Pre and post-NAC average aLN compacity of contralateral, ipsilateral non-responders and ipsilateral responder.
* significantly different between pre- and post-chemo
& significantly different from contralateral at that time point
^ significantly different between responders and non-responders
NAC: neoadjuvant chemotherapy, aLN: axillary lymph node, PCR: pathological complete response
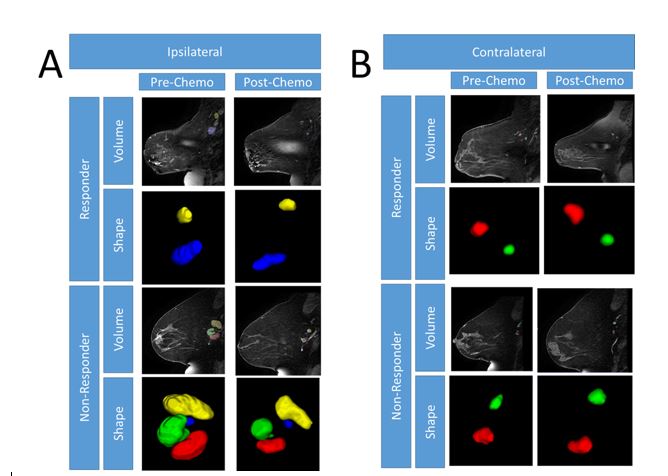
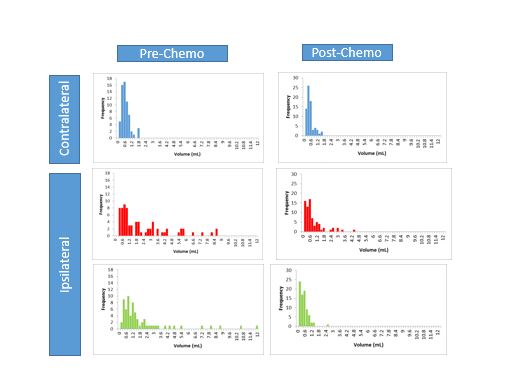
Figure 2. Pre and post-NAC average aLN volumes of contralateral (blue), ipsilateral non-responders (red) and ipsilateral responder (green).
NAC: neoadjuvant chemotherapy, aLN: axillary lymph node,
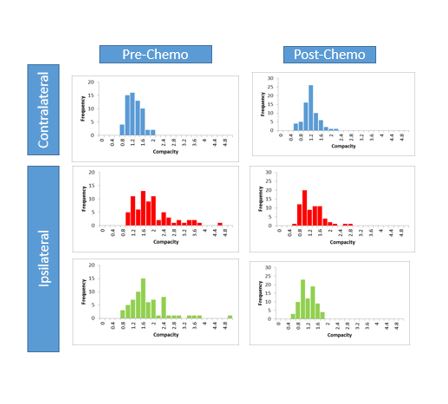
Figure 3. Pre and post-NAC average aLN compacity of contralateral (blue), ipsilateral non-responders (red) and ipsilateral responder (green).
NAC: neoadjuvant chemotherapy, aLN: axillary lymph node,